
Abstract
BACKGROUND AND PURPOSE: Treatment of ruptured aneurysms with Guglielmi detachable coils (GDCs) has been shown to prevent repeat bleeding. To assess whether GDC coiling alters aneurysmal pressure, we measured intraaneurysmal pressure in two canine types of carotid artery aneurysms before and after GDC placement.
METHODS: A 0.014-inch guidewire with a pressure transducer was inserted into parent arteries and domes of surgically created aneurysms. Intravascular static pressures were recorded before and during saline power injections (10, 20, and 30 mL over 1 and 2 s), before and after GDC placement. Common femoral arterial pressure was monitored.
RESULTS: Saline power injections reproducibly and abruptly increased pressure in parent arteries and aneurysms. Mean intraaneurysmal pressure varied (18 ± 4 [10 mL] to 75 ± 15 mm Hg [30 mL]), independent of injection duration. Intraaneurysmal baseline pressures were higher after GDC placement (111 ± 10 versus 93 ± 15 mm Hg; P = .05). Aneurysmal pressure increases with saline injections were slightly higher after GDC placement, which dampened intraaneurysmal pressure amplitude at baseline (26.5 ± 5.6 versus 19.6 ± 7.4 mm Hg; P = .003) and during hypertension (25.3 ± 5.4 versus 19.8 ± 7.5 mm Hg, P = .002). The pressure increase slope with saline injection was delayed with GDC placement (0.24 ± 0.1 versus 0.38 ± 0.19 s; P < .001).
CONCLUSION: Graded saline power injections into parent arteries can rapidly increase intraaneurysmal pressure. GDC treatment did not attenuate mean intraaneurysmal pressures, but both dampened the pressure amplitude and delayed pressure increases during locally induced hypertension.
The Guglielmi detachable coil (GDC) is a safe and effective alternative to surgical clip placement as a treatment for many types of intracranial aneurysms (1). Successful use of this device in the treatment of ruptured aneurysms causes an immediate and highly significantly reduction in the incidence of repeat bleeding (2). Despite the widespread use of this device, however, its exact mechanism of action has not yet been determined.
Both the genesis and growth of saccular aneurysms directly reflect the influence of hemodynamic forces (3–5). Untreated saccular aneurysms are exposed to the full force of systemic arterial pressure, and, in historical accounts of ruptured aneurysms, an element of transiently increased arterial pressure has often been present.
We hypothesized that the insertion of GDCs into an aneurysm may alter the intraaneurysmal pressure and thereby protects against rupture. By abruptly increasing the arterial pressure in the parent artery of an aneurysm while simultaneously measuring pressure in both the parent artery and the aneurysm, assessment of the propagation of pressure waves into the aneurysm is possible. If the protective effect of GDCs against repeated aneurysmal bleeding is from a mechanical embankment (breakwater effect) of these pressure waves, the response in intraaneurysmal pressure to a defined pressure change in the parent artery should be distinct and differ before and after treatment of the aneurysm with GDC placement.
Methods
With an institutional animal-use protocol, lateral and bifurcation aneurysms were created in five mongrel dogs by using a technique originally described by German and Black (6) and later modified by Graves et al (7). At least 3 wk were allowed between aneurysm creation and treatment.
Endotracheal halothane anesthesia was used in all instances. Vascular access was obtained by using sterile technique through 6F sheaths placed by cutdowns into both common femoral arteries. Systemic arterial pressure was continuously monitored in one of the common femoral arteries. Through the other, a 6F guide catheter was positioned in the common carotid artery proximal to each aneurysm. Fluoroscopy and digital subtraction angiography (DSA) were performed by using a portable C arm. Arterial pressure was monitored and recorded throughout each experiment by using Run-Time LabVIEW 5.1 Software (National Instruments Corporation, Austin, TX). Mean systemic blood pressure was calculated as the systemic diastolic blood pressure plus one third of the difference between the systolic and diastolic pressures.
