
Abstract
BACKGROUND AND PURPOSE: Since 1996, several preliminary studies have shown the usefulness of contrast material–enhanced MR angiography for imaging supraaortic vessels. The aim of this study was to compare the accuracy of contrast-enhanced 3D MR angiography with that of digital subtraction angiography (DSA) in the evaluation of carotid artery stenosis.
METHODS: A blinded comparison of first-pass contrast-enhanced MR angiography with conventional DSA was performed in 120 patients (240 arteries). MR angiography was performed with a 1.5-T magnet with gradient overdrive equipment, by using a coronal radiofrequency-spoiled 3D fast low-angle–shot sequence after the intravenous injection of gadodiamide. The guidelines of the North American Symptomatic Carotid Endarterectomy Trial for measuring stenosis of the internal carotid artery were applied on maximum intensity projection (MIP) images and conventional catheter angiograms.
RESULTS: Grading of stenoses on MR angiograms agreed with grading of stenoses on DSA images in 89% of arteries. In the severe stenosis group (70–99%), agreement was 93%. All internal carotid occlusions (n = 28) and seven of nine pseudo-occlusions were accurately detected with contrast-enhanced MR angiography. The correlation between MR angiography and DSA for determination of minimal, moderate, and severe stenoses and occlusion was statistically significant (r = 0.91, P< .001).
CONCLUSIONS: This investigation with a large number of patients confirms that contrast-enhanced MR angiography could become a diagnostic alternative to DSA in the treatment of patients with carotid artery disease.
Several randomized controlled clinical trials, such as the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the European Carotid Surgery Trial proved the benefit of endarterectomy in patients with symptomatic, severe (≥70%) carotid stenosis (1–4). The indication for carotid endarterectomy has been extended also to patients with asymptomatic carotid artery stenosis (≥60%), as presented in the Asymptomatic Carotid Atherosclerosis Study (ACAS) (5). Final NASCET results demonstrated a surgical benefit for selected patients with stenosis as low as 50% (6). These studies gave rise to discussion and kindled the interest in and necessity for accurate measurements of carotid stenosis. In these studies, digital subtraction angiography (DSA) was the accepted criterion standard to determine the degree of carotid stenosis with respect to surgical intervention.
Since 1996, several preliminary studies have shown the usefulness of contrast material–enhanced MR angiography for imaging supraaortic vessels (7–38). Developments in hardware and software have overcome initial limitations and resulted in high-quality images of the carotid arteries comparable to those with DSA. Different strategies for sampling k space can be used for acquisition of 3D MR angiographic sequences according to the clinical application. The most conventional protocols include a large imaging volume, a spatial resolution adequate for carotid assessment, and an acquisition time of approximately 30 seconds. Other sequences improve the spatial resolution of the images by using a 512 × 512 matrix with submillimetric voxels. Another strategy is to improve the temporal resolution by using an acquisition time of 5–10 seconds, to obviate bolus timing and provide some hemodynamic data.
The aim of this study was to compare an ultrafast time-resolved contrast-enhanced MR angiorgaphic technique with DSA for use in detecting stenosis at the carotid bifurcation.
Methods
Patients
We examined 120 consecutive patients (30 female and 90 male patients; mean age, 65 years ± 12 (SD); age range, 9–88 years) who underwent contrast-enhanced MR angiography and DSA over a period of 30 months. The patients were examined at our institution for suspected extracranial carotid artery disease based on clinical and color-coded duplex sonographic findings. The MR imaging protocol included intracranial conventional spin-echo T1-weighted and fast spin-echo T2-weighted sequences, as well as diffusion-weigthed imaging. DSA and contrast-enhanced MR angiography were performed within a maximum of 2 weeks of each other. A total of 240 carotid bifurcations were evaluated in this study.
MR Angiographic Technique
All MR angiorgaphic investigations were performed with a 1.5-T imaging system (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany) equipped with a gradient overdrive. The maximum achievable gradient amplitude was 25 mT/m, and the slew rate was 180 T/m/s.
