
Abstract
BACKGROUND AND PURPOSE: The T2-weighted gradient-echo (GRE) imaging is currently the gold standard MR imaging sequence for the evaluation of patients with cerebral cavernous malformation (CCM) lesions. We aimed to compare the sensitivity of susceptibility-weighted imaging (SWI) with T2-weighted fast spin-echo (FSE) and GRE imaging in assigning the number of CCM lesions in patients with the familial form of the disease.
Materials and METHODS: We studied 15 patients (8 men, 7 women; mean age, 34 years) with familial CCM. All patients underwent MR imaging with the following sequences: T1-weighted spin echo, T2-weighted FSE, T2-weighted GRE, and SWI. Two neuroradiologists read the images regarding the number of lesions seen on each sequence. The final decisions were reached by consensus. The number of lesions on the different sequences was compared with analysis of variance, followed by a nonparametric Wilcoxon matched-pairs signed rank test.
RESULTS: The number of lesions was higher on T2-weighted GRE than on T2-weighted FSE (P = .001). In addition, more lesions were seen on SWI than on T2-weighted GRE (P = .001) and FSE (P = .001) sequences.
CONCLUSION: The sensitivity of SWI in assigning the number of CCM lesions in patients with the familial form of the disease is significantly higher than that of T2-weighted FSE and GRE sequences.
Cerebral cavernous malformation (CCM) comprise 5%–13% of all the central nervous system vascular malformations, with an estimated prevalence of 0.5% in the general population. Histologically, the lesion is defined as blood cavities surrounded by a single layer of endothelium, without muscular tissue or intervening brain parenchyma.1,2 CCM may occur as a sporadic form, in which patients usually have a single lesion, and a familial form, characterized by multiple lesions and autosomal dominant transmission.3,4
The finding of multiple CCM lesions calls for a family screening that may confirm the diagnosis of unrecognized affected patients and establish the baseline imaging for the appropriate follow-up of the kindred. The likelihood of a de novo lesion in the future and counseling of female kindred in childbearing age make necessary an imaging surveillance of the family members with the best imaging technique available.5,6
MR imaging is currently the best imaging method to evaluate CCM.6 On T2-weighted sequences, the lesions usually appear as areas of mixed signal intensity, with a central reticulated core and a peripheral rim of decreased signal intensity.6,7 T2-weighted gradient-echo (GRE) imaging has been advocated as the gold standard MR imaging sequence for both sporadic and familial CCM evaluation.7,8
Susceptibility-weighted imaging (SWI) is a technique that exploits the magnetic properties of tissues, such as blood or iron content. Recently, a new SWI was described, which is a technique that maximizes the sensitivity to susceptibility effects by combining a long-TE high-resolution fully flow-compensated 3D GRE sequence with filtered phase information in each voxel.9,10 As a result, SWI has an exquisite sensitivity to the venous vasculature, blood products, and vascular malformations. Preliminary studies have suggested that SWI is more sensitive than T2*-weighted imaging for evaluating CCM.11,12
The goal of this study was to evaluate the sensitivity of SWI compared with T2-weighted fast spin-echo (FSE) and GRE sequences in assigning the number of CCM lesions in patients with the familial form of the disease. We hypothesized that the number of CCM lesions is better evaluated with the SWI sequence.
Materials and Methods
This prospective study included 8 male and 7 female subjects (ages ranging from 18 to 74 years of age; mean age, 34 years of age) from 6 families with CCM. All patients signed informed consent forms, and the institutional review board of our hospital approved the study.
All patients underwent MR imaging in a 1.5T scanner (Magnetom Avanto; Siemens, Erlangen, Germany) with a 12-channel head coil. The standard protocol included T1-weighted spin-echo imaging (SE) (TR/TE, 375/11 ms; flip angle, 90°; FOV, 230 mm; matrix, 512 × 256; section thickness, 3 mm; intersection gap, 0.9 mm), T2-weighted FSE imaging (TR/TE, 4,880/116 ms; flip angle, 30°; echo-train length, 11; FOV, 230 mm; matrix, 512 × 256; section thickness, 3 mm; intersection gap, 0.9 mm), and T2-weighted GRE imaging (TR/TE, 829/26 ms; flip angle, 20°; FOV, 230 mm; matrix, 512 × 256; section thickness, 3 mm; intersection gap, 0.9 mm).
