
Abstract
Summary: Multiple myeloma involving the thyroid cartilage is exceedingly rare. We describe a patient with progressive airway obstruction due to diffuse involvement of the thyroid cartilage with multiple myeloma. CT revealed a conglomerate of calcifications of the thyroid cartilage. Additional classic lytic lesions of multiple myeloma were subsequently found in the bones, without associated calcifications. Calcified matrix in multiple myeloma involving the thyroid cartilage should now be included as an additional manifestation of extraosseous multiple myeloma.
Multiple myeloma belongs to a group of diseases known as the plasma cell dyscrasias, in which an uncontrolled proliferation of plasma cells, which elaborates a specific immunoglobulin molecule (1, 2). We herein present an unusual appearance of multiple myeloma in an extramedullary location: diffuse calcifications in the thyroid cartilage.
Case Report
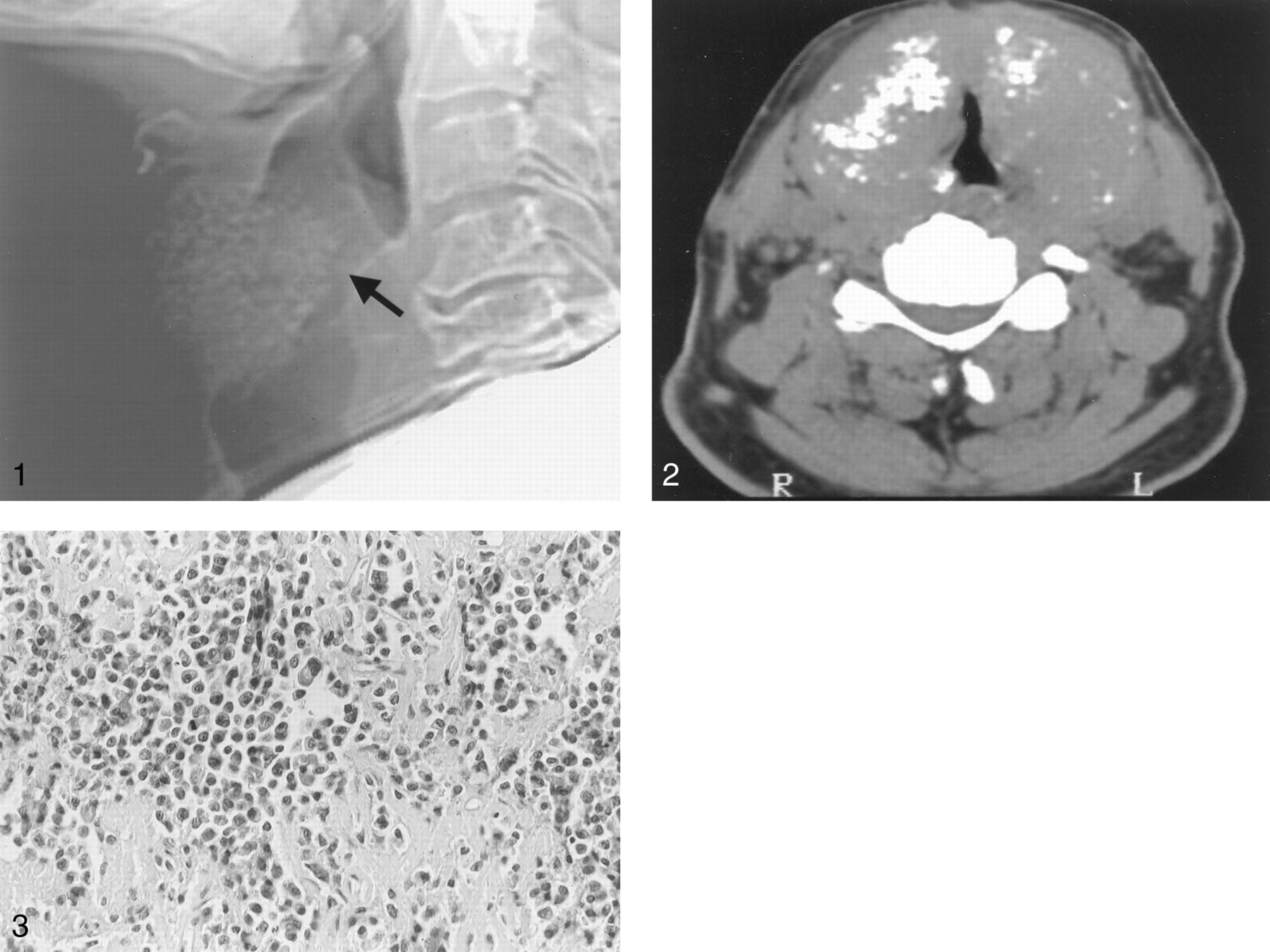
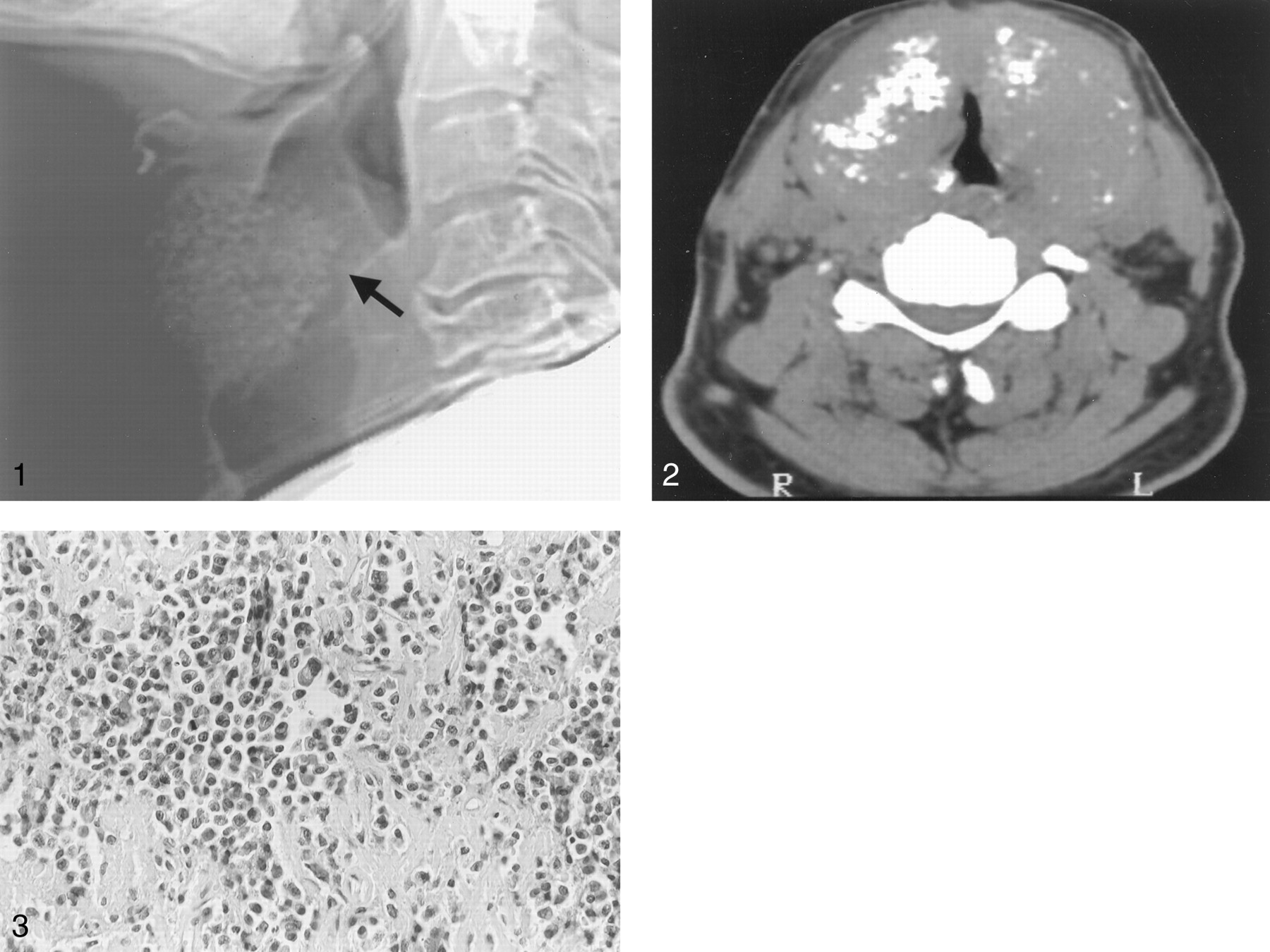
A 54-year-old man presented to the emergency department with increasing hoarseness and progressive difficulty breathing. Two days before admission, he noticed a lump in his neck. Indirect laryngoscopy disclosed severe supraglottic narrowing, with edema of the vocal cords. A lateral scout view of the neck showed a mass containing small coarse calcifications in the anterior part of neck, in the region of the thyroid cartilage. The mass compressed the larynx (Fig 1). A CT scan of the neck displayed enlargement of the thyroid cartilage and a conglomerate of calcifications involving the right and left lamina of the thyroid. Most of the calcifications seemed to be located centrally (Fig 2). Narrowing of the laryngeal and upper airway was also noted. A diagnosis of chondrosarcoma of the thyroid cartilage was made. The patient was admitted to the intensive care unit, where IV steroids were immediately administered. Biopsy of the anterior neck mass revealed diffuse infiltration with multiple myeloma plasma cells (Fig 3). There were no thyroid glandular or cartilaginous remnants in the tissue obtained at biopsy. No amyloid was found with the use of Congo Red stains. A radiologic skeletal bone survey disclosed multiple lytic bone lesions in the skull and the femora. Bone marrow aspirate revealed small groups of plasma cells (<10% per smear) with positive staining for kappa light chains. Elevated immunoglobulin G κ-paraprotein level of 2057 mg/dL were found in the serum. No urine paraprotein was found. A diagnosis of multiple myeloma was made on the basis of plasma cell infiltration of the bone marrow, the lytic bone lesions, the presence of monoclonal immunoglobulins in the serum, and the myeloma plasma cells in the neck mass. The patient underwent local radiation therapy to the neck (1500 cGy) with three courses of chemotherapy (adriamycin, vincrystin, and dexamethasone). After treatment, no change in the