Spoiled 3D fast low-angle–shot contrast-enhanced MR angiography was performed by using a 4 × 2 circularly polarized phased-array neck coil. The sequence was performed with 32–36 coronal partitions each 1.67–1.94 mm thick, 2.84–3.15/1.03–1.11/1 (TR/TE/NEX), 35–40° flip angle, 70–60 × 140 × 280-mm3 field of view by a 36 × 92 × 256 image matrix, and an imaging time of 9–9.5 seconds. Reconstruction was performed without zero filling. The pixel size was 1.5 × 1.0. The spatial resolution or voxel size was 1.8 × 1.4 × 1.0. The k space was filled in sequential order. Four consecutive 3D images were obtained, starting at approximately 3 seconds after the start of the bolus injection of 0.1 mmol/kg gadodiamide (Omniscan; Nycomed, Oslo, Norway). In our experience, this contrast dose is enough to provide adequate diagnostic image quality with a time-resolved contrast-enhanced MR angiographic technique. Considering the variability in patient size and weight, as well as cardiac output and hydration, we believe that only occasionally could a diagnostically significant higher image quality be attained with a higher dose of contrast material. Because of the rapid acquisition time, we believe that use of other timing strategies such as a test dose or a triggered acquisition would not noticeably improve image quality. In non–time-resolved contrast-enhanced MR angiography, timing strategies have a more important role. No breath holding was used in the current study. All injections were performed by hand (a power injector was not available) by means of a 150-cm-long catheter into an antecubital vein. Each bolus was followed immediately by a 15-mL saline flush, by using a three-way stop-cock to facilitate a smooth transition between contrast material and saline injections. Maximum duration of the total injection was 10 seconds.
The 3D image set acquired during the arterial phase of the bolus passage was identified by means of visual inspection, and that data set was subsequently subtracted from the precontrast (usually the first) data set, after the disturbing background signal intensity of fat was eliminated. Postprocessing subvolumes were generated interactively by using the MR postprocessing console to isolate each carotid artery and create 19 maximum intensity projection (MIP) images at 10° increments each. Voxels of interest on magnified images were used to facilitate determination of the extent of disease.
The total time for the 3D contrast-enhanced MR angiographic examination was 5–10 minutes, the largest part of which was taken up by handling and positioning the patient. Over the 2½-year period of this study, we did not substantially change the technical parameters of the study protocol.
DSA Technique
Selective cerebral DSA was performed via the femoral artery, starting routinely with imaging of the aortic arch followed by selective injections of contrast material (iopamidol [Iopamiro 300]; Bracco, Milan, Italy) in both common carotid and subclavian arteries and at least one vertebral artery. The injected volume of contrast medium was 5–8 mL. Biplane DSA was performed routinely in the anteroposterior and lateral projections with a 33-cm field of view and a 1024 × 1024 matrix. The spatial resolution was 0.32 × 0.32 mm. If a bifurcation was not adequately visualized, additional DSA was performed in oblique projections.
Stenosis Measurement and Image Analysis
Carotid stenosis was measured on both DSA images and MR angiograms as a percentage of the diameter by using the NASCET criteria (1, 2, 39–45). The image that demonstrated the most severe stenosis was used. The diameter of the most severe stenosis was divided by the diameter of the distal cervical internal carotid artery beyond the stenosis. Carotid stenoses were measured at the same level on the DSA images and contrast-enhanced MR angiograms. The value was subtracted from 1 and then multiplied by 100 to yield the percentage diameter stenosis. The NASCET categories were arbitrarily modified to define a 98% stenosis as the presence of a signal void on MIP images at the level of the stenosis when flow was visible distal to the stenosis (9). Negative values were defined as 0% stenosis. The obstructions were classified as mild stenosis (0–29%), moderate stenosis (30–69%), severe stenosis (70–99%), or occlusion (100%). For each examination, the measurement of the exact degree of stenosis was made at the level of maximum stenosis by using high magnification.
A neuroradiologist (L.R.) reviewed image quality of the MR angiograms and DSA images. Images were evaluated for overall quality, including vascular signal intensity, venous suppression, and presence of artifacts. Evaluation criteria for overall quality were 1, excellent; 2, more than adequate for diagnosis; 3, adequate for diagnosis; and 4, nondiagnostic.
The DSA images and MR angiograms were rated in a blinded manner. The patient’s name was removed from the images. The DSA images of the right carotid bifurcation were randomized, and the percentage of stenosis was determined. The left carotid images were then randomized and reviewed in a similar manner. The DSA images were evaluated by an experienced neuroradiologist (G.S.).
