
Abstract
BACKGROUND AND PURPOSE: Carcinoma arising in thyroglossal duct remnants is a well-described entity in the pathology and surgery literature, but it has little recognition in the radiology literature. Preoperative diagnosis may alter surgical management, although this diagnosis is rarely made. This study was undertaken to determine the radiologic features that might differentiate carcinoma from benign thyroglossal duct cysts.
METHODS: Twenty-one cases of nonpediatric thyroglossal duct anomalies imaged at our institution during a 15-year period were reviewed retrospectively. The images were assessed for lesion wall thickness, enhancement, soft-tissue component, calcification, and loculation of the cystic component. Three additional cases of thyroglossal duct carcinoma obtained from outside institutions were reviewed for these features also.
RESULTS: Six cases of thyroglossal duct carcinoma were reviewed. All cases of carcinoma had solid soft-tissue elements visible on CT scans or MR images, compared with three of 18 cases of benign thyroglossal duct cysts. The malignant component was seen as a small peripherally based mass in relation to a cyst, a solid mass in the expected course of the thyroglossal duct, or a complex invasive mass also in the midline of the neck. CT only revealed calcification in cases of carcinoma, within either the primary carcinoma mass or a metastatic node.
CONCLUSION: Thyroglossal duct carcinoma should be suspected in an adult patient in the presence of a solid nodule or invasive features in association with a thyroglossal duct lesion visible on CT scans or MR images. The presence of calcification, which is seen best on CT scans, may be a specific marker for carcinoma.
Thyroglossal duct cysts (TDCs) are the most common congenital neck anomaly (1, 2). Carcinoma arising within a TDC or tract has been reported to occur in approximately 0.7% of cases, but is rarely diagnosed preoperatively (3). Its clinical features do not usually distinguish it from a benign TDC (4–6), although malignancy tends to occur in older patients.
Although thyroglossal duct carcinoma (TDCa) is a well-recognized entity, with more than 245 cases reported in the pathology and surgery literature, it has little representation in the radiology literature. We completed this study to review the CT and MR imaging features of TDCa and to determine the radiologic features that might differentiate TDCa from benign TDCs.
Methods
We reviewed all cases of nonpediatric (>18 years of age) thyroglossal duct anomalies that were seen at our institution during the past 15 years and that were imaged by CT or MR. The clinical and pathologic records were retrospectively analyzed. The CT scans and MR images were reviewed, with particular attention paid to lesion wall thickness, lesion wall enhancement, cyst loculation, associated soft-tissue components, calcification, and neck adenopathy. The MR images were also assessed for variability in intensity of the cystic component(s).
Cases of benign TDC were determined based on either pathologic findings at resection or clinical follow-up of at least 1 year. Malignant cases were diagnosed by histopathologic analysis.
We also reviewed three cases of proven TDCa from other teaching institutions, and their images were added to our cases. We reviewed the radiology and general medical literature to identify clinical and pathologic characteristics of TDCa.
Results
Of our 21 cases of thyroglossal duct anomalies that were imaged by CT or MR imaging or both, three were proven pathologically to be papillary carcinoma. The clinical presentation did not help differentiation of TDCa from benign TDCs. Three additional cases of TDCa from outside institutions were reviewed, and their data are also included.
All malignant lesions were pathologically proven to be papillary carcinoma arising in thyroglossal duct remnants. One patient showed papillary carcinoma with a small follicular component. Nine of the 18 cases of benign TDC were pathologically proven, and five of the nine showed chronic inflammatory changes. The remaining nine have not been resected, but clinical follow-up of at least 1 year has shown no significant growth.
In the TDCa group, there were three female and three male patients. The average age of these patients was 40 years (age range, 30–53 years). The average age of the patients with benign TDC was 41 years (age range, 19–65 years; eight male and 10 female patients).
