
Abstract
BACKGROUND AND PURPOSE: Iodine contrast extravasation (ICE) is common in patients with acute ischemic stroke (AIS) after endovascular-thrombectomy (EVT). The aim of our study was to evaluate the incidence of ICE assessed by dual-energy CT (DECT), its determinants, and associations with clinical outcome.
MATERIALS AND METHODS: We retrospectively examined imaging parameters and clinical factors from consecutive patients with AIS treated with EVT who had a DECT 24 hours thereafter, identified at a single academic center. Associations between ICE, clinical, imaging, and procedural parameters, as well as clinical outcome were explored by using univariable and multivariable models.
RESULTS: A total of 197 consecutive patients were included (period 2019–2020), of which 53 (27%) demonstrated ICE that was pure ICE in 30/53 (57%) and mixed with intracranial hemorrhage (ICH) in 23/53 (43%). Low initial-ASPECTS, high per-procedural-contrast volume injected, and high admission-glycemia were independently associated with ICE (respectively, OR = 0.43, 95% CI, 0.16–1.13, P = .047; OR = 1.02, 95% CI, 1.00–1.04, P = .003; OR = 8.92, 95% CI, 0.63–125.77, P = .043). ICE was independently associated with ICH (P = .047), but not with poorer clinical outcome (6-month mRS >2, P = .223). Univariate analysis demonstrated that low ADC, higher ischemic volume, ICA occlusion, mass effect, longer procedure duration, combined thrombectomy technique, higher number of device passes, and lower recanalization rate were associated with ICE (respectively, P = .002; <.001; .002; <.001; .002; 0.011; <0.001; 0.015).
CONCLUSIONS: ICE evaluated with DECT is a relatively frequent finding after EVT, present in almost one-third of patients. Lower admission ASPECTS, higher glycemia, and high contrast volume injected per procedure were associated with ICE. We also found an association between ICE and ICH, confirming blood–brain barrier alteration as a major determinant of ICH.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- BBB
- blood-brain barrier
- DECT
- dual-energy computed tomography
- EVT
- endovascular thrombectomy
- HU
- Hounsfield units
- ICC
- intraclass correlation coefficient
- ICE
- iodine contrast extravasation
- ICH
- intracranial hemorrhage
- IOM
- iodine overlay map
- VNC
- virtual noncontrast
Intracranial hemorrhage (ICH), especially when symptomatic, represents a significant complication in individuals experiencing acute ischemic stroke, being associated with increased mortality and worse functional outcome.1,2 The determinants of symptomatic ICH following endovascular treatment (EVT) have been extensively studied in recent works, but there remain areas of uncertainty.3 Among pathophysiological mechanisms of ICH, a severe disruption of the blood–brain barrier (BBB) has been shown to play a pivotal role, and can be readily identified when intraparenchymal iodine contrast extravasation (ICE) is seen on control imaging. Prior studies have shown that ICE is common following EVT,4⇓-6 and is associated with ICH as well as poor clinical outcome.7⇓-9 These works suggest an interplay between ICE and ICH that may be of direct relevance for our pathophysiological understanding of the determinants of ICH, for patients' postacute antithrombotic regimen adaptation and possibly to better inform clinical prognosis following EVT. On follow-up imaging though, increased intraparenchymal attenuation may indicate ICE and/or ICH, making them typically indistinguishable by using single-energy CT. Conversely, dual-energy CT (DECT) has high discriminative capacities for blood and iodine contrast,10⇓⇓⇓⇓⇓-16 allowing it to differentiate ICE from ICH and evaluate their distinct incidence, determinants, and independent contributions to clinical prognosis.
In a single-institution retrospective, observational study, where DECT is routinely used for 24 h follow-up imaging after EVT, we aimed to evaluate the incidence of ICE, its association with clinical imaging and procedural variables, and its association with any radiologic type of ICH and clinical outcome.
MATERIALS AND METHODS
Study Sample
We retrospectively reviewed data from patients with ischemic stroke who underwent EVT between January 2019 and June 2020 and had a control DECT 24 hours later, at our University Hospital Center, a tertiary care academic center.