The MIP MR angiograms obtained in the right and left carotid bifurcations were randomized and reviewed identically for stenosis. The MIP images were reviewed by a neuroradiologist (L.R.) and a neurosurgeon in training at our neuroradiology department (P.S.). No analysis of the source images was performed.
Statistical Analysis
A Spearman rank test was used to find any correlation between findings at DSA and those at MR angiography. Finally, the values of sensitivity, specificity, and positive and negative predictive values were established for the presence or absence of disease that would necessitate surgery (to distinguish stenoses ≥70% from those <70%). For each MR angiogram, the degree of agreement in the interpretation of the degree of stenosis was determined by using the κ coefficient. Agreement was classified as mild (κ > 0.40–0.69), good (κ > 0.70–0.89), or excellent (κ > 0.90–1.00).
Results
In all 120 patients, the quality of both the MR angiograms and DSA images was graded as adequate for diagnosis (grade 3) or better. All MIP MR angiograms included the aortic arch and the circle of Willis within the field of view. No relevant motion artifacts diminished the quality of the MIP images.
Grades of stenoses on MR angiorgams agreed with grades of stenoses on DSA images in 89% of the carotid arteries. The agreement between findings at MR angiography and those at DSA (Fig 1) in the group of severe stenosis (70–99%) was 93% (Table). Underestimation of severe stenosis at MR angiography in comparison to that at DSA occurred in three cases, each with extremely short severe stenoses (Fig 2). Overestimation occurred in two cases, both pseudo-occlusions. In the group of moderate stenosis (30–69%), stenoses of 60–67% in six cases were overestimated (71–84%) at MR angiography.

Agreement between findings at DSA and those at MR angiography.
A, DSA image of the right carotid bifurcation shows a focal severe stenosis (arrow) of the internal carotid artery.
B, The 3D contrast-enhanced MR angiographic MIP image (magnification factor, 2) shows the focal severe stenosis (arrow), correlating well with the DSA image.

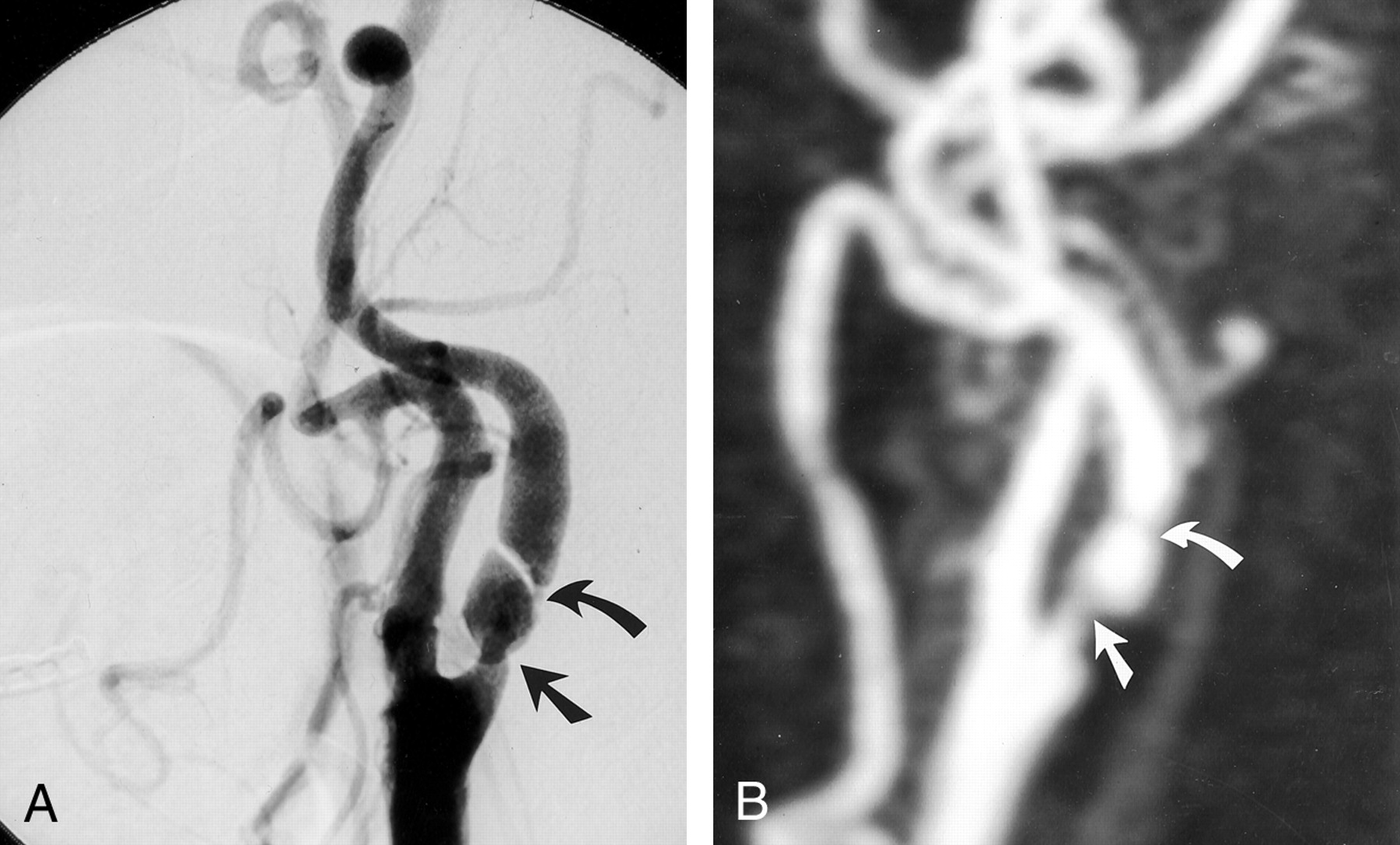
Underestimation of stenoses.
A, DSA image of the left common carotid artery depicts a proximal moderate stenosis (straight arrow) and an extremely short distal stenosis (curved arrow) of the internal carotid artery.
B, 3D contrast-enhanced MR angiographic MIP image (magnification factor, 2) depicts the moderate proximal stenosis (straight arrow) and a short band of decreased enhancement (curved arrow) without clear definition of a stenosis.
Agreement of Contrast-Enhanced MR Angiography with DSA in Evaluation of Carotid Artery Stenosis
All 28 carotid occlusions (Fig 3) were accurately detected with MR angiography. In nine cases, a pseudo-occlusion of the internal carotid artery was suspected during DSA following contrast material injection into the proximal segment of the common carotid artery. MR angiography showed pseudo-occlusion (Fig 4) in seven cases and occlusion in two cases.

