
Abstract
BACKGROUND AND PURPOSE: Although sonographic evaluation of cervical adenopathy by use of size criteria is effective, the sensitivity and specificity fall short of that required to make adequate judgments regarding neck dissection. Therefore, we tested whether the combined use of size criteria and Doppler sonographic findings would improve the predictive ability for metastatic cervical nodes.
METHODS: We analyzed 338 histologically proved cervical lymph nodes (108 metastatic and 230 nonmetastatic) in 73 patients with head and neck cancer. The sonographic topography of the nodes was compared with dissected specimens, and their position in the neck was categorized into three levels (I, II, and III+IV). The diagnostic accuracy of sonography was evaluated by using the single criterion of short-axis diameter of the node or by the combined criteria of short-axis diameter and Doppler blood flow features (the absence or presence of normal hilar flow).
RESULTS: As compared with the single criterion of short-axis nodal diameter, the combined criteria of nodal size and Doppler blood flow patterns increased the diagnostic accuracy of sonography at all levels in the neck. Accordingly, the best cut-off values were improved to 6, 7, and 5 mm for nodes at levels I, II, and III+IV, respectively. In addition, the combined criteria yielded high sensitivites (≥89%) and specificities (≥94%).
CONCLUSION: Hilar blood flow information obtained by Doppler sonography significantly improves diagnostic accuracy for the detection of nodes metastatic from head and neck squamous cell carcinoma.
Advancements in imaging techniques such as helical CT, MR imaging, and high-resolution sonography (1–5) have improved the detection of metastatic cervical nodes in patients with head and neck cancer. Accordingly, several investigators have attempted to determine reliable criteria for detecting these nodes. One of these is the criterion of size. Most recently, van den Brekel et al (6) refined the previously reported size criteria for assessing metastatic cervical nodes with cross-sectional techniques. Other studies with CT and MR imaging have shown that interpretive criteria on CT studies, including size, are superior to those on MR studies (7, 8), and that the criterion of nodal size yielded high predictive values only when short-axis diameters of 10 mm or more were used (8).
Doppler sonography has recently been proposed as an additional tool for the detection of metastatic cervical nodes (9, 10). Parenchymal (or peripheral) blood flow, as depicted by Doppler sonography, is one of the most predictive criteria for metastatic nodes. Nevertheless, a substantial number of metastatic and nonmetastatic nodes have been shown to exhibit an avascular pattern on Doppler sonograms (9). Thus, Doppler characteristics may be less accurate than nodal size (ie, short-axis diameter) in predicting metastatic nodes. In contrast, the presence of normal hilar flow on Doppler sonograms was highly suggestive of nonmetastatic nodes (11). These studies may indicate that the absence of normal hilar flow is the most, if not only, reliable Doppler criterion in the diagnosis of metastatic nodes. Therefore, we hypothesized that the combined criteria of nodal size, as determined by short-axis diameter, and absence of normal hilar flow on Doppler sonograms could improve the predictive ability of sonography for metastatic nodes.
Cervical lymph nodes may be classified into several groups on the basis of their anatomic location in the neck (12). A number of studies have confirmed the notion that enlarged nodes at different levels require different size criteria for predicting metastatic nodes. For example, Curtin et al (8) assessed the predictive value of size criteria by CT and MR imaging in cervical nodes that were classified into three anatomic levels. Furthermore, van den Brekel et al (6) showed that, among nodes at different levels, different cut-off values for size criteria were required for the best combination of sensitivity and specificity. In these two studies, however, the topographic correlation between images and dissected nodes was performed by level, not by node. In addition, no evaluation was performed with respect to Doppler sonographic criteria in relation to anatomic location of the nodes. Therefore, after topographic correlation by node in patients with head and neck cancer, we tested whether a combination of size and Doppler sonographic criteria could improve the predictive ability for metastatic cervical nodes.
