Langerhans Cell Histiocytosis (LCH) of the Spine
- Background:
- LCH comprises a rare group of disorders with a wide range of clinical presentations.
- It is characterized by abnormal accumulation of histiocytes in different tissues, but the etiology remains unknown
- LCH is more common in children and adolescents.
- Bone is the most common site affected, with a predilection for the axial squeleton.
- Relevant Clinical Information: Pain, neurologic deficits, restricted motion, deformity. Some patients may be asymptomatic.
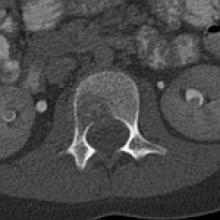
- Key Diagnostic Features:
- Solitary or multiple lytic lesions, round or oval, with poor or well defined margins in plain radiographs
- CT depicts expansive lytic bone destruction that may have a geographic pattern and soft tissue masses. Limited sclerosis is seen during the healing stage.
- On MRI most lesions have low-to-intermediate signal intensity on T1WI, intermediate-to-high on T2WI, and they enhance avidly with contrast.
- Other findings include edema, paravertebral soft tissue components, and peridural compression.
- Vertebra plana may be seen on all these imaging modalities.
- DDx:
- Ewing sarcoma
- More likely to have large soft tissue mass, permeative bone destruction and relative hypointense in T2
- Lymphoma
- Multiple levels, ivory vertebral body, hypointense-to-normal marrow
- Metastatic neuroblastoma
- Multiple osteosclerotic lesions
- Discitis-osteomyelitis
- Hyperintense narrow disc with or without fluid signal
- Ewing sarcoma
- Treatment Options: For monostotic disease, treatment includes observation, injection of corticosteroids, nonsteroidal anti-inflammatories, and surgical curettage.