All cases of carcinoma had solid tissue elements evident on CT scans or MR images. Two of the cases of carcinoma did not have a cystic component but appeared to represent thyroid carcinoma arising in thyroglossal duct remnants rather than within a TDC (Fig 1). Two cases showed a small, eccentric, well-defined nodule within a rounded/oval-shaped cyst, whereas a third was a thick-walled, irregularly shaped cyst with an inferior solid component. In these cases, the solid nodules enhanced and showed small foci of calcification. Two of the remaining cases showed more aggressive-appearing lesions with complex features and evident invasion of adjacent tissues (Fig 2).

TDCa in a 36-year-old man with an enlarging, painless right neck mass and a mass at the level of the hyoid bone.
A, Axial contrast-enhanced CT scan shows a 3 × 2.5-cm jugulodigastric node (arrow), which was shown by fine-needle aspiration to be papillary carcinoma.
B, More inferior CT section shows a solid soft-tissue mass at the level of the hyoid bone, slightly to the right of midline (arrow), representing the primary thyroglossal duct tumor. The thyroid gland was normally positioned.
fig 2. A 53-year-old man presented with an enlarging midline neck mass. Axial contrast-enhanced CT scan shows both a cystic component containing a fluid-fluid level (arrowhead) and a large, irregular, invasive solid component (arrow). This was determined to be papillary carcinoma arising in a TDC.
Three of the cases of benign TDC showed solid components (Table 1). Only one of these lesions had a complex cystic/solid appearance on MR images that was thought to be suspicious for malignancy. This appearance was shown to be from thick mucoid material, with the cyst walls showing focal ulceration and inflammation (Fig 3). In the remaining two cases, CT scans showed small, focal areas of thickened cyst wall, but no discrete mass.
CT and MR Imaging features of thyroglossal duct cysts and carcinomas

A 56-year-old man presented with a neck mass that had rapidly enlarged over several months. Malignancy was suspected because of heterogeneity, with solid components seen on MR images and sonograms (not shown). Contrast material was not administered. The lesion proved to be inflammatory changes superimposed on a TDC, with no malignancy found at resection.
A, Sagittal T1-weighted MR image shows a heterogeneous mass of slightly hyperintense signal.
B, Axial T2-weighted image shows hyperintense but heterogeneous signal within this complex lesion.
Four of the six malignant cases showed calcification associated with the solid component on CT scans (Fig 4); one also had calcification in a metastatic right jugulodigastric node. One additional case showed malignant adenopathy without calcification in the node or primary lesion. Calcification was not seen in any of the cases of benign TDC.

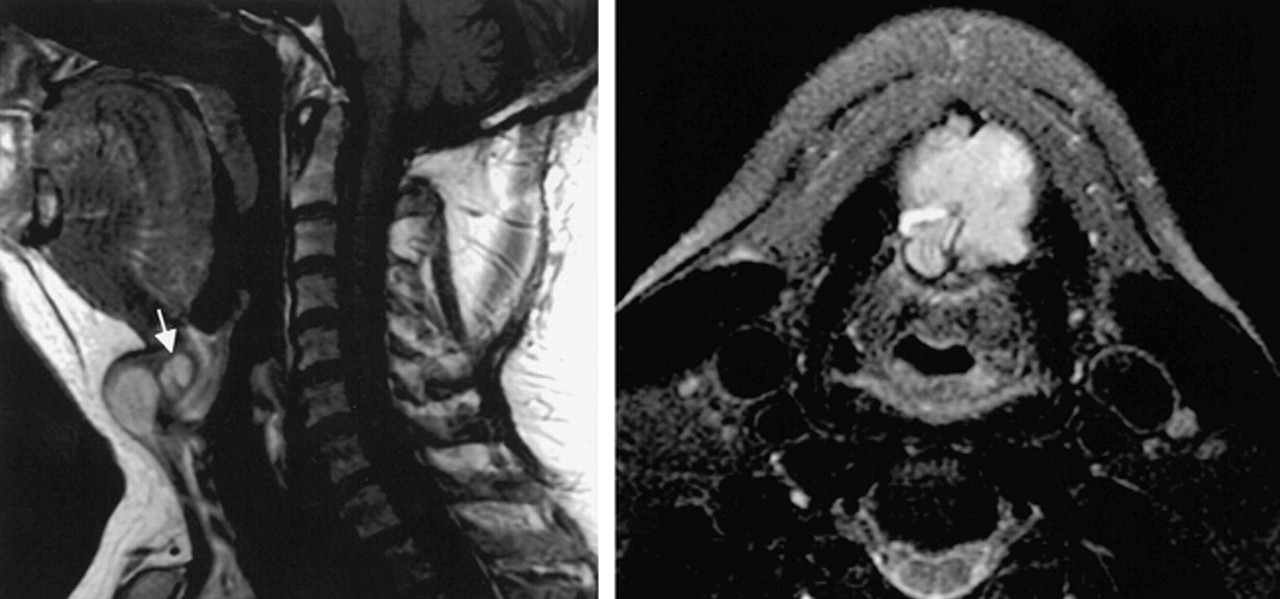