Methods
Patients
We retrospectively reviewed the sonographic features of 338 histologically proved cervical lymph nodes in 73 patients with head and neck cancer. The study group included 20 women with an average age of 68 years (age range, 47–85 years) and 53 men with an average age of 61 years (age range, 35–80 years). All 73 patients had neck dissections. The primary sites of the lesions were the oral mucosa (42 squamous cell carcinomas), the pharynx (19 squamous cell carcinomas: 11 hypopharynx, four nasopharynx, and four oropharynx), and the larynx (12 squamous cell carcinomas).
Sonographic Examination
Gray-scale and power Doppler sonography were performed using a Logiq 700 unit (General Electric Yokogawa Medical Systems, Tokyo, Japan) equipped with a wide bandwidth (range, 6–13 MHz) transducer. Gray-scale sonography was performed at 10 MHz. Power Doppler sonography was performed at 8 MHz, and standardized Doppler settings were chosen to optimize detection of the signals from the lymph node vessels, which had low-velocity flow. Common settings for pulse repetition frequency (500 Hz) and for the wall filter (75 or 62 Hz) were used. Representative images by gray-scale and power Doppler sonography were obtained from each lymph node so that the maximal area of the node appeared on the sonograms, with an axial orientation to the neck.
Comparison between Dissected Lymph Nodes and Sonograms
Topographic correlation between dissected nodes and sonograms was performed node by node by using a reporting system as described previously (9). The report included data concerning the approximate location relative to the surrounding anatomic structures, such as vessels and muscles, and the size of the enlarged nodes on sonograms. At surgery, the lymph nodes were excised en bloc along with the adjacent reference structures to ascertain more easily the spatial relationship between the excised nodes and surrounding structures, such as muscles, salivary glands, and veins. The size of the node was also compared with the sonographic findings. Surgeons and at least one of the radiologists who performed the sonographic examination together compared the excised nodes with the nodes studied sonographically. Final decisions were reached by consensus. The excised nodes that matched those on sonograms were then examined histopathologically. These data were compared with a map illustrating the metastatic or nonmetastatic nodes depicted sonographically, thus enabling the surgeon to correlate the dissected nodes with the nodes depicted on the sonograms.
