Abstract
BACKGROUND AND PURPOSE: Arterial remodeling may enable atherosclerotic disease without luminal stenosis. We sought to assess the prevalence and characteristics of atherosclerosis in angiographically normal carotid arteries.
MATERIALS AND METHODS: Forty-six arteries with 0% stenosis by MRA were evaluated with multicontrast carotid MR imaging at 3T. For each artery, the percentage wall volume (wall volume/[lumen volume + wall volume] × 100%) and the presence versus absence of an LRNC, calcification, IPH, and fibrous cap rupture were recorded. In addition, the relative size of each plaque component (eg, percentage LRNC = LRNC volume/wall volume × 100%), when present, was calculated.
RESULTS: The mean of percentage wall volume in arteries with 0% stenosis was 43.0 ± 6.9% with a range from 31.6% to 60.1%. An LRNC was present in 67.4% (31/46) of arteries, calcification was present in 65.2% (30/46), IPH was present in 8.7% (4/46), and fibrous cap rupture was present in 4.3% (2/46). In arteries with an LRNC (n = 31), the average percentage LRNC volume was 8.8 ± 7.3% with a range from 1.0% to 31.5%. For calcification (n = 30), the mean percentage calcification volume was 3.8 ± 4.2% with a range of 0.1%–17.4%. The mean percentage IPH volume (n = 4) was 2.7 ± 1.7% with a range of 0.5%–4.1%.
CONCLUSIONS: These findings indicate that stenosis by MRA may underestimate the presence of carotid atherosclerosis, and they demonstrate the need for improved methods for accurately identifying carotid atherosclerotic plaque severity.
Abbreviations
- CB
- carotid bulb
- CCA
- common carotid artery
- CE
- contrast-enhanced
- ECST
- European Carotid Surgery Trial
- ETL
- echo-train length
- HDL
- high-density lipoprotein
- ICA
- internal carotid artery
- ImQ
- image quality
- IPH
- intraplaque hemorrhage
- LDL
- low-density lipoprotein
- LRNC
- lipid-rich necrotic core
- MIP
- maximum intensity projection
- MRA
- MR angiography
- NASCET
- North American Symptomatic Carotid Endarterectomy Trial
- PDW
- proton-attenuation weighted
- SI
- signal intensity
- T2W
- T2-weighted
- TOF
- time-of-flight.
Luminal stenosis is the current standard for assessing the risk of stroke from carotid atherosclerotic disease.1 Several large prospective studies have established the value of stenosis measurement for disease severity and the risk of stroke in patients with moderate- and severe-grade symptomatic carotid artery stenosis.2–5 However, luminal stenosis may be unreliable in asymptomatic patients and in symptomatic patients with low-grade stenosis. The ECST reported that 43.8% of the 3018 individuals with symptomatic carotid disease had <30% stenosis.6 The NASCET found that among patients with <50% stenosis, the 5-year rate of any ipsilateral stroke was 22.2%.3 Although each trial used a different reference standard during the stenosis calculation (approximation of the carotid bulb for ECST, distal normal internal carotid artery for NASCET), these findings indicate that regardless of the denominator used, stenosis may be an incomplete measure of atherosclerotic disease severity.
Accordingly, Babiarz et al7 have demonstrated that carotid atheroma was frequently identified by MR imaging in arteries with minimal angiographic stenosis. In addition, Saam et al8 reported a notably high occurrence (approximately 30%) of carotid plaques with IPH and fibrous cap rupture in arteries with ≤ 50% stenosis. In arteries with only 1%–15% stenosis, these features were present in 8.1% of lesions.8 In this study, we sought to extend these previous investigations7,8 and determine the prevalence of atherosclerotic disease and plaque compositional features in angiographically normal arteries (ie, 0% stenosis) identified in subjects with known carotid atherosclerotic disease in the contralateral artery.
Materials and Methods
Study Population
Individuals with at least 1 carotid artery with >50% stenosis by duplex sonography were serially recruited for MR imaging of their bilateral carotid arteries. At the time of MR imaging, all participants provided answers to a standardized health questionnaire, had their height and weight measured, and underwent phlebotomy. The study procedures and consent forms were reviewed and approved by the institutional review board before study initiation.