The SWI technique used in this study is a novel imaging method that maximizes the sensitivity to susceptibility by combining a long-TE high-resolution fully flow-compensated 3D GRE sequence with filtered phase information in each voxel to both enhance the contrast in magnitude images and add the susceptibility differences between tissues as a new source of information.9–12 The SWI was acquired with the following parameters: TR/TE, 57/40 ms; flip angle, 20°; rectangular FOV, 5/8; matrix, 512 × 256; section thickness, 2 mm). All images were acquired in the same axial plane. Subsequently, the SWI sequences were reconstructed with minimum intensity projection (MinMIP) technique to obtain images with section number, thickness, and position similar to those of T2-weighted FSE and GRE sequences.
Two neuroradiologists were blindly and independently assigned to read the images on the PACS system (Carestream Health, Rochester, NY). The equivalent sections of SWI, T2 FSE, and T2 GRE were compared simultaneously in 2 conjugated 19-inch monitors divided into 4 windows. The neuroradiologists counted the number of lesions in each sequence and compared all of them, confirming that all the lesions seen on T2-weighted FSE were observed on both T2-weighted GRE and SWI and that all lesions demonstrated on T2-weighted GRE were seen on SWI.
In addition, all the CCM lesions were classified according to Zabramski et al7 into types I-IV, based on conventional T1 and T2 FSE and GRE MR imaging sequences. The type I lesions are defined as having a hyperintense core on T1-weighted images and hyper- or hypointense on T2-weighted FSE sequences. The type II are seen as reticulated mixed–signal intensity cores on T1- and T2-weighted FSE sequences, with a hypointense rim on T2-weighted FSE images. The next category, type III, exhibits iso- or hypointense signal intensity on T1-weighted FSE images and hypointense signal intensity with a hypointense ring magnified on T2-weighted FSE sequences. Finally, the type IV CCM lesions present as punctate hypointense lesions on T2-weighted GRE images. The lesions seen only on SWI were considered independently of the classification of Zabramski et al.7 The final decisions regarding the number and classification of the CCM were reached by consensus.
The number of CCM lesions seen on T2*-weighted GRE, T2-weighted FSE, and SWI sequences were compared with analysis of variance (ANOVA), followed by a nonparametric Wilcoxon matched-pairs signed rank test. The statistical analysis was performed with the Statistical Package for Social Sciences software, Version 11.0 (SPSS, Chicago, Ill), and values of P < .01 were considered as statistically significant.
Results
All except 2 patients had lesions on the 3 sequences. These patients showed no lesions on T2-weighted FSE and GRE sequences, and 1 had a lesion on SWI. In the remaining 13 patients, there was a mean of 5.7 lesions on T2-weighted FSE imaging (ranging from 1 to 28 lesions), a mean of 26.3 on GRE imaging (ranging from 2 to 89 lesions), and a mean of 45.6 lesions on SWI sequence (ranging from 4 to 149 lesions) (Figs 1–5).