Patients with posterior circulation ischemic stroke, single-energy CT control, or without control CT were excluded from this study (Online Supplemental Data). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement standards.17
Ethics Statement
In accordance with French legislation, a commitment to compliance was filed to the French National Commission for Information Technology and Civil Liberties, Health Data Hub before data centralization of both retrospective cohorts, in respect to the General Data Protection Regulation CMR004. Written informed consent was waived, but patients or their proxies were informed that they could oppose the use of their deidentified health-related data for the purpose of research.
Clinical Data
Using electronic health records, we retrospectively collected clinical data for each included patient, encompassing demographics, baseline treatments, past medical history, NIHSS index stroke severity (assessed by admission NIHSS and 24 hour-NIHSS),18 treatment variables, and clinical outcome at 6 months. A good clinical outcome was defined as an mRS score of ≤2 at 6 months.19
Endovascular Treatment Data
The following parameters were recorded: anesthesia technique, time to recanalization, delay between onset or last seen well and groin puncture as well as maximal modified Thrombolysis in Cerebral Infarction score.20 Procedural parameters, including blood pressure during procedure, EVT first intent technique (stent/aspiration/combined technique), number of device passes, and final modified Thrombolysis in Cerebral Infarction score were recorded.
Image Acquisition and Postprocessing
The initial diagnosis of AIS was directly obtained by MR imaging, without preceding CT (1.5T Magnetom Aera or 3T Magnetom Prisma, both Siemens). MRI protocol comprised systematic DWI, FLAIR, susceptibility-weighted imaging, time-of-flight MRA, and optional perfusion, and/or gadolinium-enhanced supra-aortic MRA (Online Supplemental Data).
We collected the following acute imaging parameters: occlusion site (middle cerebral artery and its segment [ie, M1, M2 or M3], internal carotid artery, or other), baseline ASPECTS (manually assessed, taking the whole brain into account),21 and positivity of FLAIR in correspondence with ischemia, semiautomated ischemic volume assessed with Carestream Vue PACS Lesion Management (version 12.2, Carestream-Health). For ischemia volume measurements, the semiautomated process was conducted in 2 steps, relying on the ischemia visible in the DWI b = 1000 mm/s2 sequence (for details, see Online Supplemental Data).
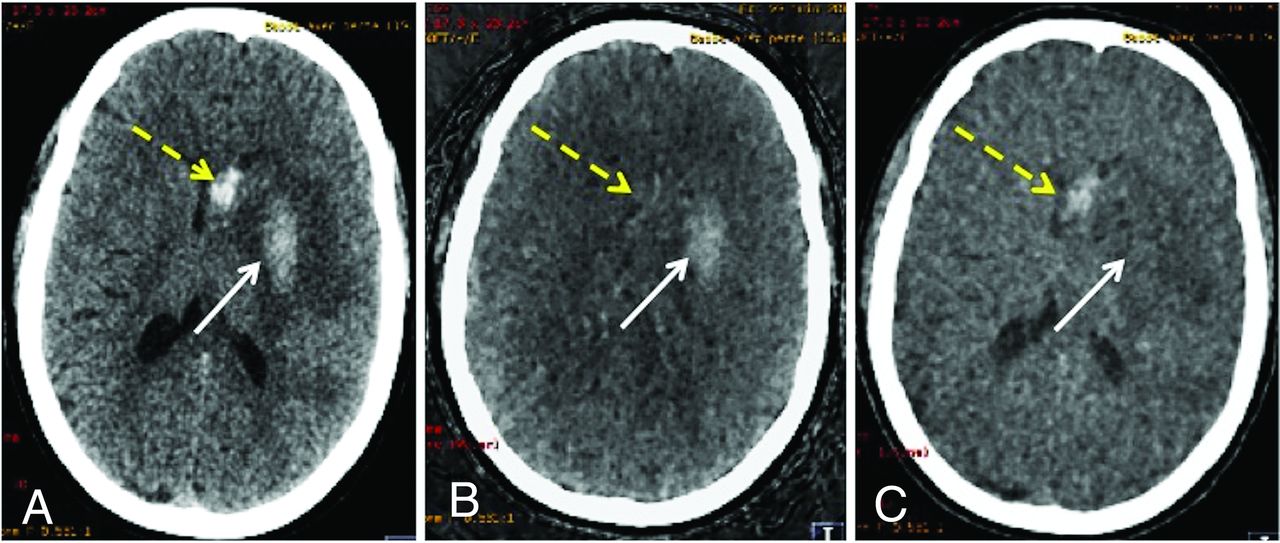
The follow-up at 24–48 h after EVT was obtained with a DECT Discovery-750HD (GE Healthcare), by using the fast kVp-switching technique. The standard practice in our center is to conduct DECT 24 h after endovascular thrombectomy (time of groin puncture), with a potential variation of ±6 h depending on the clinical status and the practical imperatives. DECT acquisition and reconstruction parameters were as follows: caudocranial-scan direction tube A/B: 80/140 kV tube voltage with a 0.25 ms