Abstract
SUMMARY: Proliferating trichilemmal cysts, also known as pilar tumors, are slow-growing lobulated masses most commonly found on the scalp of elderly women. We present the case of a 69-year-old woman with a 25-year history of multiple enlarging scalp masses. The patient was evaluated for surgical consultation after the dominant mass presented with malignant degeneration. A CT of the head revealed multiple large, subcutaneous, cystic masses with calcifications.
Trichilemmal cysts are keratin-filled cysts with a wall resembling the external root sheath of a hair follicle. These cysts affect 5% to 10% of the population, with a female predominance, and can be inherited in an autosomal-dominant fashion.1 Trichilemmal cysts can undergo transformation into proliferating trichilemmal cysts when tumorlike proliferation of cells arises from the epithelial-lined wall. Proliferating trichilemmal cysts usually result in large lobulated scalp masses. They are most often benign and can recur after incomplete excision. In some cases, malignant degeneration occurs, resulting in direct invasion of adjacent tissues and distant metastases.1 Other clinical sequelae occurring in patients with proliferating trichilemmal cysts include superimposed infection and pressure necrosis of adjacent tissues secondary to growth of the cystic masses.1
Case Report
A 69-year-old woman presented with a 25-year history of multiple slowly enlarging lesions on her scalp. The patient’s sister and mother had similar scalp masses. A lesion near the vertex of the patient’s head developed an ulceration, which prompted surgical consultation. An excisional biopsy of the ulceration revealed squamous cell carcinoma.
On physical examination, the patient’s scalp was studded with numerous mobile masses, ranging in size from 3 to 15 cm. The masses extended from the anterior hairline to the posterior hairline with most in the occiput and parietal regions. The masses varied in consistency from solid to fluctuant, and all were covered by hair. The excisional biopsy site, near the vertex, was well healed, and no other regions of ulceration or friable skin were present. There was no cervical or parotid lymphadenopathy.
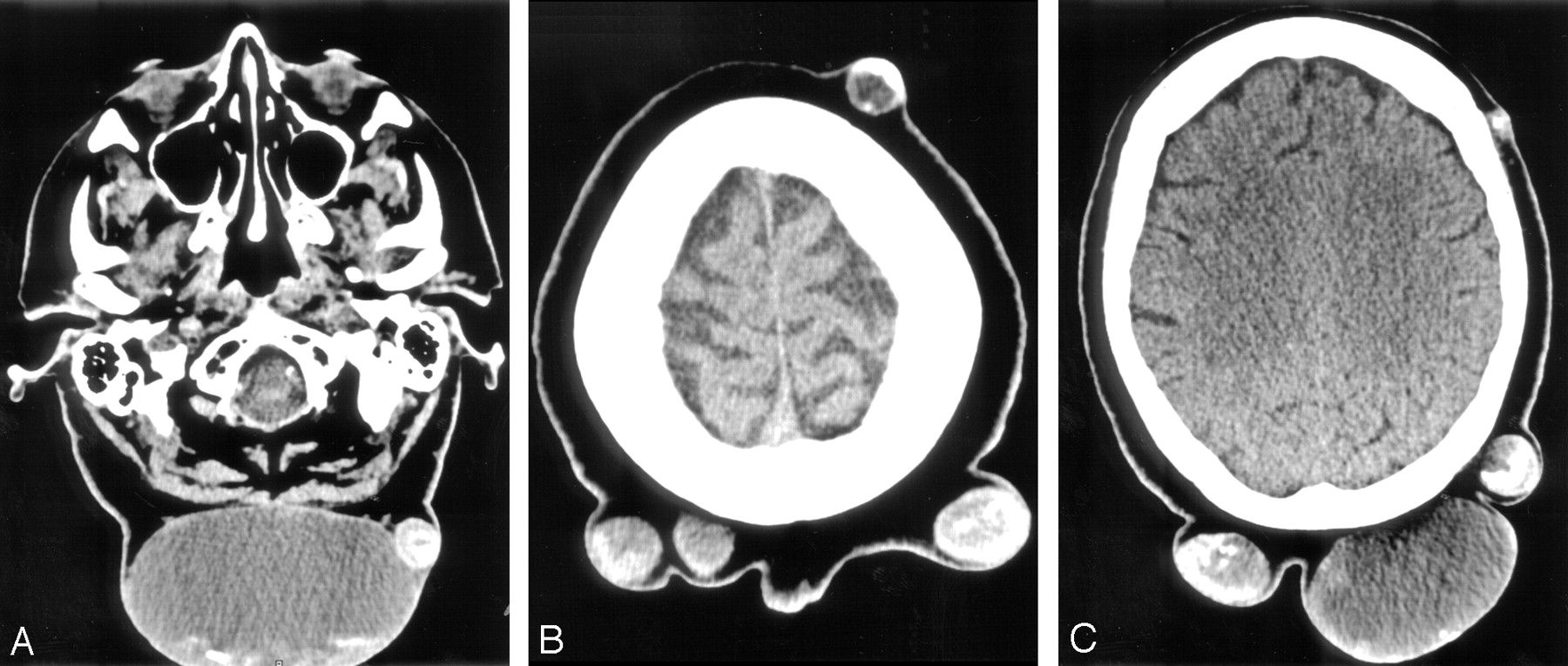
A CT scan of the head, with and without contrast, demonstrated multiple rim-enhancing ovoid complex cystic masses within the subcutaneous tissues over the scalp (Figs 1, 2A). An axial CT scan obtained through the skull base demonstrated 2 complex subcutaneous cystic masses of the posterior aspect of the upper neck (Fig 2A). The dominant mass had coarse regions of mineralization at the dependent portion, suggesting that this was a cystic structure containing relatively attenuated proteinaceous material. The