
Abstract
Summary: Pigmented villonodular synovitis (PVNS) is a benign proliferative disorder primarily occurring in the large joints of the appendicular skeleton such as the knee and hip joints. We present an unusual case of PVNS involving the cervical spine in an adult. MR imaging showed an enhancing mass lesion arising from the posterior elements of the cervical spine and hyperintensity on the T2-weighted images, without evidence of T2 susceptibility effects. Gross total excision of the tumor was performed, and the diagnosis was established by histopathology.
Pigmented villonodular synovitis (PVNS) is a slow-growing lesion of uncertain etiology arising from the synovial membrane. It is characterized by villous and nodular overgrowths of the synovial membrane of the bursa or the tendon sheath. The appendicular skeleton, especially large joints such as the knee and hip joints are frequently involved. Smaller joints of the hand and feet may occasionally be involved (1), although PVNS involving the spine is rare. The first case of spinal PVNS was reported in 1980 by Kleinman (2). Since then, about 29 cases have been reported to date, with Giannini et al presenting a study of 12 cases of spinal PVNS (2–10). We highlight the imaging features of PVNS of the spine in this report, in particular the varied signal intensity characteristics of PVNS at MR imaging, which depend on its pathologic composition. PVNS lesions typically contain areas of intermediate and/or low signal intensity on T1- and T2-weighted images (11). The decreased signal intensity becomes more pronounced on the long TR/TE images, because of the preferential shortening of T2 relaxation times of hemosiderin pigment (12). In the absence of such susceptibility changes, however, the radiologic diagnosis of PVNS can be difficult preoperatively. We present such a case of PVNS of the posterior spinal elements.
Case Report
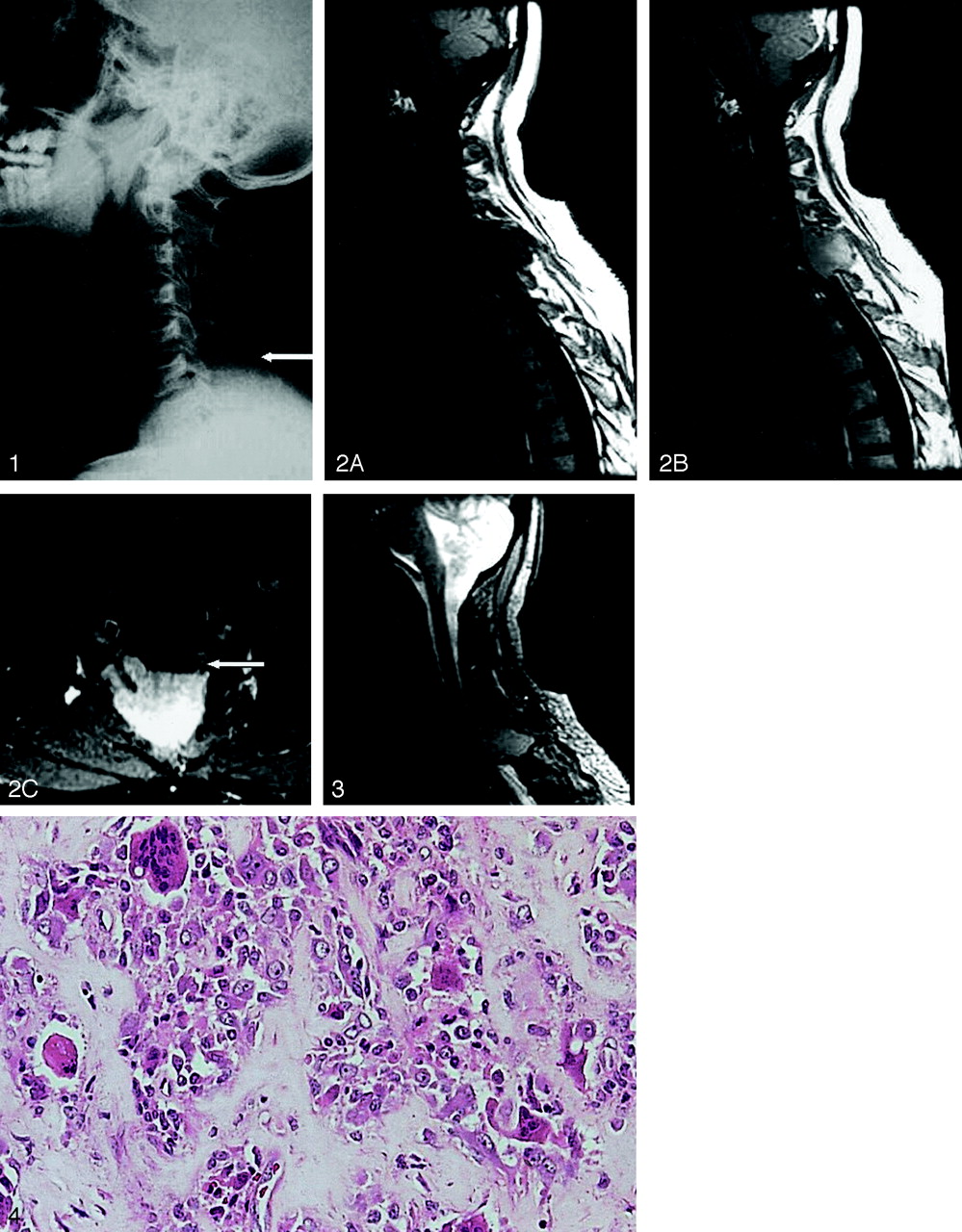