alternance, mAs-reference x/Y, CTDIvol16cm value of 48 mGy × cm, helical beam mono-detector collimation of 20 mm × 0.625, 0.8 second rotation time, pitch = 0.531. The raw spiral data were reconstructed in three different series by a dedicated algorithm, iodine overlay map (IOM) images, virtual noncontrast (VNC) images, and a reconstructed conventional CT by using commercially available software Advantage-ADW-server (GE Healthcare). VNC images were at a 70Ke-V level. Based on the energy-dependent attenuation varying for each material, IOM images map iodine material, whereas blood, which is a substance close to water, is mapped on VNC images. Thus, ICE and ICH diagnoses are made, respectively, on IOM (formal ICE) and VNC (formal ICH) images, with the possibility of association of both (Fig 1).

Association of ICE and ICH diagnosed on DECT performed 24 hours after endovascular thrombectomy. A, Native DECT demonstrating 2 spontaneous hyperattenuations: one in the left capsulo-lenticular region (white arrow, 43 HU), and another in the left caudate nucleus head (yellow doted arrow, 58 HU). B, IOM, confirming ICE in the capsulo-lenticular region (white arrow) and hemorrhagic washout in the caudate nucleus (yellow doted arrow). C, VNC image, at a 70 KeV level, demonstrating ICH in the caudate nucleus head (yellow doted arrow), without contrast extravasation (white arrow). This case also illustrates the impossibility of differentiating ICE from ICH based on HU measurements.
We focused on a radiologic perspective, without distinguishing between symptomatic or asymptomatic ICH, as our research is primarily rooted in the analysis of imaging data related to ICE and ICH.
On follow-up imaging, we assessed the following: presence of mass effect, apparition of an ICH, or/and ICE with confidence index (from 0 to 5). For a more representative depiction of ICE and ICH cases within our population, we formed and analyzed 4 main groups (ICE and no-ICE groups, ICH and no-ICH groups), and 4 subgroups (eg, pure ICE group, ICE+ICH group, pure ICH group and no-ICE, no-ICH group).
Following DECT processing, we collected ICE attenuation value (Hounsfield unit [HU]) and localization as well as ICH attenuation value (HU), localization, and all type of ICH by using the Heidelberg classification22; attenuation values are measurable on the reconstructed conventional images. Hyper attenuation areas were defined as areas with objective higher attenuation than the surrounding brain parenchyma (if doubtful, hyper attenuation of >20 HU compared with adjacent parenchyma). The absence of spontaneous hyper attenuation and formal conclusion for absence of ICE or ICH were recorded.
A double reading by 2 independent radiologists (an experienced neuroradiologist, C.C., 10 years of experience, and a junior radiologist, A.H., 4 years of experience) was performed for a subset of 110 patients' imaging data, a single reading was performed for the 87 remaining imagings (A.H.). All 197 patients' clinical and technical data were collected by a neurologist (C.H.) with 4 years of experience. Disagreement was resolved by consensus.