MR Imaging Protocol
Between February 2007 and September 2007, 72 participants were enrolled and underwent imaging on a 3T scanner (Signa Excite; GE Healthcare, Milwaukee, Wisconsin) with bilateral phased array 4-element surface coils. A standardized MR imaging protocol9 adapted for imaging at 3T10 was used to acquire transverse images of the carotid artery centered at the bifurcation of the artery with greater duplex stenosis. 2D T1-weighted images,11 2D multisection double inversion recovery PDW and T2-weighted black-blood images,12 and 3D TOF bright-blood angiograms were acquired. Imaging parameters for each weighting were as follows: T1-weighted (TR/TE, 800/11 ms; ETL, 10; 16 sections; scanning time, 5 minutes 58 seconds), T2-weighted and PDW (TR/TE, 3500/70 and 12 ms; ETL, 12; 16 sections; scanning time, 3 minutes 40 seconds), and TOF (TR/TE, 21/2.9 ms; flip angle, 15°; 48 sections; scanning time, 2 minutes 4 seconds). All images were obtained with a section thickness of 2 mm, FOV of 140 mm, and matrix size of 512 × 512. In addition, a CE T1-weighted sequence11 was acquired 5 minutes after administration of 0.2-mmoL/kg gadopentetate dimeglumine (Magnevist; Bayer Schering Pharma, Berlin, Germany) was injected intravenously by using a power injector at 3 mL/s followed by a 20-mL saline bolus at the same speed.
At the time of contrast injection and before the CE T1-weighted acquisition, a 3D CE-MRA was acquired in the coronal plane with a 3D fast-spoiled gradient–recalled echo sequence (TR/TE, 2.5/1.2 ms; flip angle, 40°; section thickness, 2 mm; partitions per 3D slab, 36; matrix, 192 × 320; FOV, 320 mm; NEX, 1). K-space was ordered by using a 3D elliptic centric view order. A fluoroscopic triggering technique was used for detecting the contrast agent bolus. All sequences used the excitation pulses of the manufacturer and were not modified to reduce the specific absorption rate to shorten scanning time.
Image Analysis
All MRA images were interpreted bilaterally by consensus opinion of 2 trained reviewers blinded to clinical information and transverse carotid MR images. Luminal stenosis was quantified in both carotid arteries by using the NASCET criterion: (1-luminal diameter at the point of maximal narrowing/the diameter of the normal distal internal carotid artery) × 100%.3 All diameter measurements were acquired by using GE software (GE Healthcare Advantage workstation, Version 4.2.) and were oriented on MIP images.
For arteries with 0% stenosis by MRA, multicontrast transverse carotid MR images were interpreted by 2 trained reviewers blinded to clinical information. Each axial section was evaluated for ImQ (4-point scale: 1 = poor, 4 = excellent). Individual sections with ImQ <2 were excluded if they were at the proximal or distal coverage of the artery. Sections with ImQ <2 in the center of coverage resulted in exclusion of the entire artery. Only consecutive images of an artery with ImQ ≥2 were interpreted. Image-analysis software (CASCADE,13 Seattle, Washington) was used to draw the lumen and outer wall boundaries. Lumen volume, wall volume, and total vessel volume (lumen volume + wall volume) were used to calculate percentage wall volume (wall volume/total vessel volume × 100%), a measure of plaque burden similar to that proposed by Nissen et al14 during imaging investigations of the coronary arteries. The presence or absence of calcification, LRNC, IPH, and fibrous cap rupture was determined by using multicontrast imaging criteria that have been previously validated with histology.15–17 In brief, SI relative to the adjacent sternocleidomastoid muscle from corresponding pixels in different contrast weightings of the same axial location was used to determine the presence/absence of each feature as follows: 1) LRNC: isointense to hyperintense SI on T1-weighted, no contrast enhancement on CE-T1-weighted, hypointense SI on T2-weighted images; 2) IPH: hyperintense SI on T1-weighted and TOF images; 3) calcification: hypointense SI on T1-weighted, T2-weighted, PDW, TOF, and CE-T1-weighted images; and 4) fibrous cap rupture: irregular lumen boundary, absence of a fibrous cap on CE-T1-weighted, and juxtaluminal IPH on TOF images. The proportion of each component (LRNC, calcification, and IPH), when present, relative to the wall volume was also calculated (eg, percenage LRNC volume = LRNC volume/wall volume × 100%).
