Abstract
BACKGROUND AND PURPOSE: Brain tissue viability depends on cerebral blood flow (CBF) that has to be kept within a narrow range to avoid the risk of developing ischemia. The aim of the study was to evaluate by 64-section CT (VCT) the cerebral perfusion modifications in patients with severe carotid stenosis before and after undergoing carotid artery stent placement (CAS) with a cerebral protection system.
MATERIALS AND METHODS: Fifteen patients with unilateral internal carotid stenosis (≥70%) underwent brain perfusional VCT (PVCT) 5 days before and 1 week after the stent-placement procedure. CBF and mean transit time (MTT) values were measured.
RESULTS: Decreased CBF and increased MTT values were observed in the cerebral areas supplied by the stenotic artery as compared with the areas supplied by the contralateral patent artery (P < .001). A significant normalization of the perfusion parameters was observed after the stent-placement procedure (mean pretreatment MTT value, 5.3 ± 0.2; mean posttreatment MTT value, 4.3 ± 0.18, P < .001; mean pretreatment CBF value, 41.2 mL/s ± 2.1; mean posttreatment CBF value, 47.9 mL/s ± 2.9, P < .001).
CONCLUSIONS: PVCT is a useful technique for the assessment of the hemodynamic modifications in patients with severe carotid stenosis. The quantitative evaluation of cerebral perfusion makes it a reliable tool for the follow-up of patients who undergo CAS.
Carotid artery stenosis, with its thromboembolic complications causing cerebral ischemia,1,2 can be successfully treated by carotid endarterectomy (CEA), which significantly reduces the risk of stroke in both symptomatic and asymptomatic patients, as compared with medical therapy alone.3,4 Alternatively, carotid artery stent placement (CAS) is increasingly used thanks to the development of safe and effective protection systems that help reduce the periprocedural neurologic complications.5,6 Two recent registry studies (ARCHeR, Caress) have demonstrated that CEA and CAS are comparable in terms of periprocedural complications in symptomatic or asymptomatic patients not presenting comorbidities.7,8 The overlapping percentage of complications between these 2 techniques at 30 days is 2%.
Cerebral perfusion changes, such as an asymmetry in the hemisphere corresponding to the affected carotid artery, have been observed in patients with unilateral severe carotid stenosis, however without a direct correlation to the degree of stenosis.9,10 A measure of perfusion disturbance as provided by cerebral blood flow (CBF) and mean transit time (MTT) appears to be helpful in evaluating brain with a risk of developing a stroke and eventually in guiding the therapeutic decisions especially in acute ischemic events.11
Positron-emission tomography (PET), single-photon emission CT (SPECT), xenon-enhanced CT (Xe-CT), perfusion CT (PCT), and MR imaging have all been applied in the study of brain hemodynamics. However, the scarce availability of PET and SPECT in most radiology departments or the difficulty in obtaining a quantitative measurement by MR imaging has drawn attention for >20 years toward Xe-CT,12 whose demonstrated accurate measurement of perfusion13 has permitted the differentiation of patients with normal CBF14 from those with reversible neurologic deficits (CBF, 10–20 mL/100 g per minute) or those with infarction (CBF < 10 mL/100 g per minute).13 PCT, validated by comparison with Xe-CT13,14 and widely available in most radiology departments, can be easily performed at the end of a CT scanning and has, therefore, further simplified the approach to brain perfusion evaluation,15,16 adding further information about hemodynamic parameters such as MTT and cerebral blood volume. More recently, the perfusion study by 64-section CT (VCT), allowing the assessment of a brain volume ≤4 cm, has offered an improved tool of investigation.
The aim of our study was to measure by brain perfusional VCT (PVCT) the hemodynamic parameters in the cerebral hemisphere supplied by the severely stenotic internal carotid artery (ICA), in a group of patients undergoing an endovascular treatment with a protection device. The hypothesis is that CBF and MTT values in the hemisphere on the side of the carotid stenosis will be abnormal before the procedure and will approach the values on the contralateral side after the procedure.