Statistical Analysis
The data were presented by using different measures depending on the variable type. For continuous variables, medians and interquartile ranges were reported. Categoric variables were expressed as counts and percentages. The normality of distributions was assessed by using histograms and the Shapiro-Wilk test. Interrater reliability was calculated by using the Cohen κ for nominal variables, and intraclass correlation coefficient (ICC) estimates and their 95% CIs for quantitative data. To evaluate the association between recorded variables and ICE, hemorrhagic transformation, and favorable outcome, we conducted univariable analyses by using appropriate tests as per variable types and distribution (categoric variables with Student t test and Mann-Whitney U test and continuous variables with the Pearson χ2 test). For comparison of the 4 subgroups on continuous data, ANOVA or Kruskal-Wallis tests were performed according to data distribution. All variables with a significant association in the univariate analyses (predefined P < .1) were entered into multiple logistic regression models by using backward elimination to analyze potential predictors of ICE, ICH, and favorable outcome. In the model investigating clinical outcome, we forced adjustment for ICE and ICH. OR and their 95% CI were generated for each considered variable. Statistical significance was assessed at a 2-tailed α-level of .05. We calculated standard diagnostic accuracy parameters (ie, sensitivity, specificity, and positive and negative predictive values) for HU associated with ICE and an area under the receiver operating curve was generated. No correction for multiple testing was performed, as this study was inherently exploratory. Statistical analyses were performed by using JMP software, version Pro.14 (SAS Institute, 1989–2021).
RESULTS
We initially screened 350 patients through the prospective department database from January 2019 to June 2020. After application of exclusion criteria (Online Supplemental Data), 197 patients were included in the final analysis: we excluded 153 patients (3 due to missing 24–48 hours CT scan, 11 due to absence of initial imaging available, 123 who had a simple energy CT-control, 15 with a vertebrobasilar occlusion, and 1 patient without clinical information); for comparison between included and excluded population, see Online Supplemental Data.
Eighty-nine (45.4%) patients were women, with a median age of 72 IQR25–IQR75 (61–82) years (Online Supplemental Data). Median delay between EVT (hour of groin puncture) and control DECT was 23 h and 15 min, IQR25–IQR75 (21 h to 25 h 30 min).
On the basis of IOM and VNC images acquired by DECT, 88 (44.7%) patients had spontaneous hyper attenuation on the VNC images. Among them, 53 (26.9%) patients of the total population presented ICE and 58 (29.4%) presented ICH, corresponding in detail to 4 subgroups comprising 30 (15.2%) patients with pure ICE, 35 (17.8%) patients with pure ICH, 23 (11.7%) patients with both ICE and ICH (Fig 1), and 109 (55.3%) patients without ICE or ICH (Online Supplemental Data).
There was a good agreement for HU attenuation for ICE (ICC = 0.89; 95% CI, 0.763–0.946; P < .001); ASPECTS diffusion (ICC = 0.80; 95% CI, 0.726–0.854; P < .001); ICH diagnosis (kappa = 0.778); ICE diagnosis (kappa = 0.772); and moderate agreement for lowest ADC (ICC = 0.66; 95% CI, 0.528–0.761; P < .001).
Predictive Factors for Iodine Contrast Extravasation
Univariate analysis showed that patients who presented ICE had more per-procedural iodine contrast volume injected (200 IQR25–IQR75 [150–300] versus 100 IQR25-IQR75 [100–200], P = .047), higher glycemia at admission (1.38 IQR25–IQR75 [1.20–1.82]g/l versus 1.27 IQR25–IQR75 [1.09–1.48]g/l, P = .016), lower admission ASPECTS (6 IQR25–IQR75 [5–7] versus 7 IQR25–IQR75 [6–8], P = .002), more ICA occlusions than middle cerebral artery occlusions (P = .036), deeper territory ischemia (P = .002), lower minimal ADC (P = .002), and higher ischemic volume (P < .001). For the ICE group, EVT procedure duration was significantly longer (P = .002), the use combined-technique procedures and number of device passes to reach thrombectomy were higher (P = .011 and P < .001), with a lower recanalization rate (P = .015) (Table and Online Supplemental Data).