Classification of Lymph Nodes in Relation to Anatomic Location in the Neck
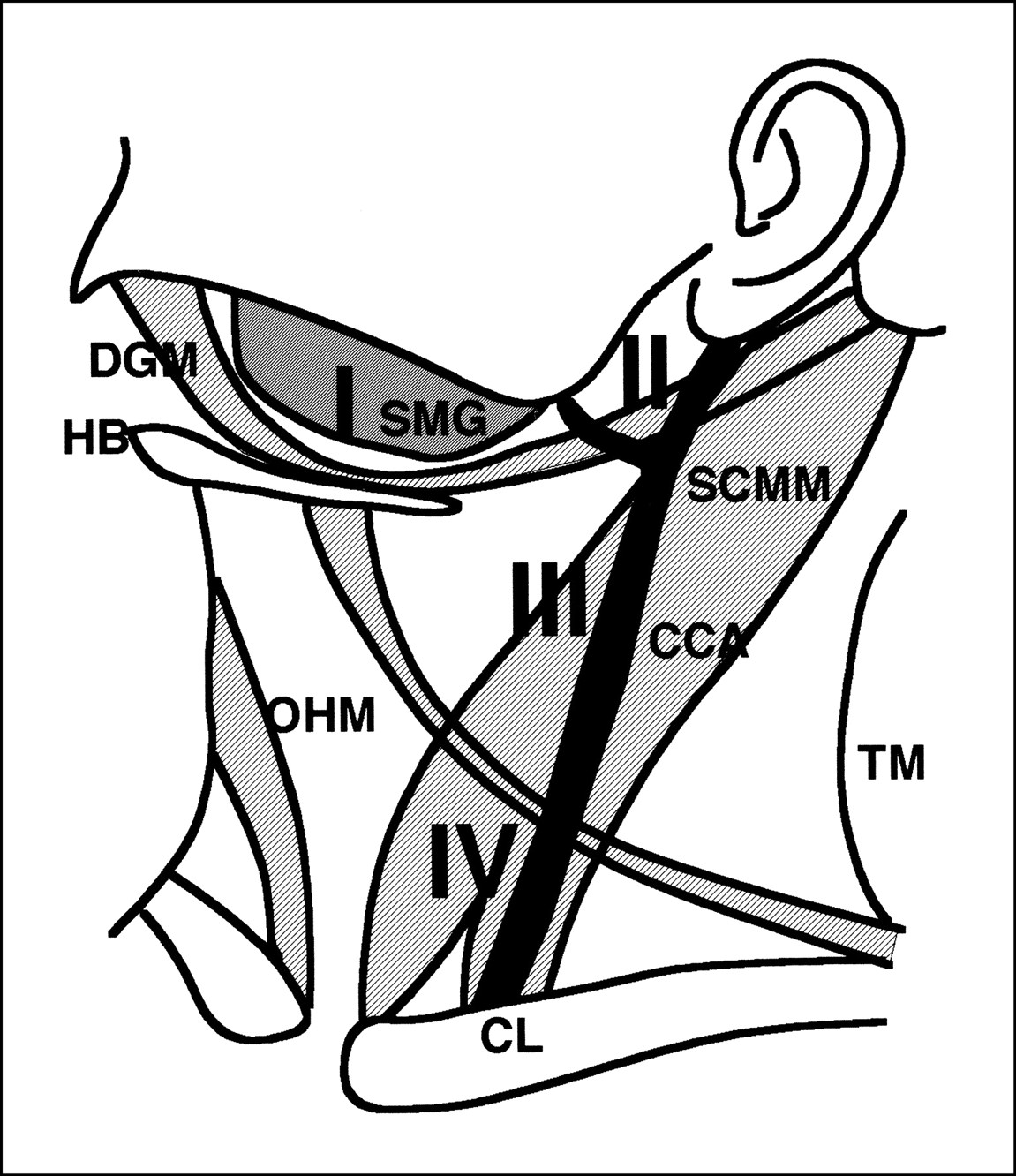
The nodes were grouped into three levels, as described in a previous report (8). Briefly, nodes assigned to level I were those in the submental and submandibular regions (Fig 1). This segment was bordered posteriorly by the posterior margin of the submandibular gland. Level II was bordered anteriorly by the posterior border of level I and inferiorly by the axial line through the carotid bifurcation. Curtin et al (8) used the inferior border of the hyoid bone instead of the carotid bifurcation; however, the carotid artery was useful as a reference for sonography. Level III was bordered superiorly by the inferior border of level II, posteriorly by the anterior margin of the trapezius muscle, and inferiorly by the inferior border of the cricoid cartilage. Level IV was also bordered posteriorly by the trapezius muscle, and represented the entire area of the neck inferior to the cricoid cartilage. Because of the paucity of nodes in level IV, we categorized the nodes at levels III and IV collectively as level III+IV.

Schematic representation of neck levels I through IV for the classification of cervical lymph nodes. SMG, submandibular gland; DGM, digastric muscle; HB, hyoid bone; OHM, omohyoid muscle; SCMM, sternocleidomastoid muscle; TM, trapezius muscle; CCA, common carotid artery; CL, clavicle
Interpretation of Sonograms and Assessment of Predictive Ability of Sonographic Features
All sonograms were interpreted by a single radiologist who had over 10 years' experience performing sonography and who had no knowledge of any clinical information about the patients. To assess nodal size, short-axis diameters were measured on hard copies of sonograms using calipers and a length standard and then expressed in millimeters. The short-axis diameter was defined as the greatest diameter on the maximum axial cross-sectional area of a node (Fig 2). Doppler blood flow features of the node were categorized into two types: 1) normal hilar blood flow, which was depicted as club- or Y-shaped flow present in the hilar echoes (Fig 3A–C); and 2) abnormal hilar blood flow, which was considered to be a parenchymal or avascular pattern (Fig 3D–F). The combined-criteria diagnosis of metastatic nodes relied both on short-axis diameter cut-off values (which varied from 5 to 10 mm) and presence or absence of normal hilar blood flow at Doppler sonography; the single-criterion diagnosis relied just on measurements of short-axis nodal diameters.