Materials and Methods
Preprocedural Evaluation
Fifteen patients (11 men, 4 women; mean age, 67 years; range, 58–79 years), with a unilateral ≥70% stenosis (as defined by the North American Symptomatic Carotid Endarterectomy Trial criteria)17 of the ICA, were enrolled in the study. The degree of stenosis ranged from 70% to 95%. The contralateral ICA was either normal or with an asymptomatic <60% stenosis. Our institutional review board approved the study protocol, and informed consent was obtained from all patients.
Angio-CT multisection scanning (LightSpeed VCT; GE Healthcare, Milwaukee, Wis) was performed a few days before perfusion to assess the degree of stenosis and the length and morphology of the plaque and to evaluate the circle of Willis. The protocol used was the following: An axial precontrast brain CT (120 kV; 250 mA; section thickness, 5 mm) was performed. For CT angiography, 100 mL of a 370-mg/dL nonionic iodinated contrast agent was injected by using an automatic injector at a rate of 4 mL/s. Acquisition parameters were the following: 120 kV; 150–350 smart mA; rotation time, 0.9 seconds; SmartPrep (GE Healthcare) helical scan from aortic arch to skull vertex; no gantry angle.
Fifteen lesions were treated, including 1 postradiotherapy stenosis, 3 postendarterectomy restenotic lesions, and 2 poststent-placement restenotic lesions (1 patient already treated in our department with stent placement and 1 previously treated at another institute). An independent neurologist performed a preprocedural neurologic examination. Eight patients (53.3%) of the 15 were classified as symptomatic, 3 (20%) because of a transient ischemic attack and 5 (33.3%) because of a stroke within 6 months before the stent-placement procedure. Of the 5 patients with a previous stroke, only 3 presented slight hemiparesis (Table 1).
Demographics and clinical data of patient population
Drug Therapy
All patients were treated with aspirin (100–400 mg/day) and clopidogrel (75 mg/day) in 12 patients (80%) or ticlopidine (500 mg/day) in 3 patients (20%), starting at least 48 hours before the procedure. During the procedure, 50–100 U/Kg of heparin bolus was administered, maintaining the activated clotting time around 300; and 0.5/1.0 mg of atropine, before dilation with the intrastent balloon to prevent bradycardia. Following the procedure, all patients received aspirin quoad vitam and clopidogrel or ticlopidine for 6 weeks. Neurologic examination was performed before and after the procedure and at follow-up.
Stent-Placement Procedure
All procedures were performed in the angiosurgery department by 2 interventional radiologists under anesthesiologic assistance. Invasive arterial pressure and oximetry monitoring were performed with the patient under mild sedation but conscious. A filter protection device (EPI filter; Boston Scientific, Natick, Mass) and a self-expandable stent (Carotid Wallstent; Boston Scientific) were used in all patients to stent the entire lesion. All stents were postdilated with noncompliant balloons (range, 5–6 mm). The mean procedural time was 5.3 minutes (range, 3.6–22 minutes).
Outcomes and Follow-Up
Technical success was defined as the complete deployment of the stent with a residual stenosis lower than 30% and normal intracranial circulation as assessed by the postprocedural angiography. All 15 procedures were technically successful. No postprocedural complications, according to the classification reported by Mathur et al,18 were recorded. All patients underwent neurologic examination the day after the procedure.
Imaging Protocol
The CT scanner used was a LightSpeed VCT with the perfusion software developed by Ting-Yim Lee and his group.15,16,19 The following protocol was performed 5 days before and 7 days after the stent-placement procedure: A precontrast study of the whole brain (thickness, 2.5 mm for the infratentorial region; 140 kV, 180 mA, and 5 mm for the supratentorial region, 120 kV, 250 mA; no overlapping) was performed. PVCT data were measured from the upper limit of the fourth ventricle to the centrum semiovale white matter; the gantry tilt was perpendicular to the posterior segment of the superior sagittal sinus. A 40-mL bolus of 370 mg/dL nonionic iodinated contrast agent followed by 40 mL of saline was administered into an antecubital vein by using an automatic injector at a rate of 4 mL/s for all patients.