Details on main parameters for the 4 subgroups are given in Online Supplemental Data, summarizing univariate analysis comparing the pure ICE and ICE+ICH groups. A higher admission NIHSS was associated with pure ICE events compared with the 3 other subgroups (P = .012), and a lower admission ASPECTS was associated with pure ICE compared with ICE+ICH group (P = .002). No other factor was associated with ICE on univariate analysis (Online Supplemental Data).
Low initial ASPECTS, high contrast volume, and high admission glycemia were significantly associated with iodine extravasation in the multivariable analysis (respectively, OR = 0.43, 95% CI, 0.16–1.13, P = .047; OR =1.02, 95% CI, 1.00–1.04, P = .003; OR = 8.92, 95% CI, 0.63–125.77, P = .043) (Table).
Multivariable analysis on ICE
Predictive Factors of ICH
Parameters significantly associated with ICH on the univariate analysis were as follows: ICH group versus no-ICH group: ICE (n = 23 [39.7%] versus 30 [23.6]%, P = .009), ischemia volume (51 ml IQR25–IQR75 [20–83] versus 20 ml IQR25–IQR75 [8–45], P = .012), lower minimal-ADC (405.5 × 10−6 IQR25–IQR75 [346–459] versus 442 × 10−6 IQR25–IQR75 [390–495], P = .006), and more deep territory ischemia (22/55[40.0%] versus 36/125[28.8%], P = .017) (Online Supplemental Data). Detailed information regarding the distribution of ICH types according to the Heidelberg classification and comparison for pure ICH versus ICH+ICE groups can be found in the Online Supplemental Data. It is worth noting that dyslipidemia posed a higher risk for pure ICH versus association of ICH and ICE (P = .007). Furthermore, during EVT, patients with pure ICH received a lower contrast volume injection, underwent fewer device passes, and achieved a higher recanalization compared with those with ICH+ICE (respective P-values of 0.024, 0.046, and 0.048).
Iodine contrast extravasation was independently associated with ICH on multivariable analysis (P = .047) (Online Supplemental Data).
Favorable Outcome
Patients without ICE had a better functional evolution (mRS ≤2) at 6 months than patients with ICE on univariate analysis (70/135 [51.9%] versus 16/49 [32.7%], P = .029). The pure ICE group was also associated with a poorer outcome (P = .041), contrary to the population presenting both ICE and ICH (P = .267) (Online Supplemental Data). Within the ICE population, pure ICE versus ICE+ICH patients did not demonstrate difference for outcome at 3 months (P = .559) (Online Supplemental Data). During EVT, both the global ICE population and the pure ICE group demonstrated a lower recanalization rate (P = .015 and .010, Online Supplemental Data).
ICH was not associated with less favorable outcomes: mRS ≤2 at 6 months for no-ICH-group versus ICH-group (63 [45.3%] versus 23 [39.7%], P = .529), and the pure ICH group did not demonstrate a poorer outcome (P = .849) (Online Supplemental Data).
Among patients without ICE or ICH, 55 (64.0%) achieved an mRS ≤2 at 6 months, while 40 (40.8%) experienced a poor outcome (P = .002).
In the multivariable analysis, 4 parameters were significantly associated with favorable outcome at 6 months (mRS ≤2): lower age (P = .027); higher baseline ASPECTS (P = .015); lower admission glycemia (P = .032); and lower admission NIHSS (P = .004) (Online Supplemental Data). Iodine contrast extravasation was not independently associated with functional outcome (P = .223).
Mean HU Value ICE versus ICH
There was no significant difference in the median attenuation values for the spontaneously hyperattenuated area on the reconstructed conventional images when comparing the ICE and ICH groups, which were previously identified on IOM and VNC maps (P = .349; 48.5 HU IQR25–IQR75 [40.5–64] versus 49HU IQR25–IQR75 [40–56]). This analysis was conducted separately for all locations of ICE (n = 53) and ICH (n = 58), with the understanding that patients with both ICE and ICH were included within each comparison group.
