
Abstract
Summary: We studied a case of olfactory neuroblastoma by noting 123I-metaiodobenzylguanidine (MIBG) uptake revealed by single-photon emission CT (SPECT). MR imaging revealed an enhancing tumor extending from the left nasal cavity to the bilateral anterior frontal cranial fossae. SPECT revealed high 123I-MIBG uptake in the enhancing tumor. SPECT-revealed 123I-MIBG uptake appears to be clinically useful for distinguishing olfactory neuroblastomas from other tumors, especially suprasellar meningiomas.
An olfactory neuroblastoma is a rare malignant tumor that originates in the olfactory epithelium of the superior nasal cavity. CT scanning typically reveals adjacent bony destruction of adjacent bones, and postcontrast MR imaging has been shown to be helpful in depicting tumor extension and staging of olfactory neuroblastoma. Radiographic findings of olfactory neuroblastoma, however, are usually similar to those of other tumors of the paranasal sinuses, and a definitive tumor diagnosis often is not possible to make on the basis of MR imaging alone (1).
Neuroblastomas belong to a group of neuroendocrinal tumors that are thought to arise from cells in the neural crest. Recently, newly developed radiopharmaceutical agents have had an impact on the diagnosis of neural crest tumors on the basis of specific uptake and storage mechanisms, whereas radionuclide methods for imaging olfactory neuroblastomas have not substantially advanced. Ramsay et al described a case of olfactory neuroblastoma with strong expression of somatostatin receptors, shown by gamma imaging with 111In-octreotide, a somatostatin analog (2). This tracer, however, is not suitable for distinguishing olfactory neuroblastomas from other tumors, especially suprasellar meningiomas, because somatostatin receptor expression has been shown in various brain tumors (eg, meningiomas, gliomas, and pituitary adenomas) (3).
In contrast, the accumulation of metaiodobenzylguanidine (MIBG), a functional analog of the neurotransmitter norepinephrine, has been related to specific uptake and storage mechanisms in neuroblastomas (4). Abnormally high uptake of MIBG has been documented in 73–96 % of patients with extracranial neuroblastoma, and the specificity has been extremely high (5–8). To our knowledge, however, 123I-MIBG uptake in olfactory neuroblastomas is not described in the literature. In the present study, we applied singe-photon emission CT (SPECT) to examine 123I- MIBG uptake in olfactory neuroblastoma to establish a preoperative diagnosis.
