Abstract
SUMMARY: JXG is a disorder classified under histiocytosis. It usually affects children and commonly presents with skin lesions. Intracranial lesions are uncommon and usually solitary. We present the case of a child who had extensive intracranial involvement with multiple enhancing solid lesions in the cerebellum, brain stem, thalami, and bilateral cerebral hemispheres on MR imaging.
Abbreviations
- JXG
- juvenile xanthogranuloma
JXG is a part of the spectrum of histiocytosis. Unlike the more commonly seen cutaneous lesions, intracranial lesions do not respond to medical management and require surgery.
Case Report
A 3-year-old child was admitted with generalized seizures, headache, dysarthria, and gait disturbance with weakness of the limbs since 1 year of age. He had a history of extensive macula-papular skin lesions from 8 months of age. Biopsy of the skin lesions revealed JXG. At that time, findings of sonography of the abdomen and a CT scan of the brain were normal. A contrast-enhanced MR imaging of the brain was requested in view of presenting symptoms. It revealed extensive intracranial involvement, with multiple lesions in the cerebellum, brain stem, thalami, and cerebral hemispheres. The lesions were of varying sizes. They were isointense on T1-weighted images and mildly hyperintense on T2-weighted images, with a mild degree of perilesional edema (Fig 1). The larger lesions were located in both hippocampi. All the lesions showed homogeneous contrast enhancement (Figs 2–5). Mild supratentorial hydrocephalous was seen secondary to compression and distortion of the aqueduct by the brain stem lesions. The results of a biopsy of 1 of the lesions revealed xanthogranulomas.

Axial T2-weighted MR image showing isohyperintense lesions in both thalami and frontoparietal lobes with mild perilesional edema.

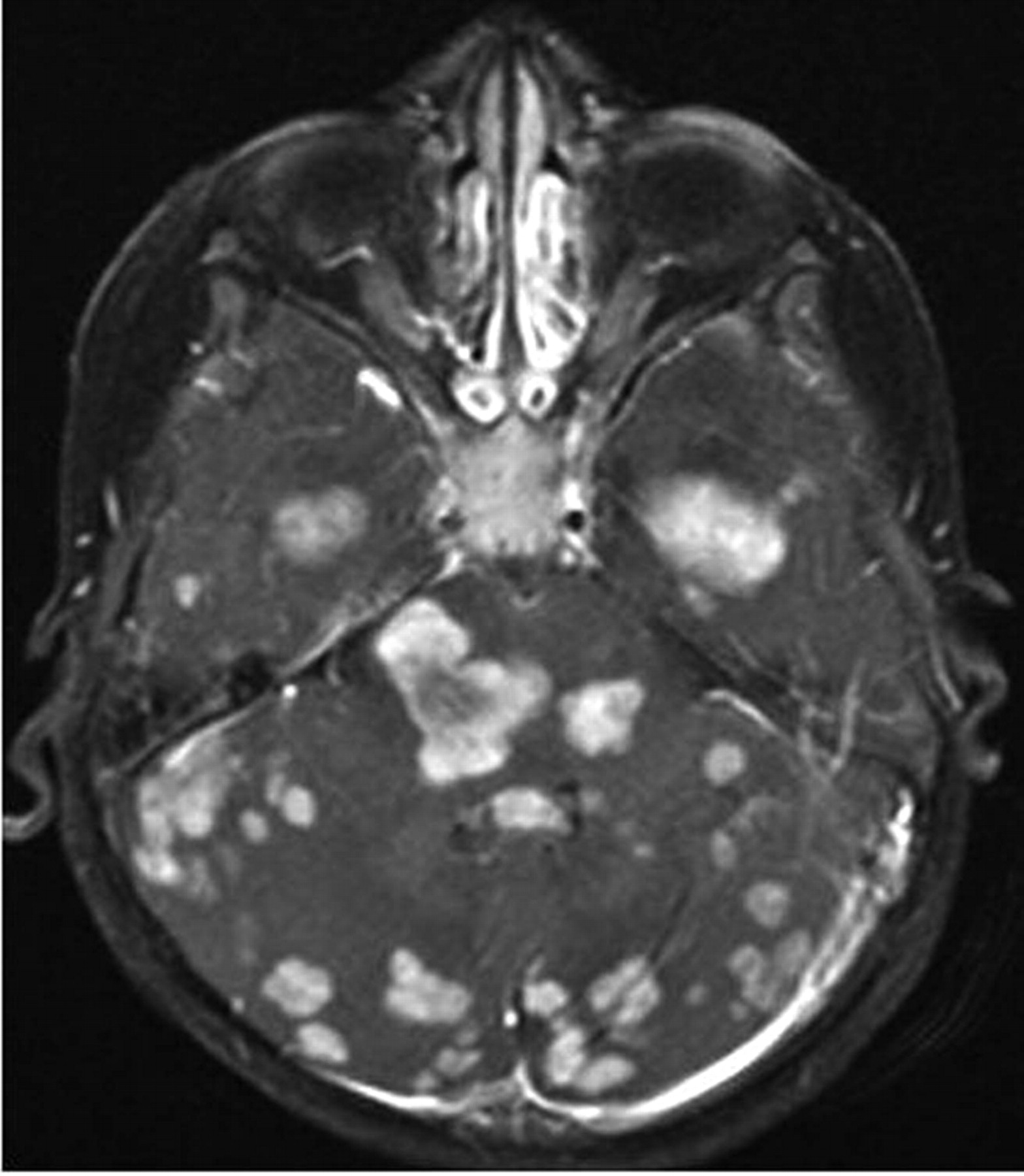
Axial contrast-enhanced T1-weighted image showing multiple enhancing cerebellar, brain stem, and parenchymal lesions.