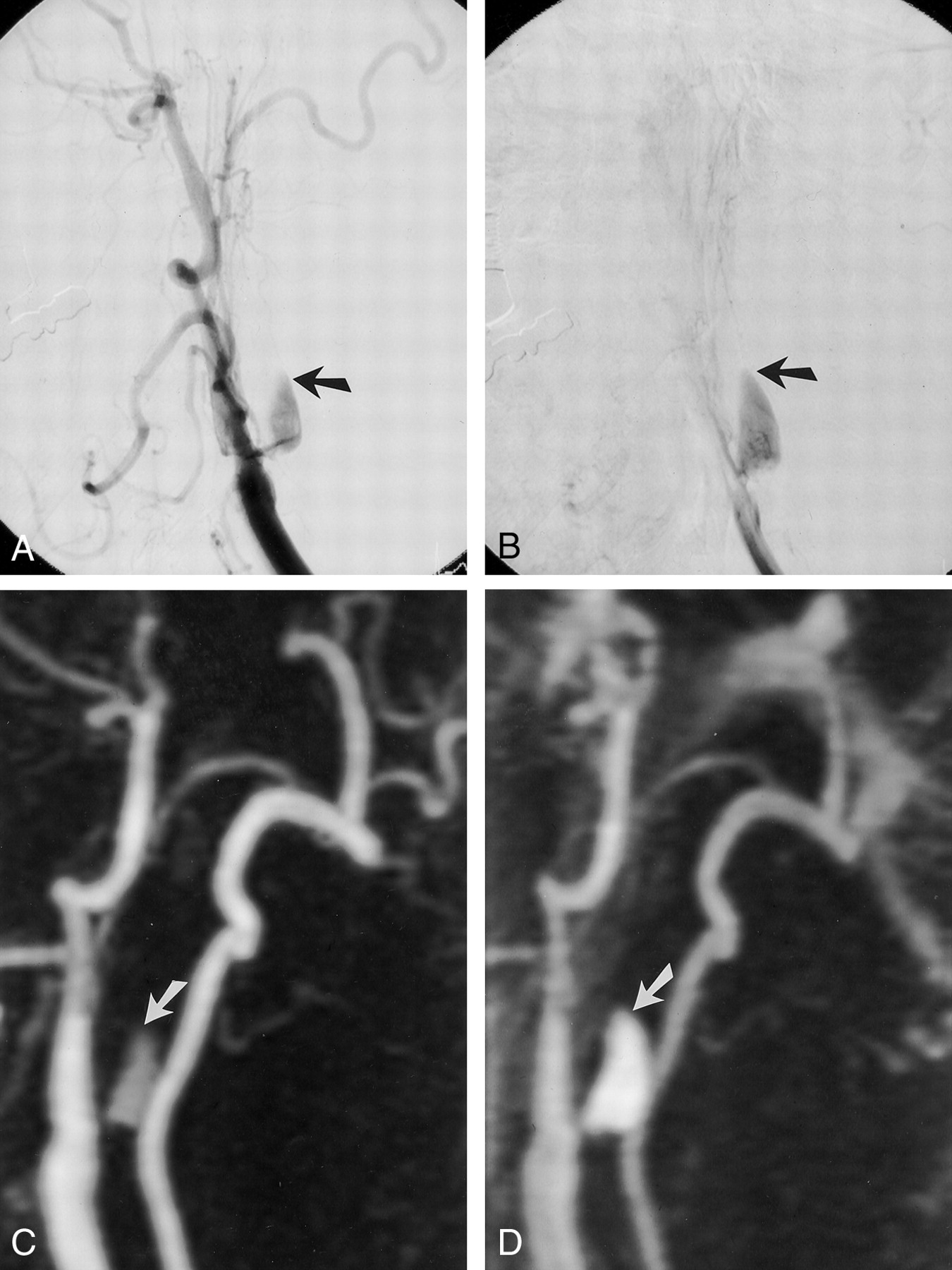
Carotid occlusions.
A and B, DSA images and, C and D, 3D contrast-enhanced MR angiographic MIP images (magnification factor, 1.5) of the left common carotid artery in the early (A and C) and delayed (B and D) phases demonstrate a stump (arrow) at the origin of the internal carotid artery and occlusion of the distal internal carotid artery.

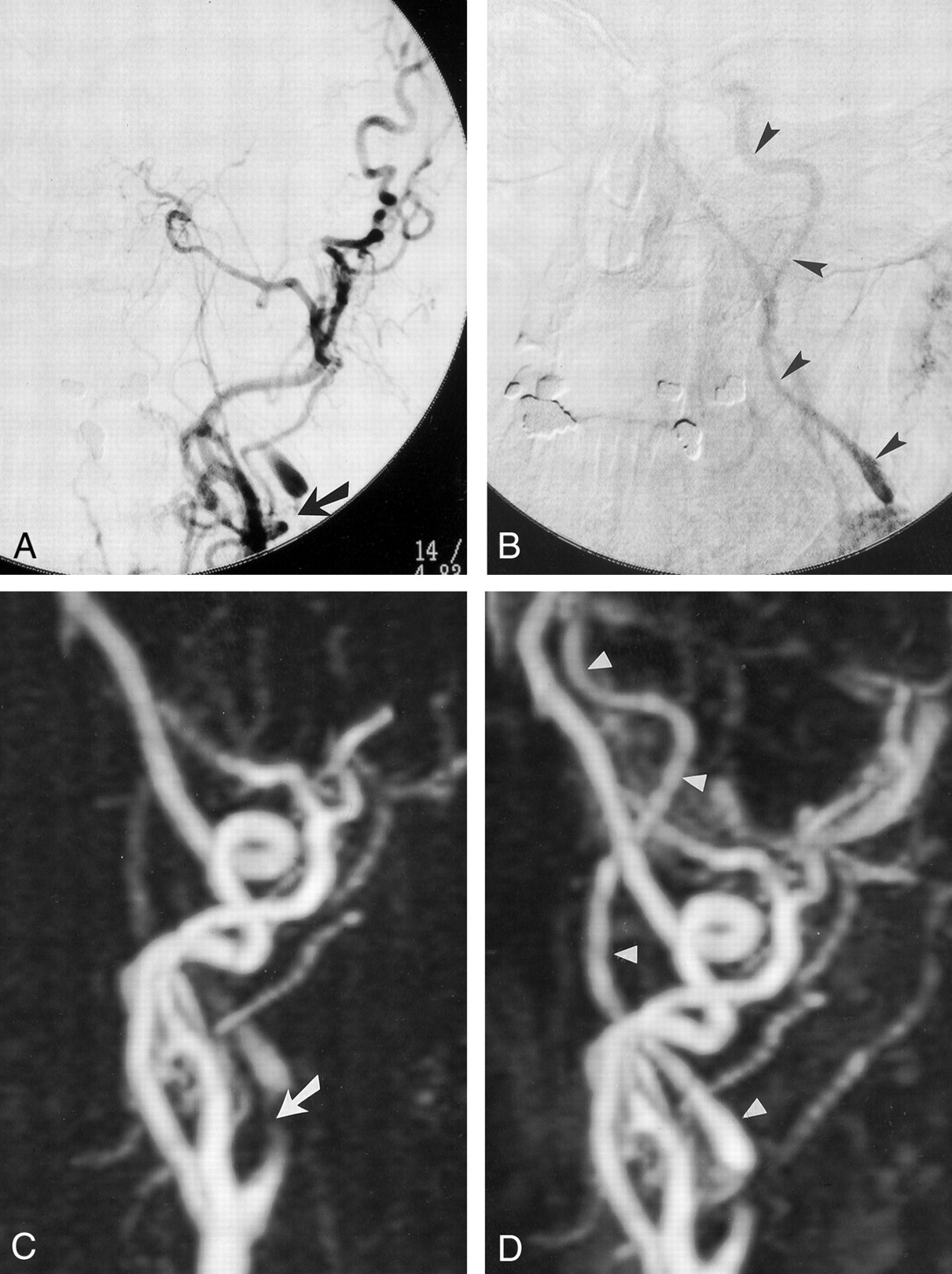
A and B, DSA images of the left common carotid artery demonstrate an extremely severe stenosis (arrow) at the origin f the internal carotid artery in the early phase (A), with collapse of the distal lumen (“string” sign [arrowheads]) in the delayed phase (B).
C and D, The 3D contrast-enhanced MR angiographic MIP images (1.5 magnification factor) demonstrate the extremely severe stenosis (arrow in C) at the origin of the internal carotid artery and opacification of the collapsed distal lumen in only the delayed phase (arrowheads in D).
The sensitivity of all the MIP images was 98%; specificity, 96%; positive predictive value, 95%; and negative predictive value, 98%. The interobserver agreement for classification of degree of stenosis was judged as good for MR angiography (κ = 89). By using the Spearman rank test, comparision of the percentage carotid artery stenosis determined at DSA with that at MR angiography showed a significant correlation (r = 0.91, P < .001).
Discussion
In many preliminary and feasibility studies, various contrast-enhanced MR angiorgaphic techniques have been implemented in the assessment of extracranial disease of the carotid artery. Different strategies are used to optimize image quality, including time-resolved and high-resolution techniques. Most of these reports, although based on small numbers of patients, suggest that contrast-enhanced MR angiography could become a diagnostic alternative as a fast, first screening method in patients suspected of having carotid artery disease, independently from the technique employed in the study.
DSA is still considered to be the criterion standard for imaging of arteriosclerotic supraaortic vessel disease. Harboring the risks of thromboembolic events, this technique can reduce the overall benefit of endarterectomy. Noninvasive techniques for imaging supraaortic vessels prevent this risk related to the diagnostic procedure and can be regarded as a safe alternative to DSA whenever possible.
We chose to compare time-resolved contrast-enhanced MR angiography with high-resolution DSA in 120 patients. The time-resolved technique for MR angiography is comparable to DSA: With one bolus injection of contrast agent, we have the ability to acquire dynamic data during the arterial and venous phases of contrast passage.