second mass had a ringlike region of mineralization both surrounding and surrounded by soft-tissue attenuation. The complex cysts were well defined with centripetal nodularity of the cyst wall. No infiltration of the surrounding subcutaneous tissues was present. There was no enhancement of the cyst contents. The cyst contents ranged from 10 to 40 Hounsfield units (HU) with regions of calcifications measuring 300 HU. The calvaria was intact without erosion or periosteal reaction. A CT scan of the thorax demonstrated 4 nonspecific subcentimeter pulmonary nodules, 2 in each of the upper lobes. A previous CT study of the thorax was not available for comparison.

Scanogram demonstrates multiple soft-tissue masses involving most of the posterior scalp, extending caudally to involve the posterior cervical region.

A, Axial CT image obtained through the skull base demonstrates 2 complex subcutaneous cystic masses of the posterior aspect of the upper neck. The dominant mass has coarse regions of mineralization at the dependent portion. The smaller mass also has calcifications.
B, Axial CT image obtained caudal to the skull vertex demonstrates multiple masses with varying degrees and regions of mineralization.
C, Axial noncontrast CT image obtained through the centrum semiovale demonstrates that the degree of mineralization is not related to the size of the masses.
A preliminary clinical diagnosis of malignant transformation of a Turban tumor was made, and the patient was taken to surgery for total scalp removal with split-thickness skin graft reconstruction. Turban tumor syndrome, also known as Brooke-Spiegler syndrome, presents in a fashion similar to that of pilar tumors. Patients present with multiple slowly enlarging scalp masses that can become large enough to cover the patient’s head. Like pilar tumors, Turban tumor syndrome typically affects elderly women and is inherited in an autosomal-dominant fashion. Diagnosis is made by histopathology, which reveals cylindromas, tumors of the apocrine sweat glands.2 The size and location of the masses, as well as the clinical history, were suggestive of Turban tumor syndrome as well as pilar tumors. Forehead and posterior scalp frozen section margins were evaluated and found to be free of tumor.
The gross specimen included the entire scalp. The scalp contained multiple large nodular cysts covered with hair. The nodular lesions ranged from 1.2 to 12 cm in diameter. The smaller lesions were firm. The larger lesions were cystic and filled with material ranging from a cheesy solid to turbid fluid (Fig 3).

Photograph of a gross pathology specimen demonstrates 2 subcutaneous complex cysts that contain a viscous turbid fluid with multiple nodules firmly attached to the wall.