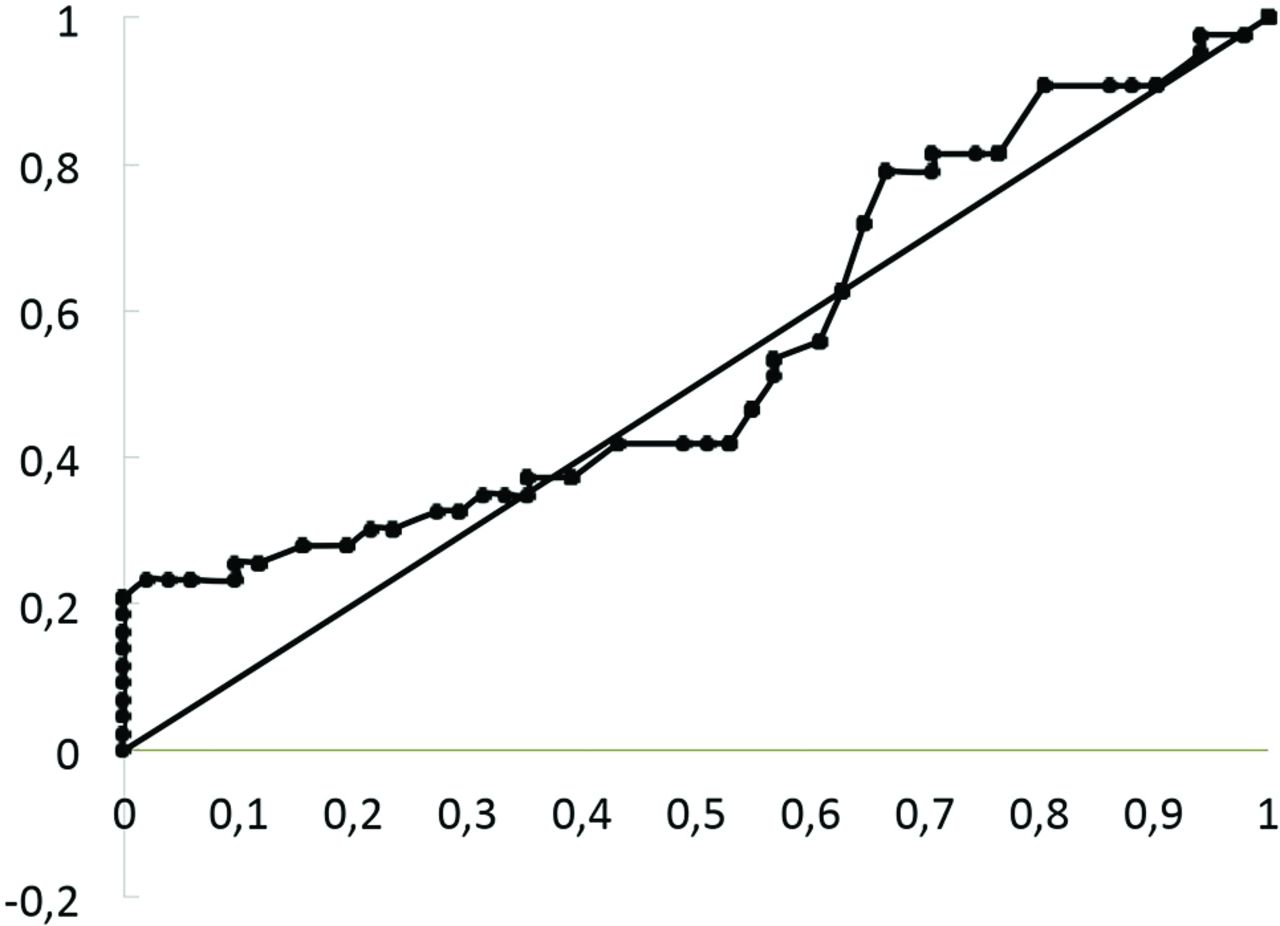
Area under the curve for HU distribution was not discriminative (0.026) (Fig 2). Consequently, we were unable to determine a discriminative threshold in HU sufficient to differentiate between ICE and ICH within the 30–70 HU range, encompassing the majority of our cases. Above 115 HU, all patients had an ICE (n = 9), associated with a 76.5% sensibility and a 18.6% specificity.