In the present study, contrast-enhanced 3D MR angiography was performed with a short TR and a short imaging time, applied in four sequential acquisitions. This sequence has an important advantage: Considering the arteriovenous transit time of 5–15 seconds in the normal cerebrovascular system, and maximal selective intraluminal contrast enhancement of the carotid arteries of 10–25 seconds after intravenous administration of a bolus of contrast material, selective arterial enhancement can be obtained from the aortic arch and the supraaortic arteries up to the circle of Willis. A delay in the arteriovenous transit time due to the presence of an arterial stenosis may actually improve the increase in intraluminal signal intensity during the first pass of the contrast-enhanced blood in the carotid and vertebral arteries. Using a short TE, we were able to reduce flow voids in the intra- and poststenotic regions of the carotid artery, because intravoxel spin dephasing due to fast or turbulent flow can be minimized with this technique. This results in a reduction in the subsequent overestimation of the stenosis, if the remaining vessel lumina are 1 mm or less. In addition, the high signal-to-noise ratio allows visualization of vessels in subvoxel volumes during the first passage of gadolinium-based contrast material. However, the effective resolution exceeds the numerical resolution. In our experience, the minimum accessible vessel diameter is estimated to be between 0.3 and 0.5 mm, thus approaching the resolution limit of DSA. At the level of a stenosis, the minimum accessible vessel diameter increases to approximately 0.8–1 mm.
Because of the rapid acquisition time with four consecutive measurements used in our study, other timing strategies such as a test dose or triggered acquisition would not noticeably improve image quality. The major advantages of this MR angiorgaphic sequence are the rapid acquisition time with subsequent reduction in flow- and patient-related movement artifacts, the high spatial resolution, and the large acquisition volume. However, results of other studies using high-spatial-resolution sequences are also very promising, although larger groups of patient are needed to confirm these results (9, 13, 14, 22, 25, 29).
The NASCET study showed that patients with an internal carotid artery stenosis of at least 70% diameter benefit from endarterectomy (1, 2). More recently, the indication for carotid endarterectomy has been established also for patients with asymptomatic carotid artery stenosis (≥60%) as presented in the ACAS (5).
In our series, the agreement between MR angiography and DSA in the group of severe stenosis (70–99%) was 93%. In three cases, a short severe stenosis of the extracranial internal carotid artery was underestimated with MR angiography compared with DSA. In six cases, a 60–67% internal carotid artery obstruction was overestimated (71–84%) with MR angiography.
An exact differentiation between occlusion and pseudo-occlusion is important for the therapeutic approach and may be a problem when using duplex sonography. All occlusions were correctly detected with MR angiography. In seven cases, pseudo-occlusions of the internal carotid artery were clearly detected with MR angiography. In two cases, pseudo-occlusions assessed with DSA were overestimated (occlusion) with MR angiography. However, retrospectively, a careful analysis of the later-phase MR angiogram showed that the pseudo-occlusion similar to that on the DSA image, according to a very slow blood flow. Thus, in cases of suspected occlusion or pseudo-occlusion, careful analysis of the later-phase image of time-resolved MR angiography is mandatory. A spatial resolution of 1 mm or less is needed.
As an alternative to MIP images, multiplanar reconstruction images can be used for stenosis measurement. We did not use this approach because it is time-consuming and previous reports indicate that measurements with MIP and those with multiplanar reconstruction images do not differ significantly (43, 45). In selected cases, the study of source images could be critical to evaluate subtle lesions (43, 45).
Although no transient or permanent neurologic complication occurred after DSA in our study, carotid angiography remains associated with a substantial number of risks and potential complications. Whereas mortality is low, the frequency of neurologic events varies from 0.45% to 2.6%. In contrast, MR imaging and MR angiography have no known adverse effects and contrast-enhanced MR angiography has a low complication rate. The unlimited number of views from a single acquisition of a carotid bifurcation MR angiographic study can represent an important advantage compared with DSA, in which a minimum of two injections of contrast material are necessary to obtain four views with standard biplane imaging. Another advantage of the contrast-enhanced MR angiorgaphic approach is the ability to display the carotid bifurcation anatomy in a format similar to that of DSA, also in the time resolution. The major advantages of contrast-enhanced MR angiography is the reduction of flow and patient-related movement artifacts, the good spatial resolution, and the large acquisition volume from the aortic arch to the circle of Willis. This allows a good estimation of the degree of carotid stenosis, a differentiation between occlusion and pseudo-occlusion, and detection of tandem stenoses, which is important for clinical and therapeutic management.