A 43-year-old man presented with pain in the back of the neck radiating to the right upper limb. The pain had progressed over a period of 3 months. There was no weakness of the lower limbs or incontinence of bladder or bowel. His cervical spine radiograph revealed a large, ill-defined soft tissue mass posteriorly at C5–C6 level, with osteolysis of the posterior elements of C5 and C6 vertebra (Fig 1). Minimal scalloping of C6 vertebral body was also seen. There were no calcific foci seen within this mass. On MR images (Fig 2), there was a large extradural mass involving the posterior elements of C5 vertebra, destroying both the lamina and the spinous process. The posterior elements of C6 were also involved. The lesion was predominantly isointense on T1-weighted image and was hyperintense on T2-weighted images. There were no areas of T2 shortening on T2 gradient echo images (Fig 3). After contrast medium administration, it showed slightly inhomogeneous but marked enhancement. It was displacing the thecal sac anteriorly without causing significant cord compression. On the basis of the imaging findings, a diagnosis of giant cell tumor of bone or an osteoblastoma was considered. Aneurysmal bone cyst was another consideration although there were no typical fluid-fluid levels. A preoperative angiogram showed a moderately hypervascular tumor, which was mainly supplied by the right costocervical artery via its deep cervical branch with lesser supply via the left costocervical artery. Preoperative embolization of the feeder vessels was performed with polyvinyl alcohol (PVA) particles (150–250 μ).

Lateral radiograph of the cervical spine shows a soft tissue mass destroying the posterior elements of the lower cervical spine (arrow). There are no foci of calcifications seen within this mass.
Fig 2. Sagittal T1-weighted images before (A) and after (B) contrast administration show an expansile mass lesion involving the posterior elements of C5 and C6 vertebra. This mass shows homogeneous enhancement after contrast material administration. It is seen to displace the thecal sac anteriorly. C, Axial T1-weighted postcontrast image with fat suppression shows the exact delineation of the mass with an anteriorly displaced thecal sac (arrow).
Fig 3. Sagittal gradient-echo T2-weighted image shows the mass to be hyperintense with no evidence of T2 shortening within it to suggest areas of hemosiderin deposition.