Receiver operating curve for mean HU in projection of ICE and ICH groups. Area under the curve = 0.546, illustrating the impossibility of differentiating ICE from ICH based on HU measurements.
DISCUSSION
In this large retrospective cohort of patients treated with endovascular thrombectomy and with a DECT as part of early imaging follow-up, we showed ICE to be frequent, occurring in over one-fourth of our sample, with 15% of patients displaying pure ICE. While ICE was independently associated a higher frequency of ICH, we did not demonstrate an independent association with functional outcome at 3 months, even though the univariate analysis on global ICE and pure ICE groups indicated that extravasation was associated with a poorer outcome.
In this analysis, ICE was diagnosed by DECT, a recognized technique for the early cross-sectional differentiation between ICE and hemorrhage,10,12 providing relevant additional information on the determinants of ICE by comparison with previous works relying on longitudinal simple-energy CT controls,5 and most notably regarding the determinants of ICH and clinical outcome.
In line with previous literature, the incidence of any hyper-attenuating lesions on follow-up CT was high in our cohort, found in 45% of our population after thrombectomy (32%–62% in previous works).7,23 In routine clinical practice, discerning whether these hyper attenuated lesions on control CT are ICE or ICH is important for the adjustment of medical care, and the stratification of hemorrhage risk.
Without DECT, identifying iodine extravasation requires repeated longitudinal control imaging to reveal iodine washout, while hemorrhage transformation persists for days to weeks.24 Previous works proposed various thresholds to help discriminate ICE from ICH on cross-sectional CT, but the commonly used >90 HU cutoff, though sensitive for ICE, lacks sensitivity.24,25 The incidence of ICE on early (12–76 h) CT control widely varies in the literature (14%–81.8%),12,15,26⇓-28 making the challenge not confirmation but rather clear differentiation from ICH.
In our sample, we could not establish a discriminative threshold in HU values to distinguish ICE from ICH, especially in the 30–70 HU range, which corresponds to most of our cases. While it is worth noting that all patients who presented attenuation >115 HU had an ICE, the accuracy for ICH in such attenuation ranges was not changed. The higher the attenuation, the higher the probability of contrast extravasation; while, as suggested by Bonatti et al,7 the higher the hyper attenuation value in early cases, the greater the risk of an ICH.
Quantitative assessment of iodine extravasation based on maximum iodine concentration measurements will possibly require a dedicated software,8 especially if postprocessing of IOM is not upgraded to calculate the iodine concentration from the increased HU values corresponding to ICE.
These data bring contrast extravasation diagnosis closer to the small-scale parenchymal analysis but are not always available on a routine practice.
Most publications on brain DECT applied to patients with AIS are based on the Siemens dual source technique10,11,27,29 or the Philips dual-layer principle.7,14 The fact that we used the fast kVp-switching technique proposed by GE Healthcare's technology, as Almqvist et al15 and Chrzan et al did,30 contributed to broaden the spectrum of data on DECT. Indeed, its use is becoming more widespread, with variations in manufacturers depending on each imaging center.
Importantly, ICH and ICE are not independent, and they have been shown to co-occur in previous works, with ICE being independently linked to ICH. In the work by Chen et al,9 the odds for ICH more than doubled (OR = 2.150) in patients with ICE, and 49% of the ICE population experienced ICH. Similarly, 50% (28/56) of patients with ICE in the cohort of Baik et al8 showed ICH, a very disproportionately higher proportion than unselected cohorts. Their study design differs from ours, as they conducted DECT within 60 min after EVT and followed up with MR imaging within 24 h. Given the higher sensitivity of MR imaging for detecting hemoglobin derivative products,31 it is likely that MR imaging will reveal a higher incidence of moderately extended hemorrhagic transformation, such as HI1 and HI2 according to the Heidelberg classification.