In our hospital, contrast-enhanced MR angiography in association with Doppler sonography has now mostly replaced DSA for diagnostic imaging of the cervical arteries. We use contrast-enhanced MR angiography not only as a screening procedure but also for preoperative (endarterectomy) or preinterventional (percutaneous angioplasty and stent placement) evaluation. We still continue to perform DSA in unclear cases. For postoperative follow-up, Doppler sonography plus contrast-enhanced MR angiography is the method of choice to display morphologic results (46).
We believe the further developments in the hardware and software of the new generation of MR imagers will permit a clinically even more sufficient and stable quality of contrast-enhanced MR angiography (47).
Conclusion
Since several clinical trials have proved the benefit of carotid thromboendarterectomy in patients with moderate or severe stenosis, imaging of the carotid artery has been the focus of considerable attention. To reduce risks related to DSA, many noninvasive imaging approaches have been advocated, such as contrast-enhanced MR angiography. Many preliminary and feasibility studies suggest that contrast-enhanced MR angiography could become a diagnostic alternative as a fast screening method in patients suspected of having carotid artery disease, independently from the technique used in the study. The time-resolved technique for contrast-enhanced MR angiography is comparable to DSA: With one bolus injection of contrast agent, we have the ability to acquire dynamic data during the arterial and venous phases of contrast passage.
Our results indicated a statistically significant correlation between contrast-enhanced MR angiography and DSA for minimal, moderate, and severe stenoses and occlusions. This investigation with a large number of patients confirms that contrast-enhanced MR angiography could become a diagnostic alternative to DSA in the treatment of patients with carotid artery disease.
Footnotes
Presented at the 39th annual meeting of the American Society of Neuroradiology, Boston, April 2001.
References
- Received July 24, 2001.
- Accepted after revision November 12, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Appropriate Minimal Dose of Gadobutrol for 3D Time-Resolved MRA of the Supra-Aortic Arteries: Comparison with Conventional Single-Phase High-Resolution 3D Contrast-Enhanced MRA
- Detection of Carotid Artery Stenosis: A Comparison between 2 Unenhanced MRAs and Dual-Source CTA
- Molecular Imaging Changes with Cognition
- Multicenter, Intraindividual Comparison of Single-Dose Gadobenate Dimeglumine and Double-Dose Gadopentetate Dimeglumine for MR Angiography of the Supra-Aortic Arteries (the Supra-Aortic VALUE Study)
- 3D Computerized Occlusion Rating of Embolized Experimental Aneurysms Using Noninvasive 1.5T MR Imaging
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery Developed in Collaboration With the American Academy of Neurology and Society of Cardiovascular Computed Tomography
- Contrast-Enhanced MR Angiography Is Not More Accurate Than Unenhanced 2D Time-of-Flight MR Angiography for Determining >=70% Internal Carotid Artery Stenosis
- Diagnostic Accuracy of Magnetic Resonance Angiography for Internal Carotid Artery Disease: A Systematic Review and Meta-Analysis
- Carotid Stenosis Index Revisited With Direct CT Angiography Measurement of Carotid Arteries to Quantify Carotid Stenosis
- ACCF/SCAI/SVMB/SIR/ASITN 2007 Clinical Expert Consensus Document on Carotid Stenting: A Report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents (ACCF/SCAI/SVMB/SIR/ASITN Clinical Expert Consensus Document Committee on Carotid Stenting)
- Comparison of image quality, diagnostic confidence and interobserver variability in contrast enhanced MR angiography and 2D time of flight angiography in evaluation of carotid stenosis.
- Assessment of CE-MRA for the rapid detection of supra-aortic vascular disease
- Measuring Carotid Stenosis on Contrast-Enhanced Magnetic Resonance Angiography: Diagnostic Performance and Reproducibility of 3 Different Methods
- Contrast-enhanced MR angiography for carotid disease: Diagnostic and potential clinical impact
- Preoperative Evaluation of Carotid Artery Stenosis: Comparison of Contrast-Enhanced MR Angiography and Duplex Sonography with Digital Subtraction Angiography
- Contrast-Enhanced Magnetic Resonance Angiography Carotid Arteries * Response
- Patient Selection for Carotid Endarterectomy: How Far Is Risk Modeling Applicable to the Individual?