After placement of the guide catheter into the parent artery of each aneurysm, a 0.014-inch guidewire-mounted pressure sensor (PressureWire Sensor; RADI Medical Systems, Uppsala, Sweden) was calibrated to 0 at room barometric pressure. It was positioned in the parent artery such that the transducer was located 2–4 cm proximal to the aneurysm, thereby avoiding any obstruction or flow disturbance in or adjacent to the aneurysm (Fig 1). By using a commercially available angiographic injector (Angiomat 3000; Liebel-Flarsheim, Cincinnati, OH), we abruptly increased the intraarterial pressure by injecting, in sequence, 10, 20, and 30 mL of normal saline over 1 and 2 s (locally induced hypertension). Pressures were monitored and recorded in the parent artery under baseline conditions as well as during each saline injection. The pressure wire was then repositioned so that the pressure sensor was in the dome of each aneurysm. Exact positioning of the pressure sensor and maintenance of the specific placement was accomplished by visualization of the radiopaque marker of the sensor on a DSA roadmap. After baseline measurements of pressure, the series of saline injections was repeated, and pressures were monitored and recorded.

DSA image shows a bifurcation and a lateral aneurysm. The pressure wire is in place in the dome of the bifurcation aneurysm. The pressure sensor is at the junction of the radiopaque and nonradiopaque portion of the wire (arrow). A dime is taped to the neck of the animal
With the pressure wire in place in the aneurysmal dome, a two-marker, Tracker Catheter (Boston Scientific Corporation–Target Therapeutics, Fremont, CA) then was introduced into each aneurysm and GDCs were positioned and detached with standard clinical techniques. In all instances, the distal aneurysm (lateral) was treated before treatment of the proximal (bifurcation) aneurysm. Intraaneurysmal pressures were monitored during the coiling procedure. All aneurysms were treated by using clinical criteria so that packing was continued until either no more coils could be introduced or there was judged to be risk of compromise of the parent artery. When coil placement was completed, the saline power injections into the parent artery were repeated in a manner identical to that previously described. After completion of these measurements, all animals were euthanized (Beuthanasia-D Special; Schering Animal Health, Kenilworth, NJ).