Data Analysis
Statistical analysis was performed only on arteries with ≤0% stenosis by MRA. Summary statistics for each metric are presented as mean ± SD and the range. Histogram analysis is also provided to characterize the variability of disease within this particular cohort. The prevalence of plaque features (LRNC, IPH, calcification) and fibrous cap status was determined at the artery level and for 3 segments: 1) the common carotid artery: >6 mm proximal to the flow divider; 2) the carotid bulb: <0–6 mm proximal to the flow divider; and 3) the internal carotid artery: ≥0 mm distal to the flow divider.
Results
There were 144 arteries from 72 subjects available for review. Eleven (7.6%) arteries had a noninterpretable MRA (motion artifacts, n = 4; missed arterial phase with venous contamination, n = 4; poor ImQ, n = 3). Of the remaining 133 arteries, 36.1% (48/133) had 0% stenosis on MRA. Of the 48 arteries with 0% stenosis by MRA, 95.8% (46/48) had sufficient ImQ of ≥2 on the corresponding multicontrast carotid MR imaging for interpretation of plaque morphology and composition. The demographic information for this subgroup (n = 46) is presented in the Table.
Demographics of the sample population
Plaque Burden (Percentage Wall Volume)
The mean ± SD of percentage wall volume in arteries with 0% stenosis was 43.0 ± 6.9%, with a range from 31.6% to 60.1% (Fig 1). Histogram analysis (Fig 2) indicated that a substantial number of subjects with 0% stenosis had a percentage wall volume >50%.

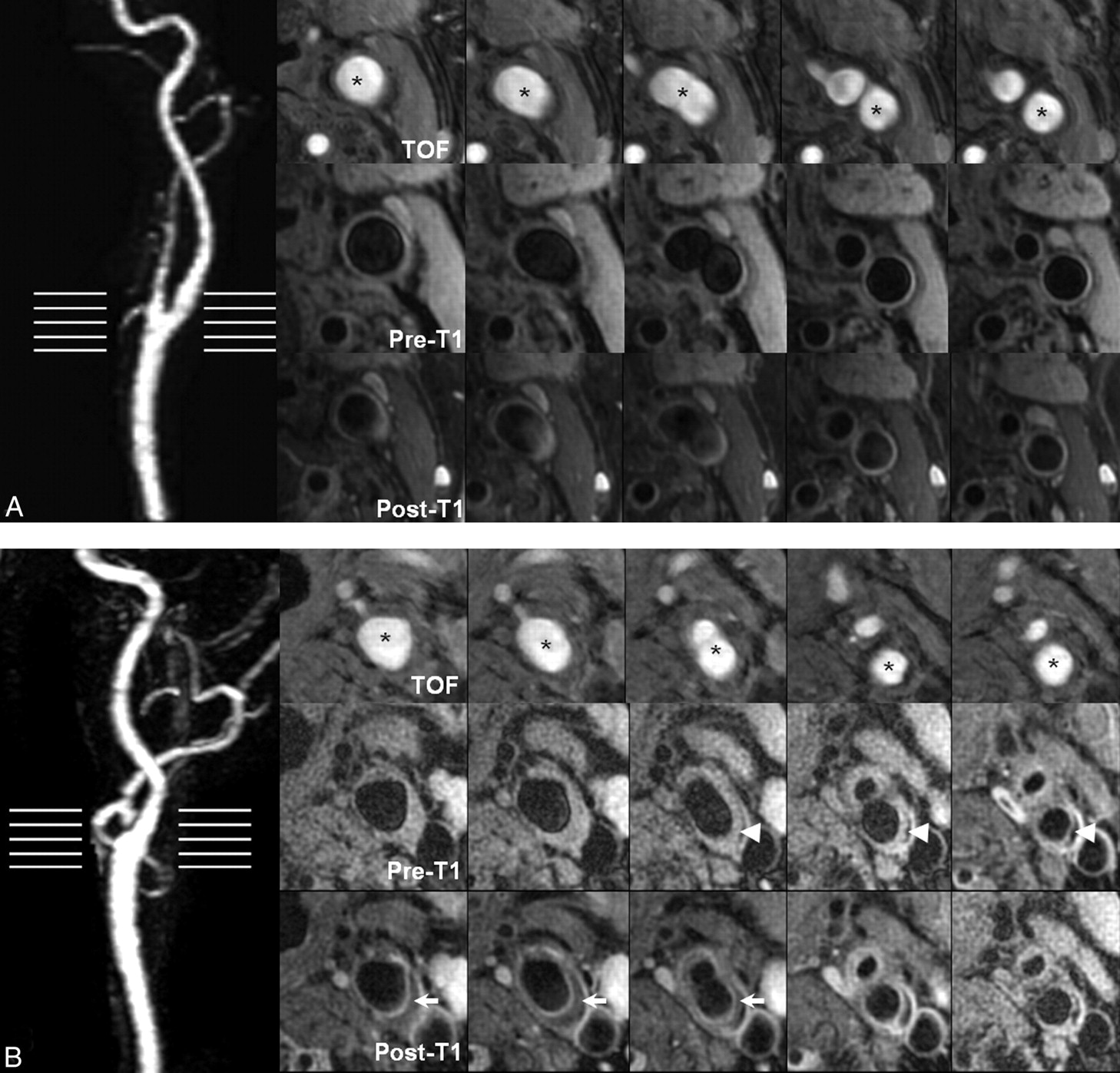
MIP and multicontrast carotid MR images of the left carotid artery from a 67-year-old woman (A) and a 62-year-old man (B). Transverse images are consecutive sections that correspond to horizontal lines