Case Report
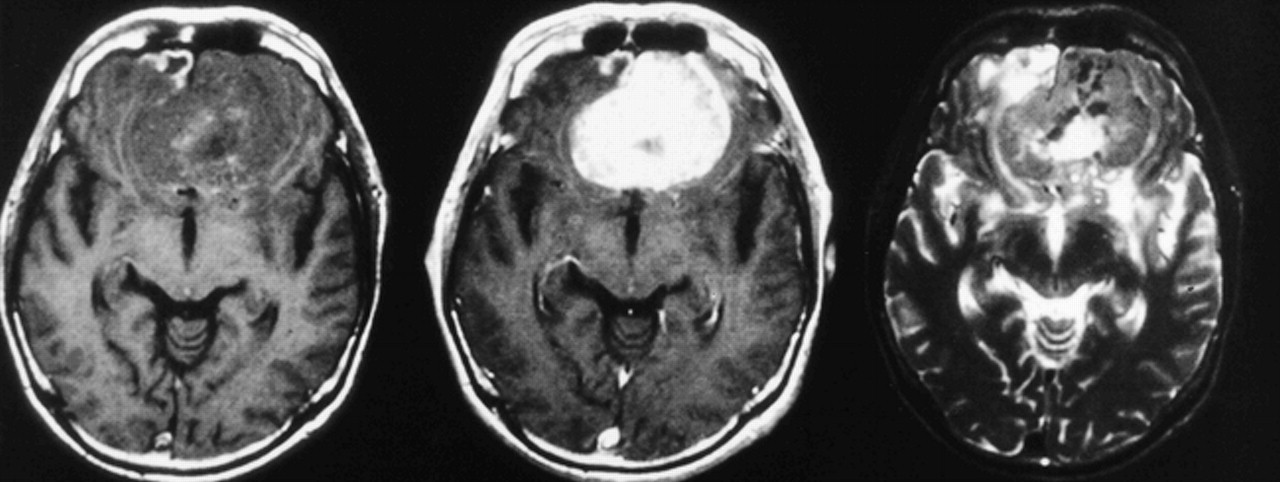
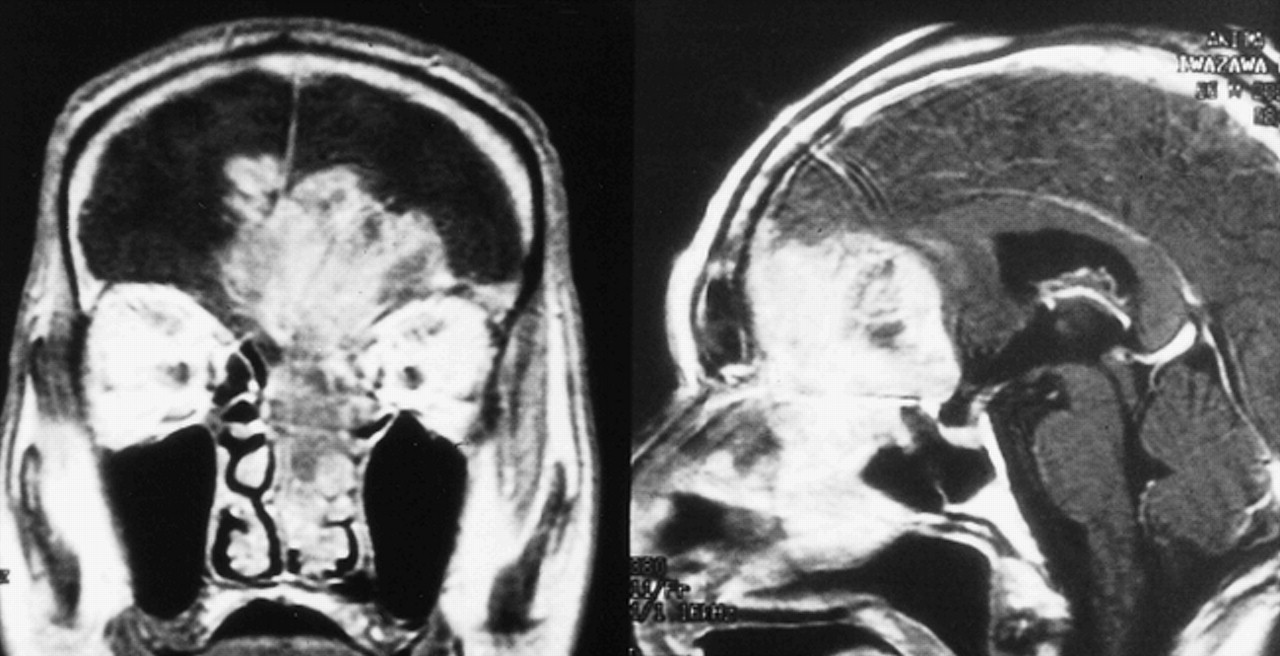
A 66-year-old man presented with a 6-month history of epistaxis. Just before admission to the hospital, he had suffered from bilateral visual disturbance. Neurologic examination disclosed anosmia, papilledema, and decreased bilateral visual acuity. CT scanning revealed a huge enhancing tumor without calcification, extending from the left nasal cavity into the anterior frontal cranial fossae, and destroying the surrounding bone. The tumor was slightly hypointense on T1-weighted MR images (380/13/2 [TR/TE/excitations]), hyperintense on T2-weighted MR images (4800/108/2), and strongly enhanced after administration of contrast medium (Fig 1, 2). Cerebral angiograms revealed a tumor blush fed by bilateral anterior ethmoidal arteries and the left posterior ethmoidal artery.

Axial-plane MR images show expansile bifrontal tumor with dense enhancement (from left to right: T1-weighted image [380/13/2], postcontrast T1-weighted image [380/13/2], and T2-weighted image [4800/108/2])
On the basis of the neuroradiologic findings, olfactory neuroblastoma was suspected as a preoperative diagnosis. Because 123I-MIBG has been shown to accumulate in the neural crest tumors, we examined 123I-MIBG uptake by imaging this patient with SPECT. SPECT images 30 minutes after IV injection of 123I-MIBG at a dose of 111 MBq revealed the accumulation of 123I-MIBG in the tumor. The ratio of tumor (area of highest uptake)/nontumor (T/NT), as an indicator of selective uptake in the tumor, was 2.3. The bilateral temporal lobes were considered representative of nontumor regions (Fig 3).

Coronal (left) and sagittal (right) planes on postcontrast T1-weighted images (380/13/2) reveal an enhancing tumor extending from the left nasal cavity into anterior frontal cranial fossae

Axial-plane 123I-MIBG SPECT image 30 minutes after IV injection of 123I-MIBG at a dose of 111 MBq shows intense uptake in the tumor
Total removal of the tumor was performed successfully through extended bifrontal craniotomy. The histologic diagnosis was neuroblastoma. Fourteen months after postoperative radiotherapy (54 Gy to the tumor bed), the patient has been free of symptoms, showing no evidence of tumor regrowth on follow-up MR images.