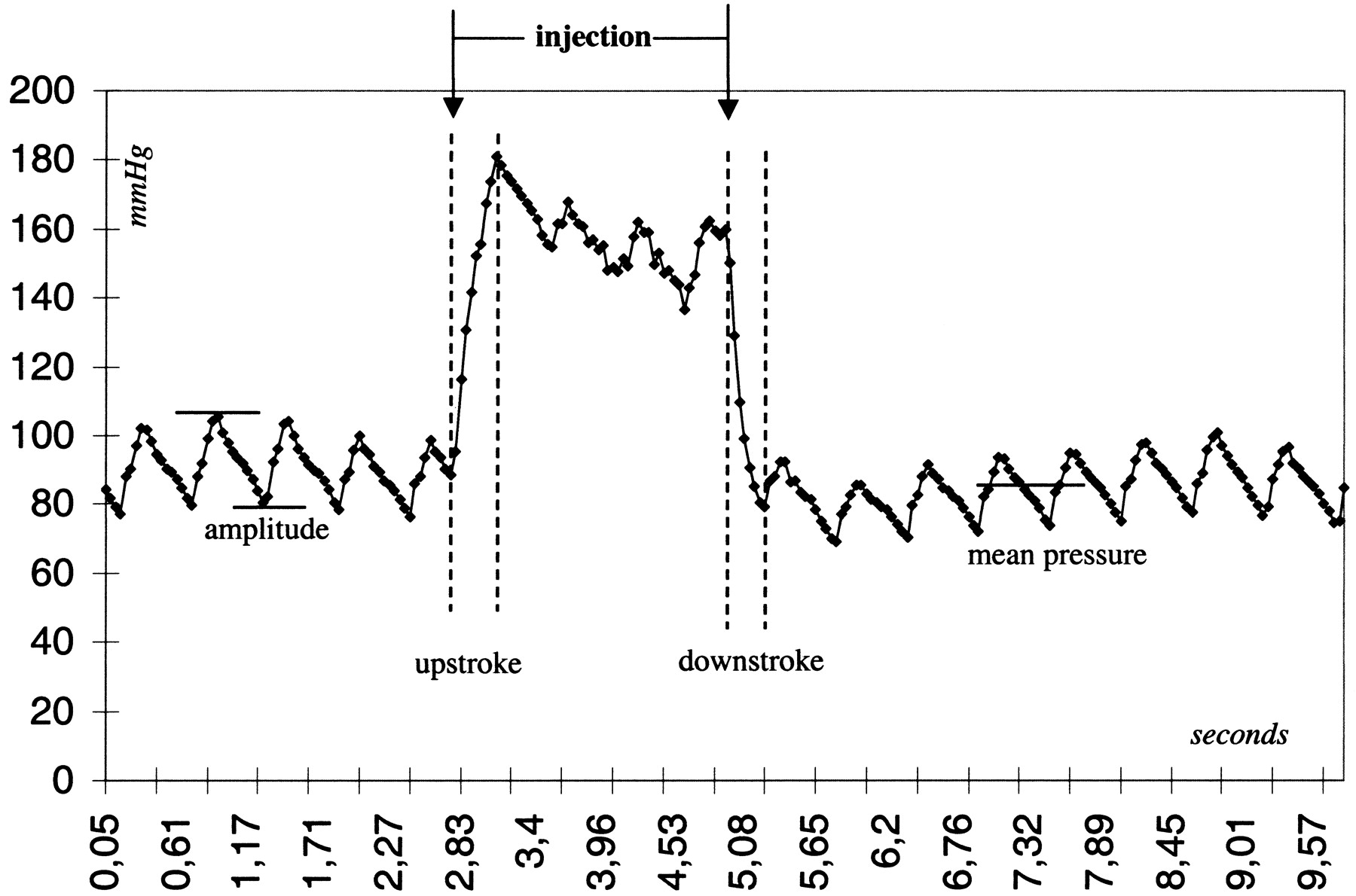
The mean pressures at baseline and during the saline injections, the pressure amplitudes (systolic pressure minus diastolic pressure), and the upstroke and downstroke of pressure changes were analyzed both before and after GDC placement. The upstroke was defined as the interval between the start of saline injection and the maximum pressure increase after saline injection. The downstroke denotes the time from the end of the induced hypertensive interval to a return to baseline pressure values (Fig 2).

Pressure trace in the dome of a lateral aneurysm during injection of 30 mL/s saline over 2 s. The pressure amplitude, mean pressure, upstroke, and downstroke of the saline injection are indicated
Results
In all instances, the pressure guidewire allowed stable pressure measurements to be recorded under baseline conditions and during power injections of saline and during GDC placement. Differences were noted between the measurements obtained in the lateral and bifurcation aneurysms, during baseline conditions, induced hypertension, or during or after GDC placement. No spasm was induced in the parent artery with manipulation of the pressure guidewire or with the saline injections.
Induced Hypertension
Graded power injections of normal saline into the parent arteries of these aneurysms created reproducible, abrupt increases in arterial pressure in both the parent artery and the aneurysm. The magnitude of the pressure increases depended upon the volume of the saline injection. Table 1 lists the increases in pressure obtained by saline injections at a given volume (the values represent an average from multiple injections of a specific volume). The duration of the injection did not correlate with the magnitude of the pressure increase (Table 1, Fig 3). Systemic blood pressure was unaffected by the saline power injections.