on the MRA. A, There is 0% stenosis on MRA and no evidence of plaque formation at any axial location. B, There is substantial plaque with evidence of a LRNC (arrows) and calcification (arrowheads), though there is no evidence of stenosis on MRA. The asterisk indicates the lumen of either the CCA or ICA.

Histogram of plaque burden (percentage wall volume) for arteries with 0% stenosis on MRA.
Plaque Composition
A LRNC (Fig 1B) was present in 67.4% (31/46) of arteries, calcification was present in 65.2% (30/46), IPH was present in 8.7% (4/46), and fibrous cap rupture was present in 4.3% (2/46, Fig 3).

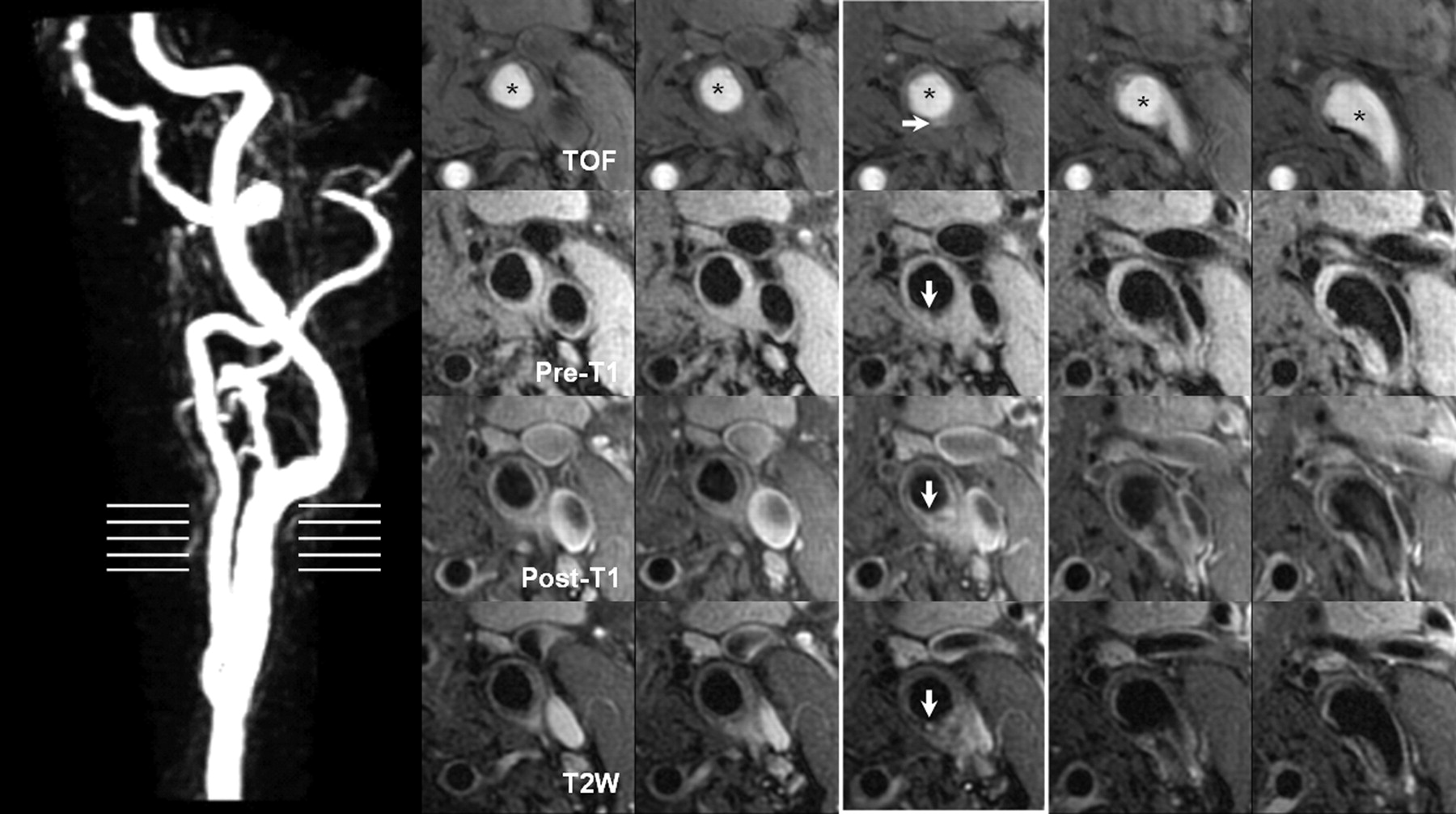
Transverse carotid plaque images and MIP of the left carotid artery were obtained from a 60-year-old woman. On the left side, MIP of the CE-MRA identifies a 0% stenosis at the left CCA. The horizontal lines indicate the level