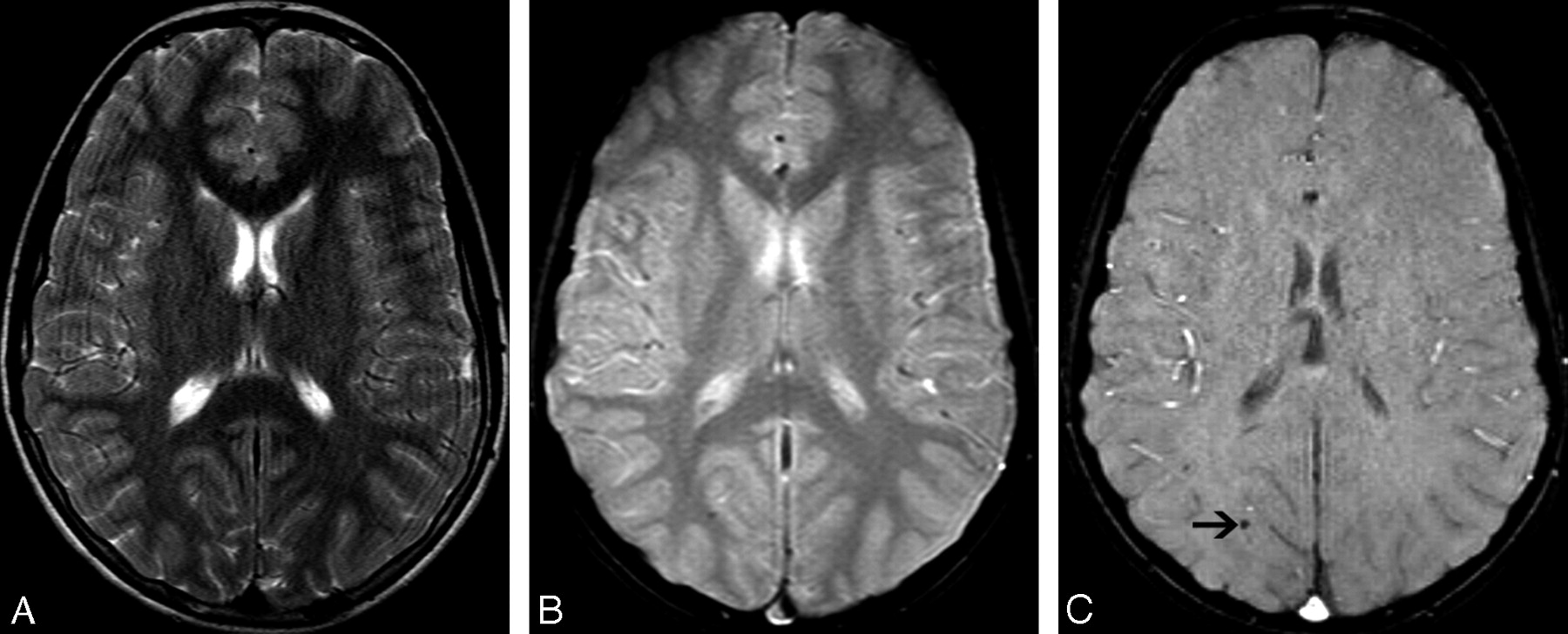
A 46-year-old male patient with familial CCM. A, Axial T2-weighted FSE image shows no significant abnormalities. B, Axial T2-weighted GRE image demonstrates a small extinction on the right parietal region, though it is larger on SWI (type IV lesion) (C, arrow).

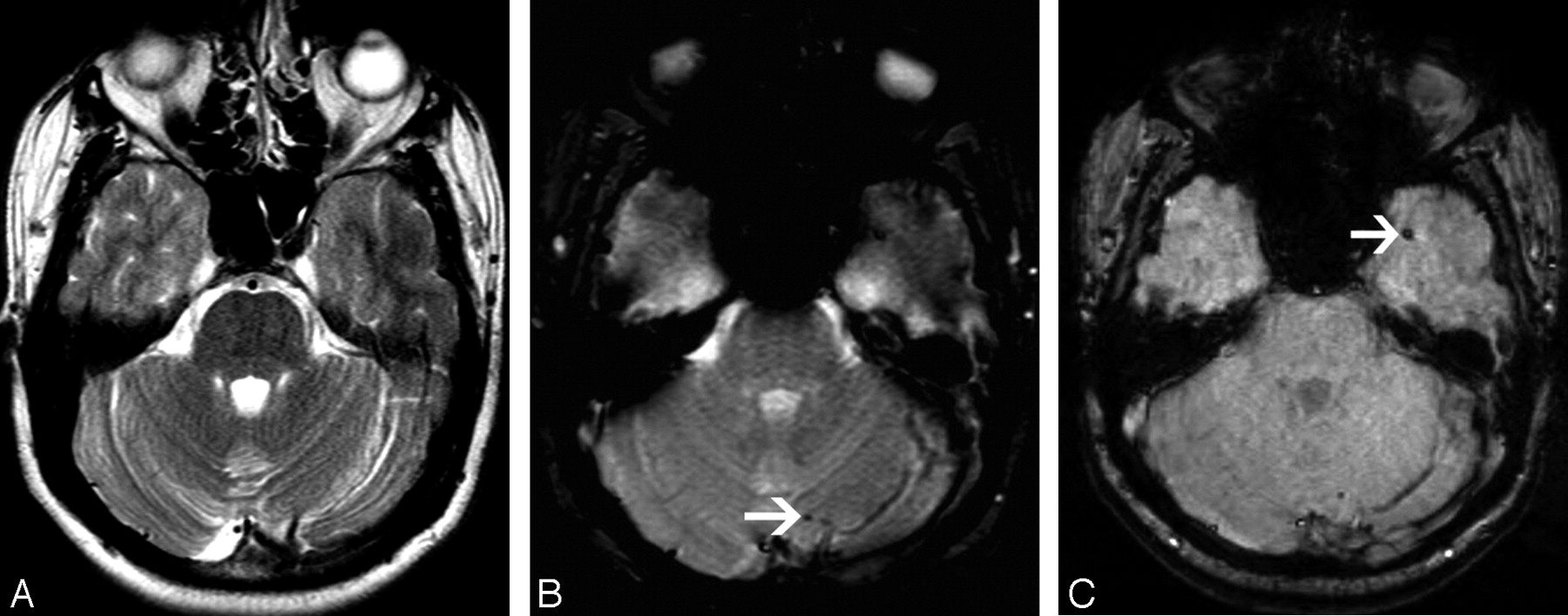
A 53-year-old female patient with familial CCM. A, Axial T2-weighted FSE image shows no significant abnormalities. B, Axial T2-weighted GRE image shows a small focus of low signal intensity (arrow) on the left cerebellar hemisphere (type IV lesion). C, SWI demonstrates the cerebellar lesion but, in addition, shows a left temporal lesion (arrow), which was obscured by the bone artifacts.