Another work, by Xu et al,5 also showed an association between ICE and ICH. In our sample, a lower initial ASPECTS, a high periprocedural volume of contrast media injection, and a high admission glycemia were independently associated with ICE, which was itself independently associated with ICH. Importantly, all the above-mentioned determinants of ICE are also directly or indirectly linked to the final infarct volume, the most important determinant for the risk of ICH following mechanical thrombectomy in the literature. Our findings plead for a strong interplay between the determinants of ICH and ICE. Whether these factors lead to BBB disruption to varying extents, which may translate as ICE and/or be responsible for ICH remains speculative. In our work, the fact that lower ADC values (a marker of ischemic process severity) were associated with higher risk for ICH, but also for the incidence of ICE, is an additional argument for such an interplay. Hemorrhagic transformation after endovascular treatment implies that the BBB is severely damaged. The disruption of the BBB soon after ischemia paves the way for reperfusion injuries and subsequent ICH. Both MR imaging and CT perfusion studies have aimed to assess disturbances in parenchymal permeability that result in BBB damages after AIS. This was done by analyzing parameters, such as increased time-to-peak or volume transfer constant (Ktrans).32⇓⇓-35
Conversely, iodine extravasation appears to enhance the permeability of the BBB without destroying the basal lamina, allowing the contrast agent to pass between the intravascular and extravascular spaces.32,36⇓-38
Importantly, the association between larger infarct volume (or its determinants) and ICE may explain why previous works have shown a univariable association between ICE and functional outcome, which was present in our work but was not maintained after multivariable adjustment.39
Although we could not perform multivariable analysis for the pure ICE group (due to small sample size), this event was associated with a higher admission NIHSS, lower initial-ASPECTS, longer EVT duration, a higher number of device passes, and a lower recanalization rate compared with the other patients, encompassing mixed ICE+ICH, pure ICH, and cases without ICE or ICH.
The distribution of hemorrhagic transformation types according to the Heidelberg classification exhibited slight differences from recent literature,40 showing a higher incidence of 1c/PH1 and a lower incidence of 1b/HI2. This variance could potentially be attributed to the relatively limited sample size examined.
Our study recommends that the neurologist consider low ASPECTS and high glycemia levels on admission to identify ICE-prone patients. This could prompt earlier CT monitoring, before 12 h post-EVT, as already practiced in some health care centers.8,27
The strong association between per-procedural iodine contrast agent volume and ICE occurrence is expected. Reducing contrast agent volume is an ideal goal, but its feasibility depends on factors such as procedure complexity, patient-specific considerations, and the interventional neuroradiologist's experience. Nevertheless, the concept of minimizing the usage of iodine contrast media in our diagnostic and interventional imaging procedures is gaining traction, driven by economic and environmental concerns.41,42
The study's retrospective, single-center design poses a significant limitation, exposing to intractable inherent selection bias, though we aimed to minimize this bias by using prospectively collected data by using a stroke registry.
Contrast extravasation volume and localization were not detailed; this might be a confusion bias as brain areas have various functional implications. Nikoubashman et al43 found predictive links between initial ischemia and ICE localization, while Song et al44 demonstrated association between ICE volume and clinical outcome, without specifying the localization.
Radiomics development45,46 and computerized tools to differentiate hemorrhage from iodine extravasation may overcome quantitative imaging features and help in discovering new imaging biomarkers.
Collateral circulation's role in ICE and its impact on clinical outcomes warrant attention. We did not distinguish asymptomatic from symptomatic hemorrhagic transformation, which might explain that no association with clinical outcome was demonstrated.
Nonetheless, our study reveals significant ICE associations and novel imaging parameter findings. Neuroradiologists should heed these insights to identify ICE-prone patients, potentially averting hemorrhagic complications.
CONCLUSIONS
ICE evaluated by DECT occurred in 27% of post-EVT patients, with 15% of patients demonstrating pure ICE. Multivariable analysis showed association between ICE with low ASPECTS, high glycemia at admission and high contrast volume injected at the time of endovascular treatment, but not with clinical outcome. We have demonstrated an association between ICE and hemorrhage transformation, an indicator of BBB insult. Identification of patients with high contrast-extravasation and bleeding risks is crucial to improve their clinical management and potential outcome.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- Received December 19, 2022.
- Accepted after revision October 29, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.