of the transverse carotid plaque images as shown on the right side. On the transverse images, a surface disruption (white arrow) is noted as hyperintense on the TOF and hypointense on the pre- and postcontrast T1-weighted, T2-weighted, and proton-attenuation images. This surface disruption is not identified on CE-MRA. The asterisk indicates the lumen of either the CCA or ICA.
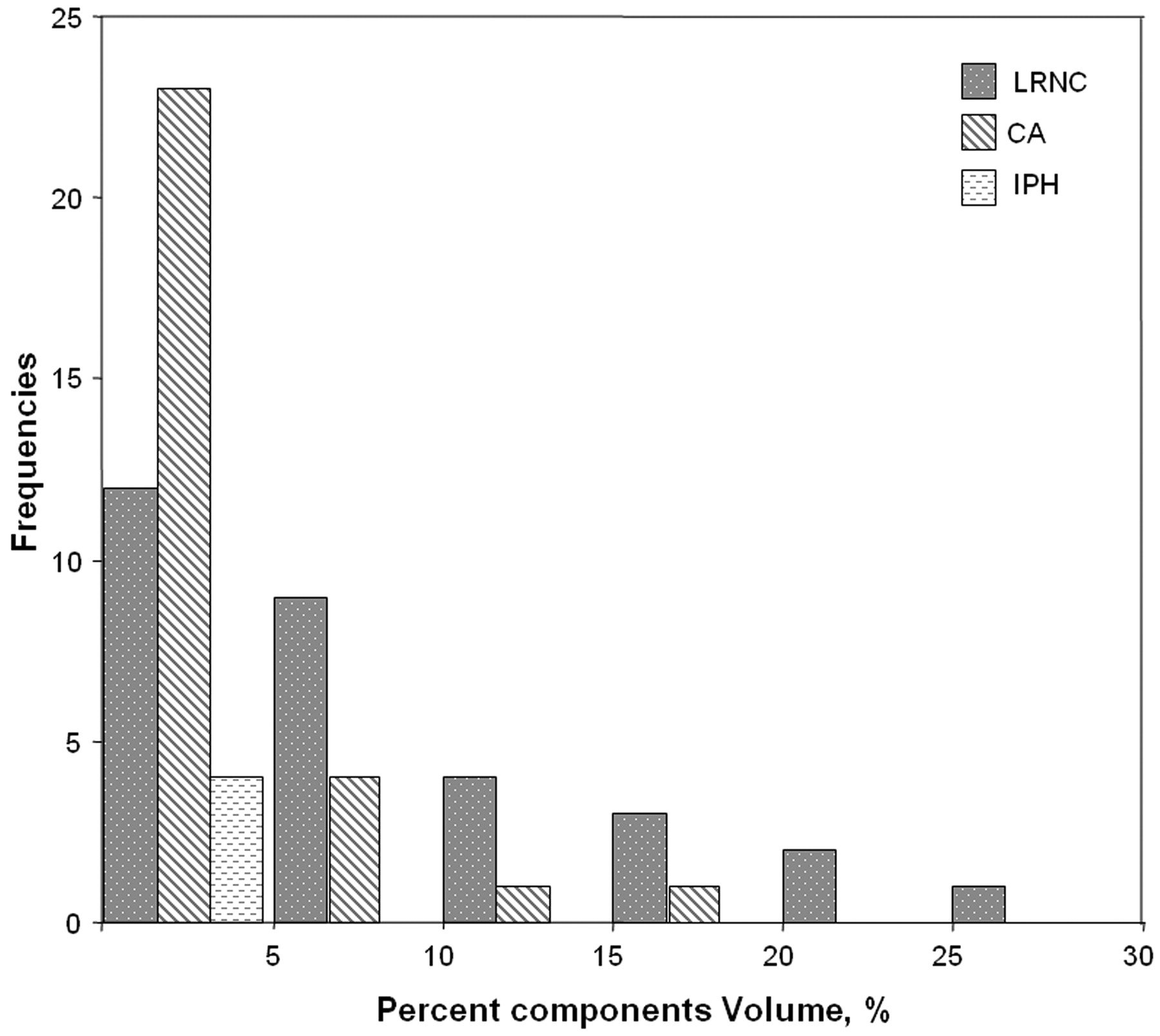
In arteries with an LRNC (n = 31), the average percentage LRNC volume was 8.8 ± 7.3% with a range from 1.0% to 31.5%. For calcification (n = 30), the mean percentage calcification volume was 3.8 ± 4.2%, with a range of 0.1%–17.4%. The mean percentage IPH volume (n = 4) was 2.7 ± 1.7%, with a range of 0.5%–4.1%. Histogram results for the volume of each plaque component are presented in Fig 4.

Histogram distribution for the size of each plaque component.