Discussion
To our knowledge, this is the first report of 123I-MIBG accumulation in the presence of olfactory neuroblastoma. MIBG was developed as a functional analog of the neurotransmitter norepinephrine. MIBG enters adrenergic cells through a sodium- and energy-dependent uptake mechanism (so-called uptake-one amine transport mechanism) and then resides in and leaves the chromaffin storage vesicles of adrenomedullary tissue (9). The success of MIBG as an imaging agent for neural crest tumors is derived from its chemical similarities to norepinephrine. In neural crest tumor cells, such as pheochromocytomas and paragangliomas, MIBG is specifically taken up by the uptake-one amine transport mechanism at the cell membrane and then transported into and stored within the neurosecretory granules in the cytoplasm. More than 90% of storage occurs in the granules, and a positive relationship between the amount of neurosecretory granules and radioiodinated MIBG uptake has been found. In neuroblastomas, although MIBG is predominantly taken up by the uptake-one amine transport mechanism (10, 11), the lack of a relationship between the amount of neurosecretory granules and radioiodinated MIBG uptake (4), and the finding that up to 60% of storage is extragranular (11), have been documented. Regarding the intracellular localization of MIBG in neuroblastoma cells, most of the 131I-labeled MIBG is found within mitochondria, whereas electron spectroscopic imaging shows fewer are present in specific neurosecretory granules of human neuroblastoma cells (12).
The clinical utility of MIBG as a tracer for detection of neural crest tumors has been well publicized. Abnormally high uptake of MIBG has been documented in 73–96% of patients with extracranial neuroblastoma (5–8), whereas the reported specificity is 93% or more (5–8). In a retrospective study of 100 children with nonsympathomedullary lesions, all had negative MIBG scans except four who had lesions, two of which were diagnosed as neural crest tumors (primitive neuroectodermal tumor and neuroendocrine carcinoma) and two of which were diagnosed as non-neural crest tumors (pancreaticoblastoma and infantile myofibromatosis) (13). The diagnostic value of MIBG scintigraphy in extracranial neuroblastomas is the result of the combination of its high sensitivity and specificity.
In normal distribution, MIBG accumulates in the salivary glands, liver, urinary bladder, gastrointestinal tract, heart, and lung (14, 15). Intracranial MIBG uptake is only occasionally and faintly visible because of the intact blood-brain barrier (BBB), although the brain is richly endowed with adrenergic neurons (16, 17). In this study, 123I-MIBG SPECT was therefore proposed for the detection of intracranial lesions of neural crest tumors, because SPECT has been a common imaging technique for the investigation of brain tumors. SPECT performed after IV injection of 123I-MIBG for detecting olfactory neuroblastomas has not been previously described. In this case, we confirmed the increased accumulation of 123I-MIBG on the early SPECT images in a case of olfactory neuroblastoma. We concurrently examined 123I-MIBG SPECT in four consecutive patients with meningiomas, including one case of planum sphenoidale meningioma. Among four patients with meningiomas, the T/NT ratio on the early SPECT images obtained 30 minutes after tracer administration was 1.33 ± 0.32 (range, 1.1–1.6), which was much lower than that of olfactory neuroblastoma (unpublished data [personal experience in our hospital]). Based on 123I-MIBG SPECT findings, we could preoperatively distinguish olfactory neuroblastomas from suprasellar meningiomas.
Some authors (18, 19) have suggested strategies for the rational use of preoperative radiochemotherapy for this tumor type, which was thought to be inoperable. Goldsweig et al (18) documented that cisplatin-based combinations of chemotherapy in a patient with advanced disease converted a previously inoperable tumor into one that could be resected. At surgery, they confirmed that most of the tumor was necrotic, representing a true response to chemotherapy. This tumor type is sensitive to radiotherapy and several different combinations of chemotherapy, whereas meningioma is less sensitive to radiochemotherapy. Therefore, on the basis of 123I-MIBG SPECT findings, preoperative differential diagnosis of olfactory neuroblastoma from suprasellar meningioma might provide important information for selecting optimal therapeutic strategies for this tumor.
Conclusion
These results support the conclusion that preoperative, accurate diagnosis of olfactory neuroblastoma achieved using 123I-MIBG SPECT may be important for choosing the appropriate strategy in the management of this kind of tumor type.
Footnotes
↵1 Address reprint requests to Toshio Sasajima, M.D., Neurosurgical Service, Akita University School of Medicine, 1–1–1 Hondo, Akita 010–8543 Japan.
References
- Received October 11, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.