Acquisition parameters were 80 kV and 160 mA, and CT scanning started 7 seconds after the contrast injection. Images were acquired and reconstructed at a temporal sampling rate of 16 images per second. Each section was 2.5 cm thick, and all sections were of the same thickness, resulting in a series of 800 per 50 seconds of acquisition time and a total of 50 data per section. Hemodynamic parameters (MTT and CBF maps) were measured in all 16 sections by positioning a region of interest over each hemisphere in the vascular territory of distribution of the ICA (Fig 1), by using the cortical and intracerebral boundaries proposed by van Laar et al.20

A, An example of ICA flow territory (red) in a population with a nonvariant type of circle of Willis. B and C, CBF (mL/100 g per minute) and MTT (seconds) perfusion maps of 1 patient with a nonvariant type of circle of Willis, showing the regions of interest placed on the territory of distribution of the ICA. No CBF and MTT changes are appreciable on visual inspection.
The imaging perfusion CT scan of each section was analyzed separately off-line at a workstation by using CT software (CT Perfusion 3, Advantage 4.2; GE Healthcare). The 5 patients with a previous stroke presented either small cortical infarcts (2 patients) or small white matter subcortical hypoattenuation (3 patients) that did not appear to affect the perfusion measurements. Pixels with signal intensity higher than 2 SDs above the brain mean value, supposed to represent blood vessels or CSF, were excluded from all regional analyses.
Statistical Analysis
The Shapiro-Wilk test was used in testing for normality. Because some of the datasets failed the test of normality, nonparametric tests were used. For the statistical analysis, the nonparametric Mann-Whitney U test was performed when independent data were compared. The Wilcoxon matched pairs test was used to compare data not entirely independent of each other (ie, before/after treatment). P values ≤ .05 were considered statistically significant. Statistical analysis was performed by using a commercially available software package (Prism 4; GraphPad, San Diego, Calif).
Results
Individual pre- and postprocedural CBF and MTT values on the stenotic side are presented in Table 2. Mean MTT and CBF values on the normal and stenotic sides pre- and postprocedure are presented in Table 3. In each patient on the stenotic side, the CBF increased and the MTT decreased following stent placement. In the hemisphere corresponding to the stenotic side, the mean pretreatment MTT was significantly higher and the mean pretreatment CBF was significantly lower than that on the contralateral side (mean stenotic side pretreatment MTT, 5.3 ± 0.2 seconds; mean contralateral MTT, 4.3 ± 0.17 seconds, P < .001; mean stenotic side pretreatment CBF, 41.2 ± 2.1 mL/100 g per minute; mean contralateral CBF, 49.4 ± 3.0 mL/100 g per minute, P < .001). The perfusion difference changed after the stent-placement procedure, showing a significant increase in the mean CBF (mean stenotic side pretreatment CBF, 41.2 ± 2.1 mL/100 g per minute; mean stenotic side posttreatment CBF, 47.9 ± 2.9 mL/100 g per minute, P < .001) and a decrease in the mean MTT (mean stenotic side pretreatment MTT, 5.3 ± 0.2 seconds; mean stenotic side posttreatment MTT, 4.3 ± 0.18 seconds, P < .001) on the affected side. Following the procedure, the affected side had CBF and MTT values that, statistically, were not significantly different from those on the contralateral normal side. On the contralateral normal side, no statistically significant differences in CBF and MTT were noted before and after the procedure.