size of the mass or degree of upper airway obstruction was present. The patient was therefore referred for further radiation therapy. The dose was increased to 3600 cGy, and the patient subsequently received an immediate dose of melphalan. The course was complicated by febrile neutropenia and severe thrombocytopenia. The patient died after right-sided hemiplegia and aspiration pneumonia.

Lateral scout view of the neck in a 54-year-old man with multiple myeloma of the thyroid cartilage shows a mass containing numerous calcifications in the region of the thyroid cartilage, with compression and narrowing of the larynx and upper trachea (arrow).

Axial CT scans obtained through the upper cervical region. The thyroid cartilage is enlarged bilaterally, with conglomerates of coarse calcifications, mainly in the central area and more evident on the right.

Immunohistochemical specimen. Diffuse infiltration with myeloma plasma cells. With immunohistochemistry, positive staining to the kappa light chain was noted. No amyloid was found (Hematoxylin-Eosin, original magnification ×10).
Discussion
Multiple myeloma belongs to a group of diseases known as the plasma cell dyscrasias, in which uncontrolled proliferation of plasma cells exists, that elaborate a specific immunoglobulin molecule. These single clones of cells proliferate diffusely in the bone marrow, with associated bone destruction, but can give rise to a localized mass in bone, soft tissues, or both.