A 47-year-old woman underwent imaging for a newly detected midline neck mass. An unenhanced axial CT scan shows a 2 × 2-cm cystic mass containing an eccentrically positioned solid nodule with an associated focus of calcification (arrow). The nodule enhanced with contrast material, and pathologic analysis confirmed it to be papillary carcinoma.fig 5. A 30-year-old woman presented with an enlarging anterior neck mass that at surgery was found to be a TDC with a nodule of papillary carcinoma. The sagittal T2-weighted MR image shows an infrahyoid multiloculated cystic mass with a solid component superiorly (arrow). The locules were of variable T2 and T1 intensity (not shown)
The only patient who underwent MR imaging showed a biloculated oval-shaped cyst at the level of the hyoid bone with an irregular, solid nodule. The anterior cystic component was hyperintense on both T1- and T2-weighted images, with the posterior cyst appearing hypointense on the T1-weighted images and hyperintense on the T2-weighted images. The solid component appeared heterogeneous in signal, being slightly hypointense to the bright posterior cyst on the T2-weighted images (Fig 5) and hypointense on the T1-weighted images. Contrast material was not used, and the focal calcification revealed on the CT scans was not identifiable on the MR images. Pathologic findings of the cyst fluid were not available. This variability of the MR signal intensity/CT density of the cyst fluid was seen with the benign cases and cases of carcinoma. Multilocular or unilocular cysts were also seen in both groups (Table). Each of our patients was shown to have a thyroid gland in its normal position.
Discussion
The thyroid gland is the first endocrine gland to appear in the embryo. It develops as an evagination of endodermal epithelium in the floor of the pharynx. The thyroglossal duct is formed along the pathway of normal caudal migration of the thyroid, tethering it to the pharyngeal floor. The duct usually fibroses then involutes by 7 to 8 weeks in utero (7, 8).
Persistent remnants of the thyroglossal duct may give rise to cysts at any point along the path of descent, with 61% developing at or below the level of the hyoid bone. These cysts are lined with columnar, cuboidal, or nonkeratinized stratified squamous epithelium. Up to 65% will also have normal thyroid tissue in the wall at sectioning (8). It is from this tissue that most TDCa arise. Thus, 95% of TDCa are thyrogenic, with the vast majority representing papillary carcinomas. This is significant radiologically because the presence of histologic psammoma bodies and calcification in these tumors provides a feature that may be recognizable macroscopically with CT imaging.
Approximately 5% of TDCa are squamous in nature and are characteristically the most aggressive (9, 10). Virtually every type of thyroid carcinoma has been identified arising in TDC, with the exception of medullary carcinoma. This is expected because medullary carcinomas arise from parafollicular cells that develop from the ultimobranchial bodies and not the thyroid anlage (9).
Most TDCs (70%) are diagnosed before the age of 30 years, whereas the average age of development of carcinoma is 39 years. The squamous type of TDCa tends to arise in an older age group, with an average age of incidence at 54 years (10). Carcinoma seems to be more common in the female population, whereas benign cysts have no clear sex predilection. No predisposing factors to malignant change have been identified, although radiation is considered a risk factor (11).