A 25-year-old female patient with familial CCM. A, Axial T2-weighted FSE image shows a small area of low signal intensity on the right frontotemporal region (arrow). B, T2-weighted GRE image clearly demonstrates the lesion (type III) (arrow). C, SWI confirms the right frontotemporal lesion. Additionally, SWI demonstrates bilateral frontal lesions (arrows), which were blurred by the bone artifacts.

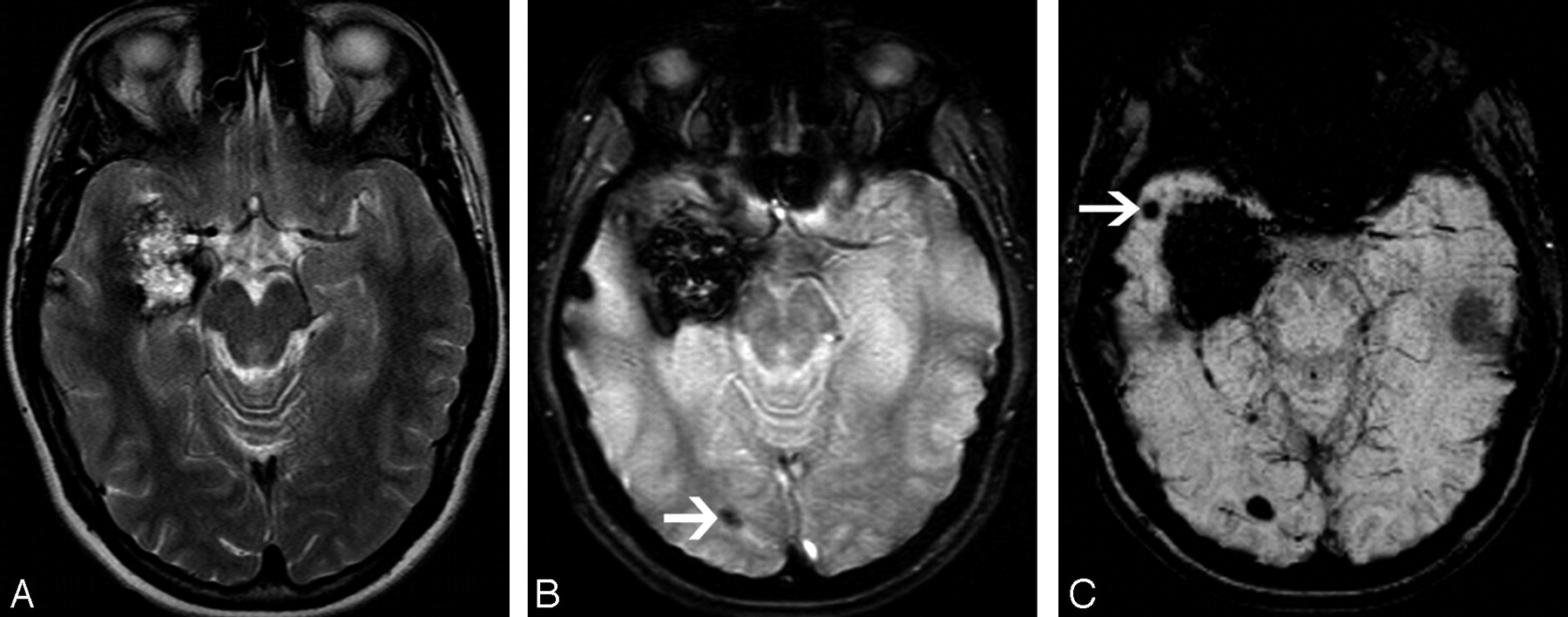
A 22-year-old female patient with familial CCM. A, Axial T2-weighted FSE image shows a large right temporal lesion with mixed signal intensity (type II). B, T2-weighted GRE image demonstrates this lesion and, in addition, a small