Sonogram shows definition of the short-axis diameter (arrow) of a node

Doppler sonographic features of reactive (A–C) and metastatic (D–F) nodes located at level I (A, D), level II (B, E), and level III+IV (C, F). Arrows indicate normal hilar blood flow.
A, Reactive node (7 mm in short-axis diameter) in 55-year-old man with squamous cell carcinoma of lower gingiva shows normal hilar blood flow.
B, Reactive node (8 mm in short-axis diameter) in 66-year-old man with squamous cell carcinoma of soft palate shows normal hilar blood flow.
C, Reactive node (6 mm in short-axis diameter) in 64-year-old man with squamous cell carcinoma of lower gingiva shows normal hilar blood flow.
D, Absence of normal hilar blood flow and presence of parenchymal flow in a metastatic node (7 mm in short-axis diameter) in a 48-year-old man with squamous cell carcinoma of the tongue.
E, Absence of normal hilar blood flow and presence of parenchymal flow in a metastatic node (8 mm in short-axis diameter) in a 53-year-old man with squamous cell carcinoma of the hypopharynx.
F, Absence of normal hilar blood flow in a metastatic node (5 mm in short-axis diameter) in a 49-year-old man with squamous cell carcinoma of the upper gingiva.
Negative and positive predictive values were used to assess the performance of sonographic examinations in the detection of metastatic nodes. The negative predictive value is the percentage of nodes interpreted on sonograms as negative for metastasis that were histopathologically proved not to be metastases. The positive predictive value is the percentage of nodes interpreted at sonography as positive for metastasis that were histopathologically proved to be metastases. We also calculated the sensitivity (true-positive results/[true-positive results + false-negative results]) and specificity (true-negative results/[true-negative results + false-positive results]). The accuracy was calculated by the following formula: (true-positive results + true-negative results)/total number of nodes.
Although the increase in positive predictive value would decrease the number of patients who undergo unnecessary treatment, the decrease in negative predictive value would increase the number of patients in whom metastatic tumor would be left untreated. If these patients were untreated, the residual metastatic tumor would continue to grow and lower the patients' rate of survival. Undertreatment is not as acceptable as overtreatment. From this point of view, the relatively high negative predictive value (>90%) and high positive predictive value (>80%) should be considered promising criteria for the diagnosis of metastatic nodes (8). We selected 90% negative predictive value and 80% positive predictive value as the minimum cut-offs for acceptable sonographic criteria.
Histopathologic Procedures
Histologic examinations on the excised nodes were first performed by bivalving the large nodes. The specimens were then fixed and embedded in paraffin. Sections with a thickness of 6 μm were obtained at intervals of 20- to 30-μm from either half of each of these nodes. The small nodes were fixed without bivalving, embedded in paraffin, and sections were obtained at intervals of 20 to 30 μm from each half. Although most of the histopathologic sections were reevaluated by one of the investigators, we could not rule out the possibility that there was micrometastasis in the nodes that were considered not to be metastases. This should be considered a possible potential flaw in the technique.
Statistical Analysis
The Mann-Whitney U test was used to evaluate the differences in overall accuracy between the single criterion (short-axis diameter) and the combined criteria (short-axis diameter plus absence of hilar flow on Doppler sonograms) for metastatic nodes. The differences in performance of sonographic criteria (accuracy, sensitivity, and specificity) for the best cut-off value at each neck level between the single and combined criteria were assessed by the McNemar test or the exact form of the McNemar test (13).