Fig 4. Histopathologic section of pigmented villonodular synovitis depicting sheetlike growth within the main tumor mass, which is comprised of mononuclear cells and multinucleated giant cells within the collagenized stroma. Hematoxylin and eosin (×100).
Subsequently, the patient underwent surgery via a posterior approach. A gross total resection of the tumor was performed with C4–C6 laminectomy. The resected specimen was approximately 7 × 6 × 1.5 cm in size and was predominantly solid, multinodular, and yellowish in hue. Microscopic examination showed a moderately cellular lesion comprising sheets of polygonal mononuclear cells with bland nuclei and eosinophilic cytoplasm. Mitoses were infrequent. Scattered multinucleated giant cells were also seen along with collagenized stroma (Fig 4). There were areas of coagulative necrosis (presumably because of the preoperative embolization) seen within the tumor. There was minimal peritumoral reactive bone and cartilage formation. There was no evidence of malignancy. A diagnosis of pigmented villonodular synovitis was made based on the histopathologic findings. This lesion located in posterior cervical spine location with collagenized stroma is not seen in giant cell tumor of bone and the absence of malignant cells ruled out malignant fibrous histiocytoma as a histopathologic differential consideration. At 6-month follow-up, the patient was clinically asymptomatic and his follow-up MR study showed no evidence of tumor recurrence. There was no postoperative radiation therapy.
Discussion
PVNS is a locally aggressive proliferative disorder most commonly affecting large synovium-lined joints. In some instances, the disease may show extraarticular soft tissue involvement, representing extraarticular extension of a primary intraarticular process. Rarely, the disease may reside completely outside the joint, in which case the origin maybe from the synovium of the bursa or the tendon sheath (9, 12).
Many other terms have been applied to it, including nodular tenosynovitis, fibrous histiocytoma of synovium, giant cell synovioma, and fibrous xanthoma of synovium (1). The term “pigmented villonodular synovitis” was first proposed by Jaffe in 1941 (1). PVNS results in various degrees of villous and/or nodular changes in these affected structures. Two primary forms are described, including a diffuse form that affects the entire synovial lining of the joint, bursa, or tendon and a smaller localized form. The diffuse form typically involves the large joints such as the knee and hip joints. The localized (focal) form affects the small joints of the hand/feet. The focal form is sometimes seen around the tendon sheaths and is then called giant cell tumor of tendon sheath (13). In practice, the term “PVNS” is generally used when the condition affects the joints, regardless of whether it is diffuse on localized. Our case was of the diffuse type, because it was seen to be involving the adjacent vertebra and had also invaded the paraspinal muscles. The spinal form of PVNS is thought to arise from the synovial membrane of the facet joints; however, considering the number of synovium lined joints in the spine, it is surprising to find that the spinal form of PVNS is relatively rare (14).
The exact etiology of PVNS is ill understood. Inflammatory reaction, neoplasia, hyperplasia, metabolic derangement, and recurrent hemorrhages due to trauma have all been considered possible etiologies (1, 10, 15). Trisomy 7 was documented in one case, suggesting that at least some cases represent clonal neoplastic proliferations (16). Furthermore, PVNS spares joints with hemophilic arthritis and Charcot arthritis (3). It also has a significant tendency for local recurrence and this has been related to the degree of resection, lesion cellularity, and mitotic activity (1, 10).
PVNS is seen to affect a wide age range of patients, with no definite sex predilection (3). In the spine, the lumbar vertebrae have a higher incidence of involvement than the cervical or thoracic vertebrae. Almost all the cases of PVNS of the spine present with radicular symptoms due to the compression of nerves by the extradural soft tissue masses. Our patient similarly presented with pain radiating to the right upper limb.