focus of low signal intensity on the right occipital lobe (arrow). C, SWI shows a small focus of low signal intensity on the right temporal region (arrow), which is dissociated from the large lesion (bloom effect).

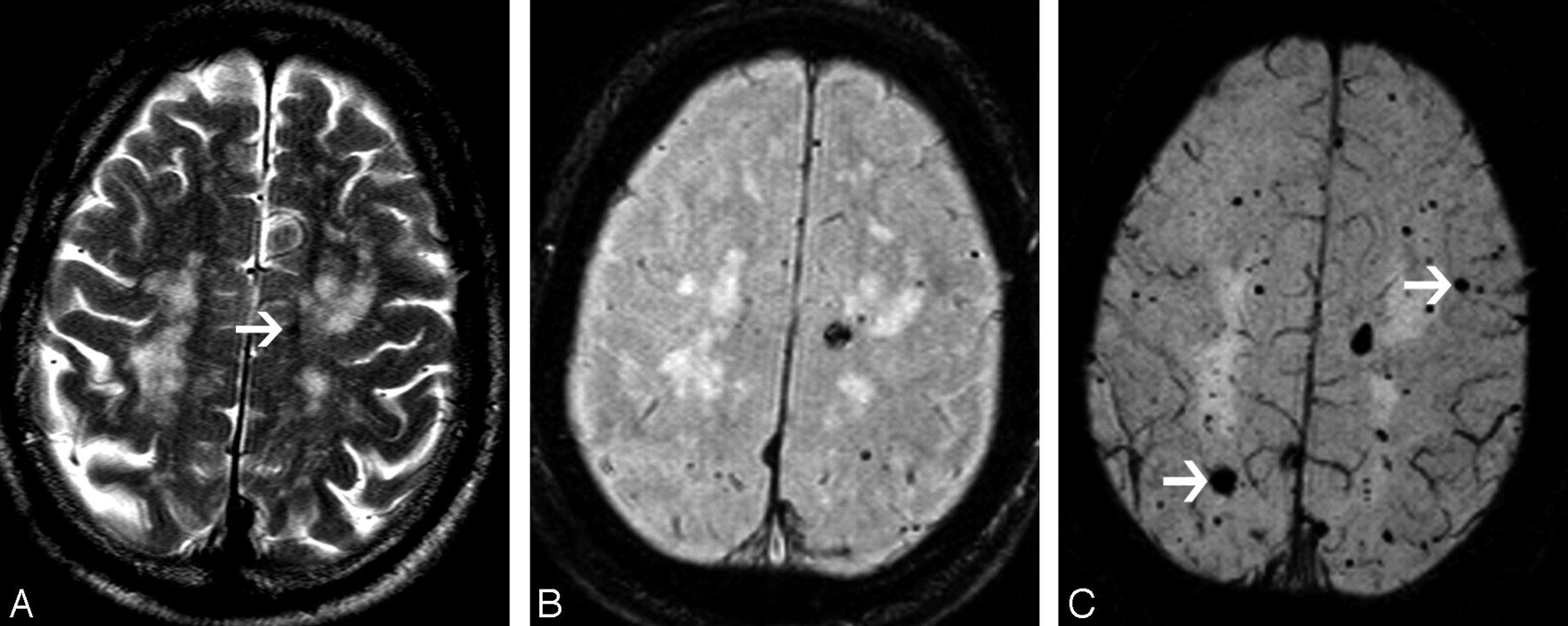
A 74-year-old male patient with familial CCM. A, Axial T2-weighted FSE image shows areas of white matter high signal intensity and a small focus of low signal intensity on the left (arrow). B, T2-weighted GRE image demonstrates multiple foci of low signal intensity on the frontoparietal regions (type IV). C, SWI shows a higher number of lesions and confirms the presence of larger lesions (arrows), which are not seen on the T2-weighted GRE image.