CBF (mL/100 g per minute) and MTT (seconds) values in the hemispheres supplied by the stenotic ICA before (Pre) and after (Post) the stenting procedure
Mean MTT and CBF values pre- and post-CAS
Discussion
The PCT technique uses first-pass tracer methodology after bolus infusion of intravenous iodinated contrast material. It was initially described in 198021,22 but has been only recently fully developed and refined15,16 so that the measurement of perfusion parameters has become clinically feasible and can be carried out at the end of a routine cerebral CT examination. This is also due to the advent of high-speed spiral CT scanners and faster image-reconstruction software such as PVCT, which allow the study of a volume of ≤4 cm in thickness. In addition, CT perfusion allows a quantitative perfusional evaluation, whereas MR imaging provides only a qualitative assessment of brain perfusion by comparing the 2 cerebral hemispheres.
We used PVCT to evaluate the cerebral hemodynamic modifications in cerebral hemispheres of a group of patients with severe carotid stenosis, before and after stent placement. We observed an average degree of CBF reduction in the patients that can be considered in the low-normal range of brain perfusion (normal values, 46 ± 24 mL/100 g per minute),14 therefore without any clinical ischemic relevance. However, we believe that the main interest of our findings consists in the constant reduction in brain perfusion detected in the hemisphere corresponding to the stenotic carotid artery, compared with the contralateral normal hemisphere. The neuropsychologic consequences of an ischemic event are well known,23 though generally neglected because the attention of the physician is driven toward the more striking and invalidating motor deficits. However, recent articles have demonstrated that even asymptomatic patients with an elevated ICA luminal narrowing show higher depression scores or reduced neuropsychologic test performances that seem to be reversed by CAS.24–26
It is, therefore, tempting, in view of these works on the neuropsychological effect of carotid stenosis, to hypothesize that the low-normal perfusion observed in our patient population, reversed by the stent-placement procedure, could be the cause of serious long-term effects consisting of either clinically evident depression, severely reduced attention, or memory impairment, ultimately perhaps contributing to the development of dementia.
The increasing number of endovascular therapies for the treatment of carotid artery stenosis performed during the last few years has intensified the need for monitoring the outcome of the procedures. We believe that our findings could strengthen the importance of performing PCT, in addition to the standard CT examination, before and after CAS because it would add valuable information for a more thorough patient assessment.
Seven of our patients were asymptomatic with a high-grade (≥80%) ICA stenosis. Indication for treatment in asymptomatic patients is still argued, and no clear-cut consensus has been reached so that there is still controversy, for example, over the degree of stenosis that is an indicator for intervention.27 In general, for asymptomatic patients with 60%–90% stenosis, the benefit/risk ratio is considered smaller compared with that in symptomatic patients. However, in our opinion, it is beneficial to treat the stenosis in patients with life expectancy longer that 5 years and surgical risk <3%.
According to van Laar et al,20 we analyzed large vascular areas placing freehand-drawn regions of interest in the largest areas of the brain supplied by the ICA.
Our data demonstrate that the normalization of the perfusion parameters occurs in all patients as soon as 1 week after the stent-placement procedure (Fig 2) (P < .001). A recent study published by Trojanowska et al9 showed a trend toward hemodynamic normalization at 3 days poststenting but an incomplete normalization in a small percentage of patients at 6 months. The selection of patients, the interventional procedure performed, and the volume of study could all account for the differences.