Segmental Distribution of Plaque Features
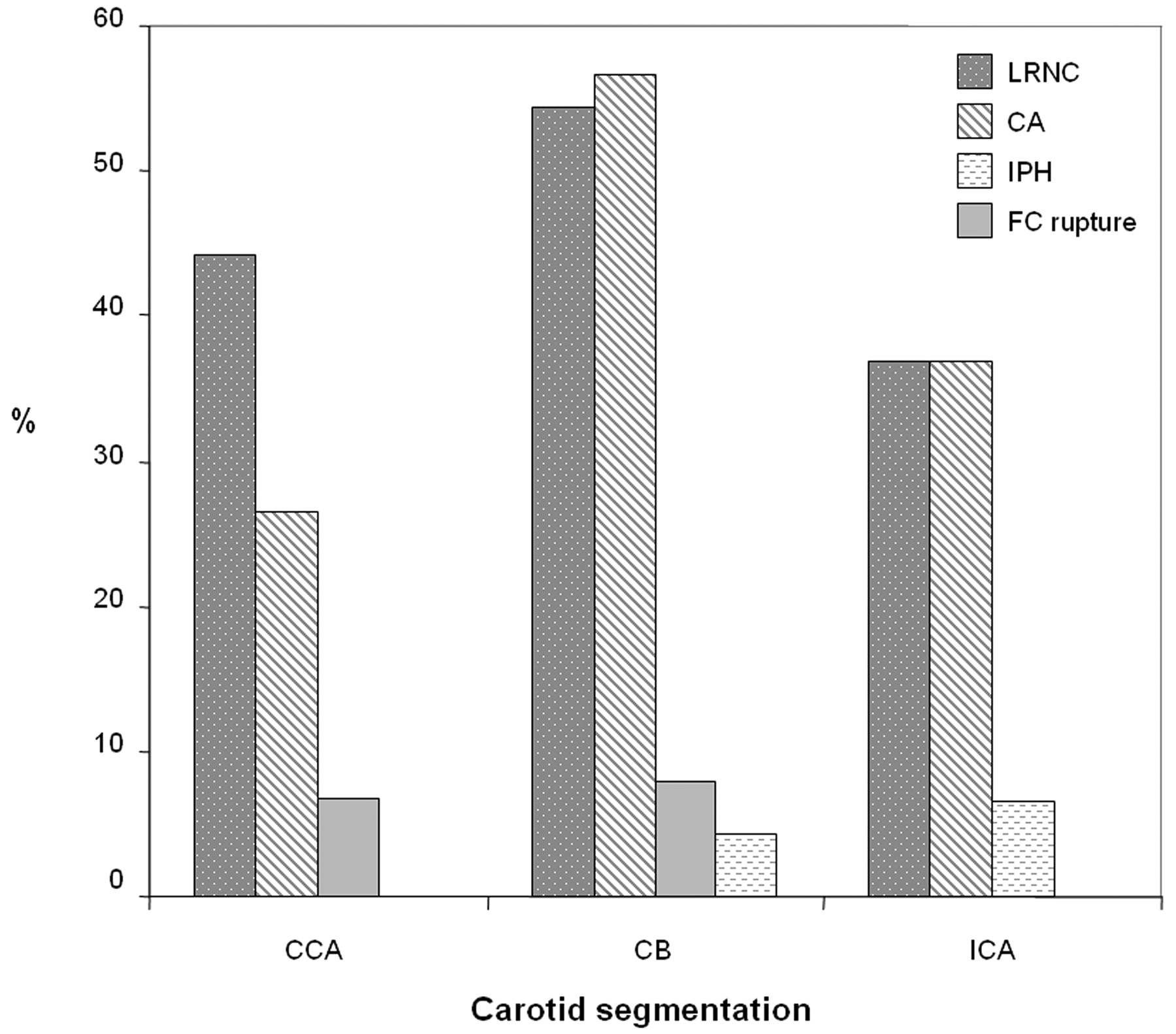
The prevalence of LRNC was highest in the carotid bulb (54.3%, Fig 5), followed by the common carotid artery (44.1%) and internal carotid artery (37.0%). The prevalence of calcification was also highest in the carotid bulb (56.5%), but prevalence in the internal carotid artery (37%) was greater than that in the common carotid artery (26.5%). IPH was not detected in the common carotid artery and had a similar prevalence in the internal carotid artery (6.5%) and carotid bulb (4.3%). In contrast, fibrous cap rupture was not present in the internal carotid artery and had a prevalence of 8% and 6.7% of lesions with an LRNC in the carotid bulb and common carotid artery, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of plaque features at each segment of the carotid artery. CCA: >6 mm proximal to the flow divider; CB: >0–6 mm proximal to the flow divider; ICA: ≥0 mm distal to the flow divider.