Multiple myeloma accounts for 1% of all malignancies, with an incidence of four cases per 100,000, and accounts for 10% of hematologic malignancies (1, 2). There are two important variants of multiple myeloma: solitary bone plasmacytoma and extramedullary plasmacytoma. Solitary bone plasmacytoma (SBP) is a localized intraosseous lytic lesion without marrow plasmacytosis. Extramedullary plasmacytoma is a plasma-cell tumor manifesting outside the bone marrow without evidence of systemic disease. Extramedullary plasmacytoma and solitary bone plasmacytoma have a better prognosis, and the patients are at least 10 years younger than those with multiple myeloma. Most authors think that SBP, extramedullary plasmacytoma, and multiple myeloma are different manifestations of the same disease (1, 2). Progression of SBP and extramedullary plasmacytoma to multiple myeloma is the most important feature affecting the prognosis. The disseminated form, multiple myeloma, is by far the most frequent and has the worst prognosis of the three types.
Extramedullary tumors form a small percentage of plasma cell tumors, and although 80–90% of extramedullary lesions occur in the head and neck, they account for <1% of all head and neck tumors (1, 2). Laryngeal involvement accounts for between 6% and 18% of all extramedullary plasmacytoma, with the epiglottis, glottis, false cords, aryepiglottic folds, and subglottis involved (in decreasing order) (3). Involvement of the cricoid cartilage has been observed to occur in patients with overt multiple myeloma as well as in patients with plasmacytoma (2–5). Involvement of the thyroid cartilage by multiple myeloma is exceedingly rare. To our knowledge, the only other CT report of multiple myeloma involving the thyroid cartilage showed a soft tissue mass “contained within arcs of expanded thyroid cartilage, which caused compression of the glottis” (6). This CT appearance is different from the imaging findings in our case, in which the myelomatous infiltration had enlarged the thyroid cartilage with conglomerate of coarse calcifications located mostly centrally.
Radiologically, this appearance resembled, to some extent, the chondroid calcifications seen in chondroid tumors. Chondrosarcoma tumors may arise within the larynx, including the thyroid cartilage; however, these are rare and account for <1% of all malignant laryngeal tumors (7). Several examples have been reported of calcifications that simulate chondrosarcoma, occurring in deposits of amyloid, lying within and produced by the plasma cell tumors (8).
The two mechanisms suggested for cartilaginous involvement in cases of multiple myeloma are direct extension from adjacent plasmacytoma and metaplasia of cartilage to bone, with the formation of a marrow cavity in which plasma cell proliferation can take place. Considering that no plasmacytoma in the tissues adjacent to the thyroid cartilage existed in our patient, the likely mechanism seems to be that of osseous metaplasia of the cartilage with subsequent myelomatous involvement of this extraskeletal marrow.
Calcification in plasma cell tumors may take place under certain circumstances. These include metastatic tissue calcification in patients with an elevated serum calcium-phosphate product, dystrophic calcification in foci of necrotic tissue, calcium accumulation on amyloid deposits within the myeloma, and fragmentation of the metaplastic cartilage from tumor lysis.
In our patient with normal serum calcium levels, the potential mechanism could have been either fragmentation of the metaplastic thyroid or calcium deposition on amyloid. In the other bony lesions, the usual lytic pattern was noted without the presence of any calcifications. Amyloid was ruled out by the lack of positive staining with Congo Red. This left dystrophic calcification in areas of necrosis or fragmentation of the metaplastic cartilage by tumor destruction as the probable explanation.
In summary, at presentation, our patient had signs and symptoms localized to a single region, the supraglottic region of the neck. After a diagnosis of plasma cell tumor was suggested, the subsequent radiologic bone survey disclosed other regions of myelomatous involvement. This case thus illustrates an unusual location of multiple myeloma with a unique radiologic manifestation. Calcified matrix in multiple myeloma should therefore be included as an additional manifestation of extraosseous involvement of multiple myeloma.
- Received May 8, 2001.
- Accepted after revision August 7, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.