{kind=link}
{kind=link}
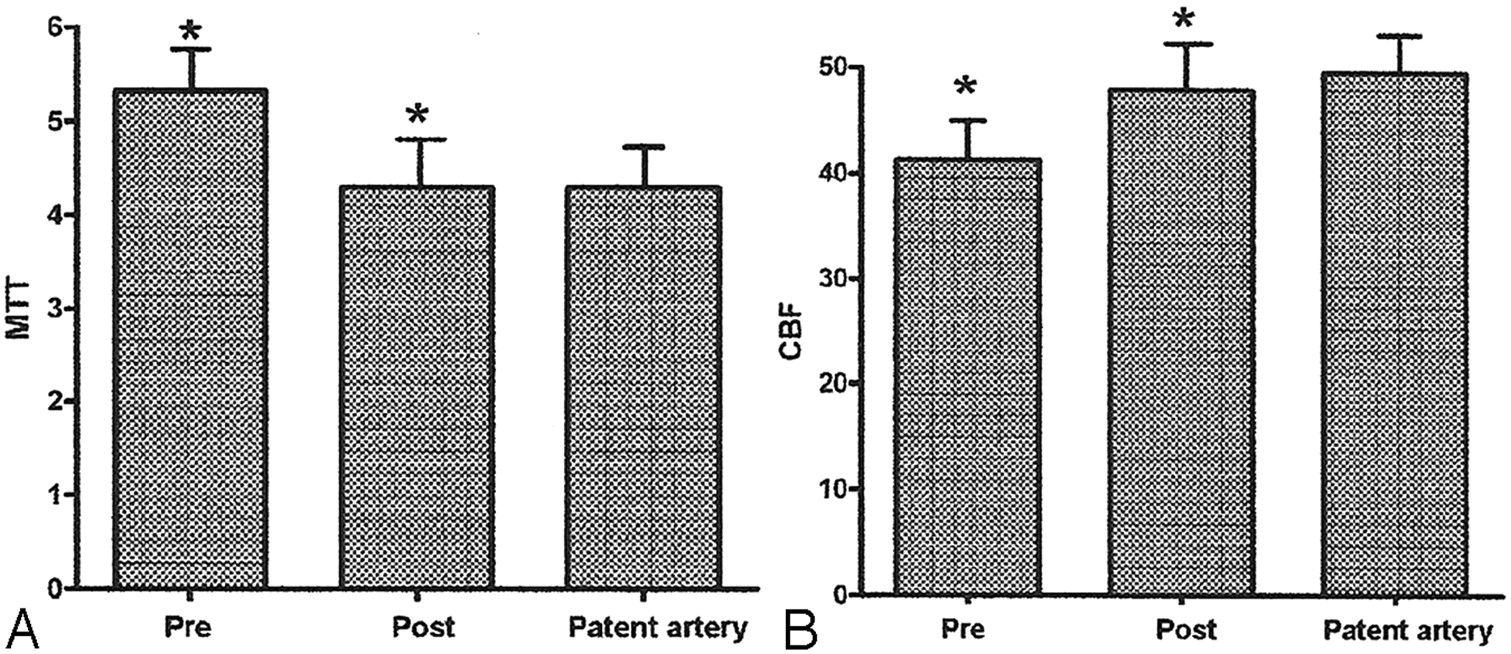
A and B, Differences between mean MTT (seconds) (A) and mean CBF (mL/100 g per minute) (B) values measured 5 days before (pre) and 1 week after (post) the stent-placement procedure. The patent artery refers to the contralateral normal hemisphere. Asterisk indicates P < .001.
Most interesting, Sanchez-Arjona et al28 have shown, with a different method of study, significant hemodynamic changes in the anterior brain circulation, ipsilateral to CAS at 6 hours after the procedure.
Several authors have demonstrated the high frequency of anatomic variants, such as a missing A1 segment of the anterior cerebral artery or a fetal-type posterior cerebral artery29–31 and pointed out their relevance with respect to an accurate prediction of blood flow territories. This is why all subjects examined had a nonvariant-type circle of Willis.
Conclusions
PVCT is a useful technique for the assessment of the hemodynamic modifications in patients with severe carotid stenosis. The quantitative evaluation of cerebral perfusion makes it a reliable tool for the follow-up of patients who undergo CAS. However, further long-term follow-up perfusion studies are needed to assess the hemodynamic outcome of CAS in patients with variant types of the circle of Willis.
References
- Received April 12, 2007.
- Accepted after revision November 16, 2007.
- Copyright © American Society of Neuroradiology