Axial contrast-enhanced T1-weighted image showing enhancing solid lesions in both hippocampi, brain stem, and temporal lobes.

Axial contrast-enhanced T1-weighted image showing enhancing solid lesions in both frontoparietal lobes and the subependymal region.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sagittal contrast-enhanced T1-weighted image showing enhancing solid lesions in the brain stem, cerebellum, and cerebral parenchyma.
Discussion
JXG is disorder of histiocytes, which is classified under histiocytosis syndromes in children. Histiocytosis refers to a group of disorders characterized by abundance of histiocytes (tissue macrophages) within the affected tissues. It is usually diagnosed in children younger than 10 years of age.
The World Health Organization has proposed a classification for histiocytosis syndromes in children, with 3 main classes1: Class I includes Langerhans cell histiocytosis. Class II includes histiocytosis of mononuclear phagocytes other than Langerhans cells, familial and reactive hemophagocytic lymphohistiocytosis, sinus histiocytosis with massive lymphadenopathy, Rosai-Dorfman disease, JXG, and reticulohistiocytoma. Class III includes malignant histiocytic disorders, acute monocytic leukemia, malignant histiocytosis, and true histiocytic lymphoma. According to the Histiocyte Society classification of histiocytosis syndromes, JXG is classified under dendritic cell−related disorders.1
JXG is a disorder that commonly affects the skin. Other organs like the liver, spleen, kidneys, lungs, and musculoskeletal system can also be involved. Intracranial involvement is uncommon and has been reported previously.2,3 Solitary intracranial lesions are more commonly seen than multiple lesions. However, such an extensive dural and parenchymal involvement as seen in our case is extremely uncommon. Intracranial JXG is usually seen secondary to skin or other organ involvement that has been there for a considerable time.2 The lesions may arise from mesenchymal stem cells, dura, blood vessel walls, or from the perivascular soft tissues. Intracranial lesions may be seen in the cerebral parenchyma, meninges, choroid plexus, or cranial nerves. Clinically, the affected children may be asymptomatic or may present with seizures, ataxia, weakness, or growth retardation. Intracranial involvement in JXG is associated with increased mortality and morbidity. The intracranial lesions have a tendency to grow slowly and must be followed up.4 Treatment can be surgical or nonsurgical. Isolated symptomatic lesions can undergo surgery. Conservative management with steroid therapy provides symptomatic relief, and radiotherapy has also been tried in multiple lesions.
References
- 1.
- 2.
- 3.
- 4.
- Received May 13, 2010.
- Accepted after revision May 18, 2010.
- Copyright © American Society of Neuroradiology