The ANOVA showed that the difference among the number of lesions seen on the 3 sequences was statistically significant (P < .0001). In addition, the number of CCM lesions was higher on T2-weighted GRE than on T2-weighted FSE (P = .001). Finally, more lesions were seen on SWI than on T2-weighted GRE (P = .001) and FSE (P = .001) sequences.
Regarding the classification of CCM based on the MR imaging signal intensity, there were 14 (2.3%) type I lesions, 29 (4.9%) type II, 32 (5.4%) type III, and 267 (44.9%) type IV lesions. However, a substantial number of CCM lesions (n = 253; 42.5%), which were seen only on the SWI sequence, could not be categorized on the basis of the classification of Zabramski et al.7
Discussion
In the present study, we evaluated the sensitivity of SWI in assessing the number of lesions in patients with multiple CCM lesions, compared with that of T2-weighted FSE and GRE sequences. The number of lesions seen in SWI was 1.7 times higher than that seen in T2-weighted GRE and 8 times higher than that in T2-weighted FSE images.
MR imaging is currently the best imaging technique for evaluation of CCM.6–8 In addition, T2-weighted GRE imaging has been advocated as the most sensitive sequence in assessing the number of CCM lesions in both the isolated and familial form of the disease.7,8 Probably related to the blood stagnation phenomenon and chronic microhemorrhages, CCM lesions contain deoxyhemoglobin or hemosiderin, which generates susceptibility effects and causes a decrease in signal intensity.2,8 These signal-intensity abnormalities are better evaluated with GRE images compared with SE and FSE images.
Zabramski et al7 introduced a classification for CCM based on pathologic features and MR imaging characteristics. The type I lesions consist of subacute hemorrhages, type II represents lesions with hemorrhages and thrombosis of varying ages, and type III is chronic hemorrhages with hemosiderin within and around the lesions. The pathology of type IV lesions is still unclear but can represent capillary telangiectasias or a CCM in an early stage. Also, type IV lesions demonstrate a close relationship with the familial form of CCM. In the present series, most of the CCM lesions (44.9%) were type IV. Nevertheless, 42.5% of the lesions were seen only on the SWI sequence and could not be categorized on the basis of the criteria of Zabramski et al.7
In patients with CCM, the presence of multiple lesions is characteristic of the familial form of the disease. Moreover, 50%–84% of the patients with the familial form present with multiple lesions, with a mean of 5.8–6.5 lesions per patient.1,2,5–8 The natural history of the familial CCM was previously investigated by Brunereau et al,6 who studied a group of 40 patients during a mean interval of 3.2 years. They observed bleeding of lesions in 35% of the patients, de novo lesions in 27.5%, signal-intensity changes in 27.5%, and size changes in 22.5% of the patients. Moreover, other studies suggested that the annual bleeding rates and the dynamic course of familial CCM could be related to risk factors such as age, sex, location of the malformation, and previous hemorrhages.8 Because of complications associated with the familial form of CCM, mainly bleeding and de novo lesions, these patients have to be included into protocols of surveillance. In addition, MR imaging screening of family members might make possible earlier diagnosis and better support.5 Finally, new MR imaging sequences more sensitive for detection of hemosiderin deposits, such as SWI, should be included in the protocols, to assess the true prevalence of lesions, as well as to better help investigate the imaging pattern of the CCM lesions.