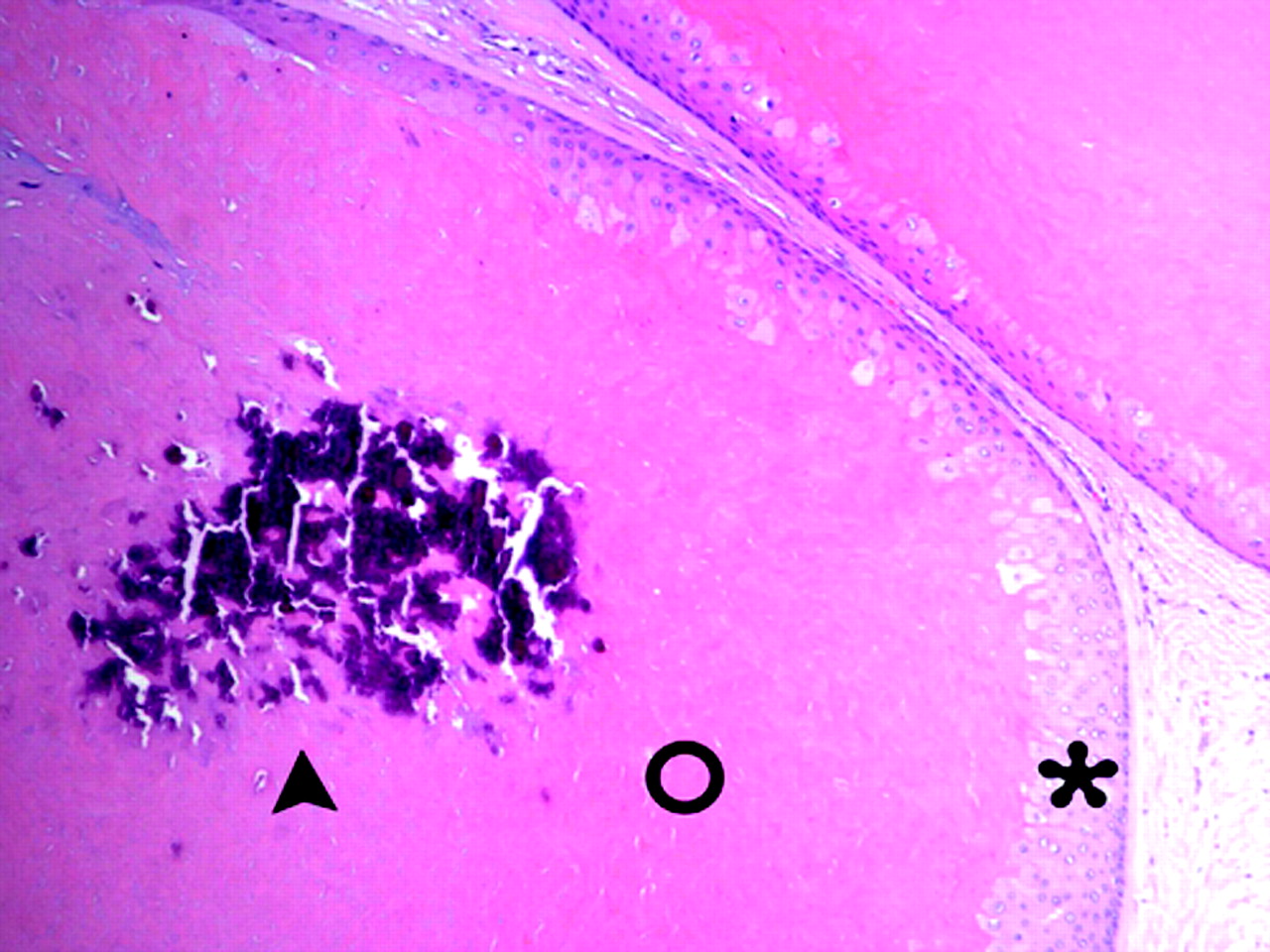
Histologic sections of the nodules showed cysts with eosinophilic centers lined by walls of stratified squamous epithelium (Fig 4). The epithelium demonstrated abrupt keratinization toward the center of the cysts. The cyst cavities were filled with attenuated, laminated keratin demonstrated by the large sheets of amorphous eosinophilic material in the center of the cysts. The basophilic material in the center of the amorphous eosinophilic material represents the focal keratin calcification. Lobulation of the cyst wall with piling up of the squamous epithelium, characteristic of a proliferating trichilemmal cyst, was seen (Fig 5). A final histopathologic diagnosis of multiple proliferating trichilemmal cysts was made.