Increases in intraaneurysmal pressure with saline power injections in the parent artery

Pressures observed during injections of 10, 20, and 30 mL saline over 1 or 2 s. The volume, not the duration of injection, correlated with the magnitude of the pressure increases
Pressures in the Parent Artery Versus Dome of the Aneurysm before Treatment
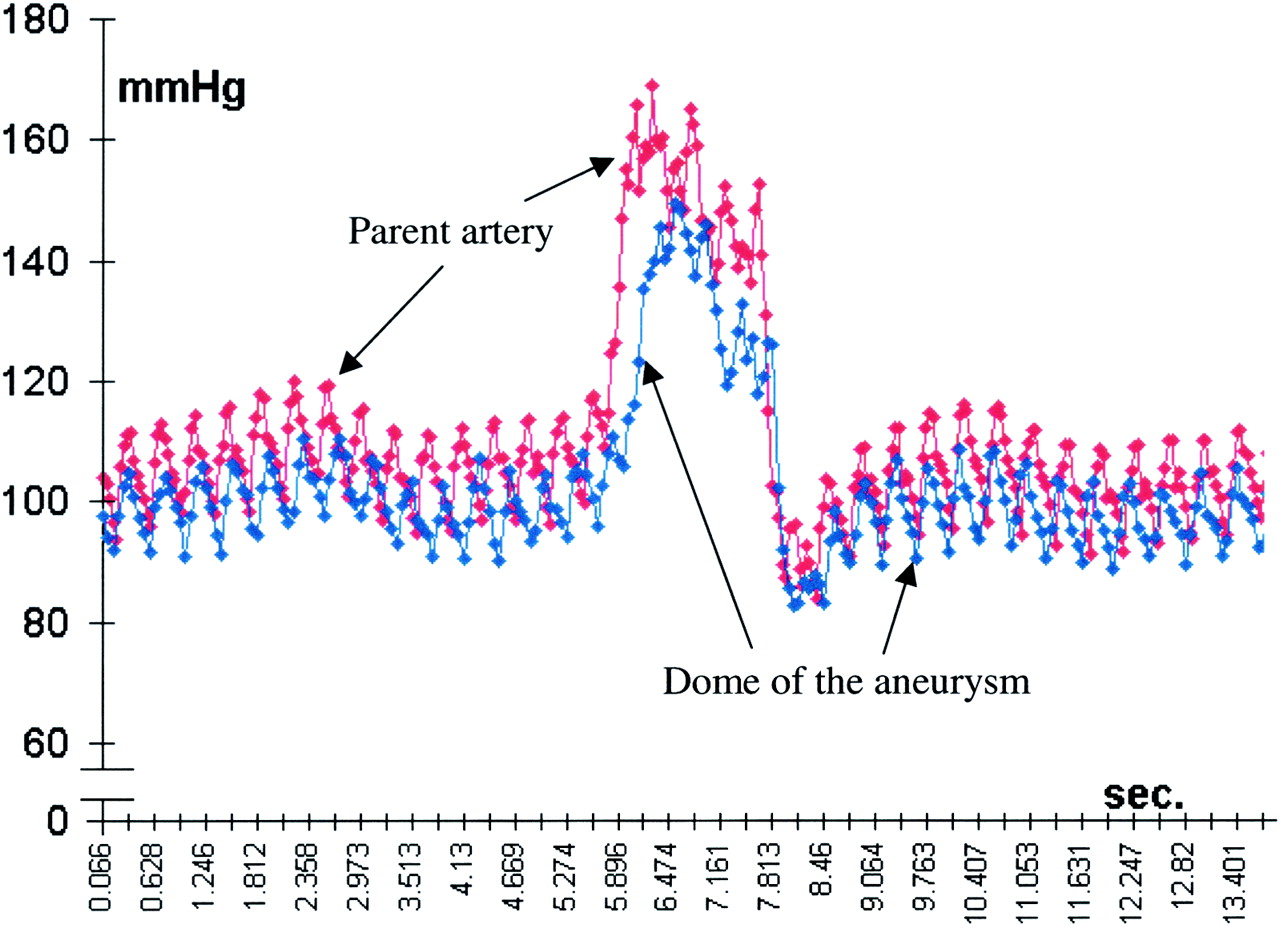
Mean pressures and pressure amplitudes in the parent arteries and in the dome of the aneurysms were similar during baseline measurement (Table 2, Fig 4). Mean pressure increases created by the saline injections were slightly greater in the parent arteries than in the aneurysmal domes; the amplitudes during saline injections were similar. The upstrokes and downstrokes of induced hypertension were comparable in the domes of the aneurysms and in the parent arteries.
Pressures in the parent artery and dome of aneurysm

Pressures in the parent artery versus the dome of the aneurysm during the injection of saline at 20 mL/s
Pressure in the Dome of the Aneurysm before and after GDC Placement
On average, GDC placement did not significantly affect the baseline pressure in the dome of the aneurysm (Table 3). The abrupt increases in intra-aneurysmal pressure that followed a power injection of saline were, however, slightly higher after completion of GDC placement (Table 3, Fig 5). Pressure amplitudes both at baseline and during induced hypertension were diminished after completion of GDC treatment (Table 3). Moreover, the upstroke of the pressure increase after power injection of saline was significantly decelerated in the coiled aneurysms (Table 3, Fig 6). The downstroke after power injection of saline was unaffected by the presence of the GDCs.