The pathologic findings of spinal PVNS are similar to those seen in the appendicular skeleton (17). Synovial cells lined villous fronds containing polygonal mononuclear cells, multinucleated giant cells, fibroblasts, and foamy macrophages containing lipid and hemosiderin may be noted. Expansive sheets of mononuclear cells interrupted by cleftlike spaces are also seen; however, extraarticular lesions usually do not have grossly discernible villous patterns, and hemosiderin staining is less evident than in their intraarticular counterparts. The presence and amount of hemosiderin is related to the extent of mechanical trauma that the lesion undergoes. Hence, PVNS lesions in the spine are often less pigmented. We believe that this variable amount of lipid and hemosiderin probably accounts for the variable MR imaging appearance of PVNS and may explain the absence of T2 susceptibility in our case, where the tumor was in a non-weight-bearing joint and bulk of the tumor was extraarticular.
Routine radiographs and CT scan of spinal PVNS often demonstrate pressure erosion with sclerotic margins of the bone associated with nodular soft tissue masses. The matrix of the tumor is rarely calcified. Reactive bone formation is also typically absent. On CT scans, the lesion may appear hyperattenuated secondary to the presence of intracellular and extracellular hemosiderin (13). At MR imaging, PVNS show areas of intermediate to low signal intensity abnormality due to the presence of hemosiderin, which is accentuated on the T2 gradient echo sequences (11, 12), but it may show variable appearance, depending on the composition of the lesion and relative proportion of hemosiderin, lipid, fibrous tissue, cyst formation and cellular elements. PVNS often shows marked enhancement after contrast material administration. MR imaging is also helpful for exact delineation of the intraspinal, as well as paraspinal, extent of the lesion. As seen in our case, where there were no areas suggestive of T2 hypointensity, however, MR imaging findings are not always characteristic of PVNS. The limited number of cases reported in the literature with limited data on PVNS of the spine often makes the differential diagnosis difficult.
Different pathologic conditions such as osteoblastoma, aneurysmal bone cyst, giant cell tumor of bone, and hypertrophic synovitis (with synovial cyst formation) should be considered (3). Both osteoblastoma and aneurysmal bone cyst show a predilection for the posterior elements. Osteoblastomas typically occur in younger male patients and cause expansile lesion of the posterior elements and/or the vertebral body (18). They are usually hyperintense on T2-weighted images and show variable contrast enhancement due to vascularized stroma. Aneurysmal bone cyst (ABC) is composed of large anastomosing cavernous spaces filled with blood products (19). At MR imaging it shows multiple expansile cystic lesions with variable signal intensity on T1- and T2-weighted images because of the presence of blood products. The presence of multiple fluid-fluid levels and T1 hyperintensity, if present, is considered more likely for an ABC (20). Giant cell tumors of bone are not uncommon in the spine with the sacrum being the preferred site in the spine (21). They show involvement of the vertebral body more than the posterior element (22), with variable appearance on the T2-weighted images, and most of the tumors show contrast enhancement. Synovial cysts are often seen associated with facet joint abnormalities and are typically rounded, well defined, and cystic in nature. Increased density is sometimes seen at the margins, presumably because of calcification or hemorrhage (13). Rarely, they can grow large or cause bone erosions (23). At MR imaging, synovial cysts are hypointense on T1-weighted images and turn hyperintense on T2-weighted images following the signal intensity characteristics of a fluid-filled structure. Uncommonly, they may have fibrous tissue or gas in the center and may exhibit variable signal intensity at MR imaging. In the absence of typical imaging findings of PVNS, image-guided biopsy or excision of the lesion may be considered. The presence of mononuclear cells, multinucleated giant cells, and hemosiderin deposition, if present, are typical histologic features, which indicate the diagnosis of PVNS (3).
Conclusion
Although PVNS of the spine may be expected to have typical MR imaging features because of the presence of hemosiderin, not all cases of PVNS will show the characteristic signal intensity patterns, as was seen in our case. PVNS, therefore, should be considered in the differential diagnosis of expansile osteolytic lesions involving the posterior vertebral elements.
References
- Received March 20, 2003.
- Accepted after revision April 28, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}