Results
Predictive Ability for Metastasis by Short-Axis Diameter Criteria
Table 1 shows positive and negative predictive values and sensitivity and specificity yielded by varying cut-off values for short-axis nodal diameters. At level I, combinations of high positive (>80%) and negative (>90%) predictive values were obtained at cut-off values of 8, 9 and 10 mm. Of these, the best compromise of sensitivity and specificity was obtained at the short-axis diameter of 8 mm. Combinations of high positive and negative predictive values were associated with good compromises of sensitivity and specificity at cut-off values of 9 mm at level II and at 7 mm at level III+IV. These diameters also provided the highest accuracy at each level.
Performance of the single criterion of short-axis length in predicting metastatic cervical nodes*
Effects of Combined Use of Size and Doppler Criteria on Predictive Ability of Sonography for Metastatic Nodes
The presence of normal hilar flow, which appeared as a club- or Y-shaped blood flow signal in the hilum, significantly contributed to the correct diagnosis of reactive (nonmetastatic) nodes, even if the reactive nodes had short-axis diameters equivalent to those of the metastatic nodes (11), which did not exhibit normal hilar blood flow patterns (Fig 3).
The combined use of short-axis diameter and Doppler criteria (absence of normal hilar flow) increased the positive predictive values at the minimal expense of negative predictive values at each of the corresponding cut-off values at all levels in the neck (Table 2). Consequently, the combined criteria significantly increased the overall accuracy at all levels in the neck: Mann-Whitney U test, P < .0000001, z(0.975) = 1.96 for level I; P < .0000001, z(0.975) = 1.96 for level II; and P = .000121, z(0.975) = 1.96 for level III+IV. Thus, a combination of high positive (>80%) and negative (>90%) predictive values was obtained even at cut-off values of 6, 7, and 5 mm for nodes at levels I, II, and III+IV, respectively. Furthermore, these cut-off values yielded high sensitivities (≥89%) and specificities (≥94%), resulting in the highest accuracy at each level of the neck. Therefore, the combined criteria decreased the best cut-off values at all levels in the neck (Table 2). When overall accuracy was compared for the 338 nodes between the single and combined criteria, Doppler flow information significantly increased the accuracy (McNemar test, P = .01963).
Performance of the combined criteria of short-axis length and Doppler blood flow in predicting metastatic cervical nodes
Discussion
We assessed whether the Doppler sonographic evaluation of intranodal blood flow patterns could improve the predictive ability of size as the single criterion for metastatic cervical nodes in patients with head and neck cancer. To this end, we compared negative and positive predictive values along with sensitivity and specificity between the single criterion of size (short-axis diameter) and the combined criteria of size plus Doppler sonographic characteristics (absence of hilar flow). The sonographic topography of the nodes was compared with dissected specimens to assess the performance of the sonographic criteria by node. We found that the addition of Doppler information improved sonographic evaluation by decreasing the cut-off values of the short-axis diameters of metastatic nodes at all levels of the neck.
Performance of the Short-axis Diameter Criterion
Investigators have proposed a variety of cut-off values (ranging from 8 to 30 mm) as sonographic size criteria for establishing metastatic cervical nodes (14–18). More recently, van den Brekel et al (6) showed that a minimal axial diameter of 7 mm for nodes at level II and 6 mm for nodes elsewhere in the neck offered the best compromise between sensitivity and specificity. However, the accuracy obtained by these authors was moderate. Our findings using a single criterion were somewhat different, indicating that higher cut-off values were required for obtaining high predictive ability. Since we and van den Brekel et al (6) measured nodal size in a similar fashion, the discrepancies between our studies may be due to differences in the methods used to assess concordance between sonographic and histopathologic evaluations; they did not compare sonograms and dissected specimens by node but rather by levels in the neck.