Intraaneurysmal pressures at baseline and during saline injections

Pressures in the dome of an aneurysm during injections of 10, 20, and 30 mL of saline over 2 s before and after complete coil placement. The mean pressure was unaffected by coil placement, whereas the pressure amplitude was attenuated

Pressure trace from the dome of an aneurysm before GDC coiling (top) and after complete GDC placement (bottom) during injections of 10 mL of saline over 2 s. Neither baseline pressure nor the induced pressure increase was reduced after coiling. The upstroke of the pressure increase decelerates after saline injection (dotted lines)
Discussion
Although the exact mechanisms and interactions responsible for growth and rupture of saccular aneurysms remain controversial, it is evident that they are closely related to what may generally be termed hemodynamic stress (pressure, shear stress, impulse) (5–7). Both in experimental and in human aneurysms, intraaneurysmal pressure has been shown to mimic systemic arterial pressure (8, 9). Thus, untreated saccular aneurysms are exposed to the full force of systemic arterial pressure. Aneurysms often rupture in situations known to be associated with transiently increased arterial pressure and heart rate (8, 10). Because of this clinical observation (and a poor understanding of the dynamics of shear stress and impulse), aneurysm rupture is often ascribed to the effect of pressure. This concept is supported by data indicating that the most frequent location of aneurysm rupture, the dome, is remote from the location of maximum shear stress and impulse—the downstream extent of the ostium (11). Hemodynamic stress also is known to induce responses that can cause tissue to reinforce itself. In this regard, the wall of an aneurysm often is thickest at sites with relatively high stress, that is, the ostium and neck (12). The dome and center of the aneurysm, on the other hand, are relatively silent zones hemodynamically, with low stress (12). Therefore, the wall of the aneurysm often is extremely thin at the dome, representing the weakest point along its wall, and thus, the most likely site of rupture.
Endovascular treatment of saccular aneurysms with GDCs is presumed to offer a protective effect against aneurysm rupture or rerupture because of relief or modification of hemodynamic stresses (9, 13, 14). The primary finding from our study is the observation that complete coil treatment in both lateral and bifurcation aneurysms with GDCs did not reduce mean pressure either at baseline or during abrupt and substantial pressure increases (as high as 300 mm Hg). We also recorded a significant reduction in the pressure amplitude under both conditions. Finally, the slope of the induced, abrupt increases in pressure (upstroke) was significantly delayed.
Both Boecher-Schwartz and colleagues (14), using an in vitro model of explanted aneurysms densely packed with coils, and Novak and associates (9), using a canine model of aneurysms treated with only a single coil, have reported that coiling neither eliminates nor modifies intraaneurysmal pressure under normotensive conditions. Both groups measured pressure by means of a cannula inserted through the aneurysmal wall. Although insertion of either a single coil (Novak) or multiple coils (Boecher-Schwarz) in these experiments did not measurably change the mean intraaneurysmal pressure, the interventions did reduce the aneurysmal wall pulsations and modify the aneurysmal hysteresis curve. These studies, because of the methods used to record pressures, necessarily operated with an artificial discontinuity in the aneurysmal wall. Our intravascular, “noninvasive” method of pressure measurement would appear to be more physiologic, which may be why we were able to delineate a dampening of the pressure amplitude after insertion of coils. The observation of reduced pulsation of the aneurysmal wall after coiling is difficult to understand if coiling truly does not alter the pressure amplitude. Our observation of attenuation of the pressure amplitude and a moderation of pressure per unit time (slower upstroke) after a sudden surge in pressure suggests that while the GDC coils do not alter the magnitude of the pressure, they do, by providing a “breakwater” effect, serve to relieve stress on the aneurysmal wall. This effect may be powerful enough to provide an immediate protection against repeat bleeding after successful coiling. It remains uncertain, however, whether this breakwater effect alone provides sufficient long-term protection. According to Austin et al (5), high-pressure amplitudes favor aneurysm growth at a lower pressure threshold. In other words, reduced pressure amplitudes will shift the curve of aneurysmal growth—and, finally, rupture—to a higher pressure threshold.