Photomicrograph of cysts with eosinophilic centers lined by walls of stratified squamous epithelium. Arrowhead indicates calcifications in the center of the cyst; ○, keratin within cyst; and asterisk, the cyst wall (hematoxylin and eosin [H&E], original magnification, 100×).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Photomicrograph of lobulation of the cyst wall with piling up of the squamous epithelium (asterisk), characteristic of a proliferating trichilemmal cyst. Open circle indicates cyst cavity filled with keratin (hematoxylin and eosin [H&E], original magnification, 400×).
Discussion
The differential diagnosis included Turban tumor and trichilemmal cyst. Histopathology in the case presented failed to demonstrate typical apocrine features of Turban tumor syndrome, and the diagnosis of pilar tumors was made. Pilar tumors are usually large 2 to 15 cm, solid, or partially cystic masses located within the dermis or subcutaneous tissue. The masses can become exophytic and occasionally are associated with ulceration.3
From a histologic standpoint, trichilemmal cysts are characterized by the absence of intercellular bridges between the epithelial cells lining the cyst wall. The peripheral layers demonstrate a palisading arrangement, whereas cells close to the cyst cavity are swollen and filled with pale cytoplasm. The cyst cavity contains amorphous eosinophilic keratin. Foci of calcifications within the keratin occur in approximately 25% of cases (Fig 4).3 Proliferating trichilemmal cysts are characterized by regions of trichilemmal keratinization and, in some cases, focal epidermal keratinization. The cyst wall shows lobulation with piling up of the squamous epithelium (Fig 5). There may also be cellular atypia, vacuolated cells, focal necrosis, squamous eddies, and scattered mitoses. Histologic characteristics of a benign proliferating trichilemmal cyst resemble those of squamous cell carcinoma. Characteristics supporting the diagnosis of proliferating trichilemmal cyst instead of squamous cell carcinoma include cyst formation, trichilemmal keratinization, calcification, and the absence of a premalignant epidermal lesion.3 It has been speculated that a proliferating trichilemmal cyst is a variant of squamous cell carcinoma; however, this belief is not widely accepted.4,5 Currently, the diagnosis of a malignant proliferating trichilemmal tumor usually requires the lesion to have some areas of an underlying benign component in addition to extensive cellular atypia and invasion of adjacent structures.3
Radiographic findings include the presence of multiple complex subcutaneous solid or cystic masses of the scalp (Fig 1). The cystic masses contain attenuated proteinaceous material with coarse calcifications that may layer dependently (Fig 2A). The masses may also demonstrate ringlike patterns of mineralization not related to size of the masses (Fig 2A–C). Malignant radiographic characteristics include local invasion into the calvaria, meninges, and dural sinuses.5 Other findings suggestive of malignancy on imaging may include enhancement of the soft-tissue components in the periphery of the cyst and infiltration of the surrounding soft tissues. The patient presented demonstrated no evidence of bony erosion, periosteal reaction, soft-tissue infiltration, or involvement of the dural sinuses (Fig 2). CT is the technique of choice to monitor bony erosion, whereas MR imaging would be more suitable to assess soft-tissue infiltration and dural involvement.
Simple trichilemmal cysts are often easily enucleated, in contrast to proliferating trichilemmal cysts, which require wide local excision to prevent recurrence.1 Because of the malignant potential of proliferating trichilemmal cysts, management includes wide local excision with continued long-term surveillance.5 Often, as in the case presented, total scalp excision with reconstruction is the treatment of choice. Recurrence of pilar tumors is common after complete excision. Malignant transformation of the epithelial lining into squamous cell carcinoma or spindle cell carcinoma is rare.6,7 Local invasion, lymphatic, and/or hematogenous metastatic spread has been reported in approximately 30 cases in the literature.7
References
- Received April 12, 2005.
- Accepted after revision May 4, 2005.
- Copyright © American Society of Neuroradiology