Our results show the clear superiority of SWI over T2-weighted FSE and GRE sequences in depicting small lesions and also in dissociating CCM from bony interface and hemosiderin artifacts. In fact, the “bloom effect,” which is extremely marked on T2-weighted GRE sequences and may obscure small CCM lesions, is less evident on SWI. In addition, SWI is a 3D sequence, which allows a more complete evaluation of the brain, with the identification of much smaller lesions in different orthogonal planes.
Our study has some weaknesses. Because familial CCM is an uncommon entity, our series included a limited number of patients. In addition, the number of lesions was subjectively assessed. However, the sections of the different sequences were compared in the same planes and independently evaluated by 2 experienced neuroradiologists. In addition, though the section thickness of the 3 sequences was not exactly the same, the SWI sequence was reconstructed with the MinMIP technique to obtain images with section number, thickness, and position similar to those of T2-weighted FSE and GRE sequences. Also, we considered all the foci of marked hypointensity on T2-weighted GRE and SWI as CCM lesions, though we had no histologic evaluation of these lesions and some of them might have been calcification or bleeding from other etiologies. Nevertheless, we carefully investigated the clinical history of all the patients and reviewed previous imaging studies, aiming to exclude additional neurologic abnormalities.
Conclusion
In conclusion, the sensitivity of SWI in assigning the number of CCM lesions in patients with the familial form of the disease is significantly higher than that of the T2-weighted FSE and GRE sequences. In our series, the SWI showed 73% more lesions than T2-weighted GRE images. The fact that the SWI is a volumetric sequence, with much fewer artifacts related to the bone-brain interface, might be responsible for the superiority of this sequence. In addition, the bloom effect, which is frequently seen on T2-weighted FSE and GRE sequences but not on SWI, results in blurring around the larger lesions and could obscure small CCM lesions. Finally, because the number of lesions seen on SWI was higher than that on T2-weighted GRE images, we suggest a modification of type IV lesions in the classification of Zabramski et al.7 Instead of lesions not demonstrated on T1- and T2-weighted SE images but seen on T2-weighted GRE, type IV CCM should be defined as lesions not seen on T1- and T2-weighted SE images but demonstrated on SWI. Further studies with pathologic correlation could clarify if the lesions seen on SWI might represent capillary telangiectasias or a CCM in an early stage.
References
- Received March 6, 2007.
- Accepted after revision May 29, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- High Prevalence of Spinal Cord Cavernous Malformations in the Familial Cerebral Cavernous Malformations Type 1 Cohort
- Prediction of Stroke Subtype and Recanalization Using Susceptibility Vessel Sign on Susceptibility-Weighted Magnetic Resonance Imaging
- Parenchymal Hypointense Foci Associated with Developmental Venous Anomalies: Evaluation by Phase-Sensitive MR Imaging at 3T
- Nonalcoholic Wernicke Encephalopathy with Extensive Cortical Involvement: Cortical Laminar Necrosis and Hemorrhage Demonstrated with Susceptibility-Weighted MR Phase Images
- Familial versus Sporadic Cavernous Malformations: Differences in Developmental Venous Anomaly Association and Lesion Phenotype
- Added Value and Diagnostic Performance of Intratumoral Susceptibility Signals in the Differential Diagnosis of Solitary Enhancing Brain Lesions: Preliminary Study
- Semiquantitative Assessment of Intratumoral Susceptibility Signals Using Non-Contrast-Enhanced High-Field High-Resolution Susceptibility-Weighted Imaging in Patients with Gliomas: Comparison with MR Perfusion Imaging
- Reply:
- Pneumocephalus Mimicking Cerebral Cavernous Malformations in MR Susceptibility-Weighted Imaging
- MR Imaging Detection of Cerebral Microbleeds: Effect of Susceptibility-Weighted Imaging, Section Thickness, and Field Strength
- Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, Part 2
- Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, Part 1
- Hemorrhage From Cavernous Malformations of the Brain: Definition and Reporting Standards