Our study indicated that the best cut-off value for the short-axis diameter of nodes at level II was higher than that for nodes at the other two levels of the neck when size criterion was used alone, which is consistent with the findings of van den Brekel et al (6). The best cut-off value at level I was higher than that at level III+IV. This may be due in part to the fact that nodes at these levels are subject to inflammatory extension from the oral cavity, since they are located on the main routes of lymphatic drainage from the teeth and periodontal tissues. Therefore, the size criterion for these nodes may be affected by oral infection (12).
Combined Criteria of Short-axis Diameter and Doppler Sonographic Findings
Several lines of evidence suggest that blood flow information is useful in predicting metastatic nodes in patients with head and neck cancer (4, 9, 10, 19). Multivariate analysis has shown that Doppler flow information (the presence of hilar flow) significantly contributes to the prediction of reactive (nonmetastatic) nodes in patients with head and neck cancer (11). In one study in which the population consisted predominantly of patients with malignant lymphomas, the combined criteria of long-to-short axis ratios and vascular sonographic features were found to improve the diagnostic performance of sonography in establishing nodal malignancies (20).
We have extended these previous findings to show that the combined criteria of short-axis diameter and Doppler sonographic evidence of an absence of normal hilar flow significantly increase the predictive ability of sonography in diagnosing metastatic nodes in patients with head and neck cancer. The combination of Doppler characteristics and short-axis diameter allowed the use of smaller size criteria (for measurements of the short-axis diameter of cervical nodes) for establishing metastatic nodes at all levels in the neck. The best cut-off values for the short-axis diameter decreased to 6 mm for nodes at level I, 7 mm for nodes at level II, and 5 mm for nodes at level III+IV. These cut-off values were equivalent to or lower than those reported by van den Brekel et al (6) and others. Importantly, our study yielded higher sensitivity (89%) together with higher specificity (94%) than reported previously. Therefore, the present findings indicate that use of the combined criteria of Doppler sonography (blood flow information) and nodal size (short-axis diameter) may facilitate earlier detection of metastatic nodes than does use of the single criterion of size.
Our results may be somewhat biased toward a higher rate of accuracy, because the techniques we used to correlate nodes on sonograms with those at histopathologic examination may have been subject to selection bias. A similar study on metastatic nodes from head and neck squamous cell carcinoma that used sonography with sonographically guided fine-needle aspiration biopsy yielded a lower rate of accuracy than ours (21).
Conclusion
Taken together with previous findings, our results indicate that Doppler sonographic evaluation improves the performance of sonographic diagnosis of metastatic nodes in patients with head and neck cancer (Table 3). Although the sonographic evaluation of metastatic nodes has several disadvantages (9), it predicts the presence of metastatic nodes with accuracy equivalent or superior to that obtained with CT and MR imaging (8). Furthermore, for the detection of nodes in the submental and submandibular regions, where CT and MR studies have occasionally been impaired by artifacts from bones and dental amalgam, the addition of Doppler techniques to the sonographic evaluation facilitated the early detection of metastatic nodes. Therefore, sonography may be an adjunct, if not the main, tool in diagnosing metastatic nodes in patients with cancer. In particular, the proposed criteria may be helpful for detecting metastatic nodes with high rates of sensitivity and specificity, thus precluding unnecessary treatment of patients with no neck disease (22).
Summary of proposed sonographic criteria for establishing metastatic cervical nodes
Footnotes
↵1 Address reprint requests to Dr. Takashi Nakamura, Department of Radiology and Cancer Biology, Nagasaki University School of Dentistry, 1-7-1 Sakamoto, Nagasaki 852-8588, Japan.
References
- Received January 7, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sonography for Diagnosis of Benign and Malignant Tumors of the Nose and Paranasal Sinuses
- Quantitative evaluation of vascularity within cervical lymph nodes using Doppler ultrasound in patients with oral cancer: relation to lymph node size
- Sonographic Examination of the Neck after Definitive Radiotherapy for Node-Positive Oropharyngeal Cancer
- Small Atypical Cervical Nodes Detected on Sonography in Patients With Squamous Cell Carcinoma of the Head and Neck: Probability of Metastasis