Discussion
In this study of angiographically normal carotid arteries, a broad spectrum of atherosclerotic disease was identified. Within this cohort, high-risk features such as IPH and fibrous cap rupture were not uncommon. However, given the extent of carotid disease in the contralateral artery (>50% stenosis by duplex sonography), our findings should not be extrapolated to an at-large population of subjects with angiographically normal carotid arteries. Rather, these findings highlight the potential limitations of traditional risk-stratification systems that implement stenotic severity as the principal criterion. In addition, our findings offer compelling evidence for vessel wall imaging in patients with appropriate clinical risk factors and/or a history of neurologic events, but negative imaging findings based on conventional lumenography.
The occurrence of carotid atherosclerotic disease without luminal compromise may be attributable to several factors. In 1987, Glagov et al18 described a process of outward arterial remodeling in the coronary arteries. They observed that luminal narrowing did not occur until the atherosclerotic lesion occupied >40%–50% of the internal elastic lamina area.18 In addition to this adaptive phenomenon, or separately, the morphology of the carotid bulb may contribute to the presence of lesions without angiographic changes. The transition between the common carotid artery and the flow divider (ie, the carotid bulb/sinus) is characterized by a localized dilation of the arterial lumen, which coincides with the presence of numerous baro- and chemoreceptors. Application of the NASCET criteria for measuring stenosis requires that a normal-appearing segment of the internal carotid artery be used as a reference.3 As such, in a normal artery, measurements from the carotid bulb compared with a reference segment of the internal carotid artery may yield a stenosis measurement <0%. We found that consistent with findings from a previous study,8 plaque compositional features occurred primarily at the carotid bulb. In addition, we found that a substantial number of subjects had a percentage wall volume >50%, which is the upper bound of the cutoff proposed by Glagov et al18 for the initiation of luminal narrowing. While these features may have resulted in luminal narrowing within the bulb consistent with the hypothesis of Glagov et al, the luminal diameter may have remained greater than the lumen of the internal carotid artery. An alternate approach to quantifying stenosis by angiography was used in the ECST.2 Stenosis was measured as the maximum percentage reduction in the relevant carotid artery. The relationship between the ECST and NASCET has been previously expressed by the following formula: ECST stenosis = 0.6 × NASCET stenosis + 40%.19 As such, this approach results in generally larger measures of stenosis than that by NASCET19 but requires extrapolation of where the nondiseased luminal boundary would be, which results in poor reader reproducibility.20 Collectively, these studies and the data presented herein offer compelling evidence that luminal stenosis alone may not be the strongest classifier of atherosclerotic disease severity.
A number of cross-sectional studies, both coronary and carotid, have indicated that fibrous cap rupture, IPH, and LRNC may represent the unstable atherosclerotic lesion.21–25 In the carotid artery, these features have been shown prospectively to be associated with a higher risk of plaque progression26 and future cerebrovascular events.27 As such, vessel wall imaging may provide critical information for discerning lesion stability, particularly in all asymptomatic and symptomatic lesions with <70% stenosis when treatment strategies remain ambiguous. Moreover, our data suggest that individuals with a history of an ischemic neurologic event may warrant carotid MR imaging in the absence of an identifiable etiology. In 1989, Sacco et al28 reported, in a prospective investigation of 1273 individuals with stroke, that 40% had infarcts of an undetermined cause. Subsequently, others have hypothesized that subclinical atherothromboembolism is the most likely etiology for cryptogenic stroke in older individuals or in patients with substantial atherosclerosis risk factors.29 The unique geometry of the carotid bulb and vascular remodeling may mask a stronger contribution to the etiology of stroke by the carotid artery than previously estimated by stenotic severity. Accordingly, vessel wall imaging may be necessary to better discriminate the origins of ischemic stroke.
Conclusions
Angiographically normal (0% stenosis) carotid arteries may have substantial plaque burden and a spectrum of compositional features, including IPH and fibrous cap rupture. Clinically, these findings indicate that vessel wall imaging may be necessary to better evaluate plaque stability across all levels of stenosis, particularly in patients with strong clinical risk factors. In addition, carotid MR imaging may be warranted in patients with angiographically normal carotid arteries and an unexplained etiology of ischemic stroke to rule out carotid atherosclerotic disease as a source of thromboemboli.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- Received April 1, 2009.
- Accepted after revision June 15, 2009.
- Copyright © American Society of Neuroradiology