Our findings confirm, in an in vivo model that eliminates the need to disturb the integrity of an aneurysmal wall, observations of similar baseline pressures in the parent artery and aneurysm. Through the use of graded power injections of saline, we were able to create extremely swift and high pressure increases. During these, the measured increases were proportionally lower in the aneurysmal domes compared with those in the parent arteries. Our explanation for this difference is that because of the very brief duration of induced high pressure (1 or 2 s), the maximum pressure present in the parent artery could not be fully transmitted into the aneurysms (forward flow into an aneurysm occurs only during systole). At a longer interval of high pressure, the pressures in the parent artery and in the dome of the aneurysm would be assumed to equalize. Except for their duration, we believe that the very swift pressure increases induced by our technique resembled those that occur during situations known to provoke rupture of cerebral aneurysms more than the pressure increases induced by pharmacologic manipulation. The power injection of saline into the parent artery allows intraaneurysmal pressure to be increased abruptly within one cardiac cycle, thus mimicking genuine blood pressure increases that can occur in patients. This method also allows easy control and the ability to repeat pressure increases to up to 300 mm Hg without systemic adverse effects.
Of possible clinical importance is our observation that the power injection of 10 mL of saline over 1 s into the common carotid artery abruptly increased intraaneurysmal pressure by about 19 mm Hg. We also were able to create pressure increases of up to 40 mm Hg by means of hand injection of 10 mL of saline. Intraaneurysmal pressure increases of this magnitude might pose a risk of causing aneurysm rupture or repeat rupture. This observation, therefore, may have potential affects on the technique used to perform angiography in patients with suspected aneurysmal subarachnoid hemorrhage. This has been stressed by Sorimachi et al (15), who investigated intraaneurysmal pressure changes during angiography in coil embolization.
In our model, under baseline conditions, complete coiling of the aneurysms did not cause any change in the mean intraaneurysmal pressure. This observation corresponds to those made using other models (9, 14). Under conditions of rapid and transient induced hypertension, however, we measured slightly higher increases in pressure in the aneurysmal domes after coil placement. The reason for this is unclear, but it may relate to changes in the arterial input impedance (the ratio of pressure to flow), a function that depends both on reflected and forward traveling waves (16). Because of their low compliance, coils will exert a high reflection coefficient, and thus, could increase arterial input impedance.
Although our results indicate that treatment with GDCs does alter intraaneurysmal pressure, which may be responsible for the protective effects of this device, other benefits may be provided as well. Although, to our knowledge, the benefit has not been quantified, even incomplete treatment of aneurysms with GDCs can dramatically alter the flow pattern within an aneurysm. Because such a change markedly decreases flow velocity, shear stress may be substantially decreased. Also, by increasing what might be considered the surface area of the aneurysmal wall, coils may substantially reduce the hemodynamic stress resulting from impulse, a variable that increases in magnitude when directed at a small area over a short interval. The effect of GDCs on these variables (flow and impulse) is the subject of ongoing experiments in our laboratory.
Conclusions
The intravascular pressure guidewire used in these experiments allows reliable and stable measurement of parent artery and intraaneurysmal pressures. By using power injections of saline into the parent artery, intraaneurysmal pressures can be abruptly increased to as much as 300 mm Hg without systemic adverse effects. The intraaneurysmal mean pressures both under baseline conditions and during induced pressure increases tended to be higher after GDC introduction. On the other hand, the pressure amplitudes, both at baseline and during abrupt increases, and the slope of the pressure increase were significantly attenuated by GDC placement.
Footnotes
1 Funded in part by Boston Scientific Corporation/Target Therapeutics, Fremont, California. Dr Strother is a member of the Scientific Advisory Board of Boston Scientific Corporation/Target Therapeutics.
2 Address reprint requests to Charles M. Strother, MD, University of Wisconsin, Department of Radiology, E1/320 CSC, 600 North Highland Avenue, Madison, WI 53792-3252.
References
- Received February 7, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.