We encountered a significantly higher incidence of carcinoma arising in thyroglossal duct remnants than the reported 0.7%. This is probably largely because of the exclusion of pediatric patients in our study. Additionally, most patients with TDCs do not undergo preoperative imaging unless a suspicious clinical feature is present, such as development of a new midline mass in an adult or the rapid enlargement of a known neck mass.
The standard surgical procedure for the management of thyroglossal duct anomalies is the Sistrunk procedure, which consists of excision of the entire tract of the thyroglossal duct, the midportion of the hyoid bone, and a portion of the base of the tongue. The presence of carcinoma with cyst wall invasion or metastatic spread has been suggested by some to indicate a need for additional thyroidectomy and postoperative irradiation (9). There is an approximately 14% incidence of coincident thyroid gland microscopic papillary carcinoma (12), but a reported low rate of nodal metastatic disease (7.9% compared with orthotopic thyroid papillary carcinoma with 89.8%) (6). The best course of management, however, is still debated. If the managing surgical team advocates thyroidectomy in addition to the Sistrunk procedure, then identification of cases of carcinoma before surgery would allow for a single operation.
The imaging of TDC with sonography, CT, and, more recently, MR imaging has been well described. The most helpful feature of these cystic neck masses in the differential diagnosis is the midline location, most often at or below the hyoid bone, and the relation of the cyst to the strap muscles. The sonography literature has emphasized the variable sonographic findings with an often-complex cystic appearance (13, 14). The CT findings of a TDC have also been well documented as a well-circumscribed, low-density lesion with a thin, smooth rim. Enhancement and thickening of the cyst wall, septations, and increase in the density of the cyst contents suggest additional inflammation or infection (15–17). A wholly solid nodule in the midline of the neck may represent an ectopic or maldescended thyroid, and the lower neck should be checked for an orthotopic gland.
On MR images, a TDC may appear as a simple cyst (low T1 and high T2 signal intensity) but is most frequently of high T1 and T2 signal intensity, consistent with high protein/thyroglobulin content (18, 19). Hemorrhage within a cyst may account for variability of CT density and particularly of MR intensity, although variability was evident with both the benign TDC cases and cases of carcinoma.
There has been little in the radiology literature describing carcinoma in thyroglossal duct remnants. Several case reports have documented these rare lesions (20, 21), and the literature has suggested that the presence of solid components in a TDC should raise the suspicion of malignancy (1, 22). Inflammatory processes, however, may show thickening of the cyst wall and the presence of solid components (15–17) (Fig 3).
Carcinoma was not diagnosed preoperatively in our malignant cases despite the solid component. In one case, the purely solid midline lesion was not recognized on the initial scan but was identified after aspiration of an enlarged node revealed papillary carcinoma. The midline location of the solid nodule and relation to the hyoid suggest its origin from the thyroglossal tract (Fig 1).
By CT, calcification was identified in four of the six cases of carcinoma and none of the benign TDC cases. Calcification was not evident on the MR images in the only case of carcinoma imaged by both techniques.
To our knowledge, calcification has not been reported in association with TDCs, even in the presence of chronic inflammation. Calcification seems to be a specific, although not sensitive, indicator of papillary carcinoma, the most common type of TDCa.
Conclusion
The presence of soft tissue in relation to a TDC suggests the possibility of carcinoma, although inflammatory processes may also show solid components. The presence of calcification may be a specific marker for papillary carcinoma, the most common malignancy to arise in association with a TDC. Calcification and soft-tissue masses are thus important radiologic features to search for when evaluating adults with a clinically suspected TDC.
Acknowledgments
We thank Vincent Chong (Department of Radiology, Singapore General Hospital), James Smirniotopoulos (Uniformed Services University of the Health Sciences, Bethesda), and Nancy Fischbein (Department of Radiology, University of California, San Francisco) for the contribution of data regarding cases of thyroglossal duct carcinoma.
Footnotes
1 Presented in part at the Annual Meeting of the American Society of Neuroradiology, San Diego, CA, May 1999.
↵2 Address reprint requests to Christine Glastonbury, MBBS, FRACR, Department of Radiology, University Hospital, 50 North Medical Drive, Salt Lake City, UT 84132.
References
- Received August 17, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.