
Abstract
BACKGROUND AND PURPOSE: Patients with Laron syndrome have an inborn growth hormone resistance. We investigated abnormalities in the upper airways and cervical spine in patients with Laron syndrome.
METHODS: We prospectively examined 11 patients (one child aged 9 years and 10 adults aged 36–68 years), 10 of whom underwent MR imaging of the spine or head; nine, radiography of the cervical spine; and four, CT of C1-C2. The width of the spinal canal was evaluated visually and quantitatively and compared with reference values. The smallest diameter of the oropharynx and the thickness of the palate were measured and compared with reference values. Nine age-matched female patients referred for MR imaging for unrelated reasons served as control subjects.
RESULTS: Cervical spinal stenosis was present in seven of the adult patients, within a confidence interval of 95%. Anomaly of the dens compatible with os odontoideum was present in three patients, causing focal myelomalacia in two. The atlanto-odontoid joint showed osteoarthritic changes in six of the adult patients. The mediolateral diameter of the oropharynx was significantly smaller in the patients with Laron syndrome than in the control subjects (P < .005). There was no difference in the thickness of the soft palate.
CONCLUSION: Patients with Laron syndrome develop significant narrowing of the cervical spinal canal and early degenerative changes of the atlanto-odontoid joint. Laron syndrome is associated with os odontoideum causing myelomalacia. The dimensions of the oropharynx are small. Patients may be prone to neurologic morbidity and sleep disturbances. Routine MR imaging of the cervical spine is recommended in these patients.
Laron syndrome is characterized by an inability to respond normally to growth hormone of endogenous or exogenous origin (1). Most growth hormone effects are mediated by insulin-like growth factor-1 (IGF-1), which is the anabolic effector hormone of pituitary growth hormone. In Laron syndrome, a defect occurs in the growth hormone receptor gene (2, 3) or the postreceptor pathways, resulting in defects in growth hormone signal transmission and, thereby, a failure to generate IGF-1 (4). The clinical features of Laron syndrome are indistinguishable from those of untreated isolated growth hormone deficiency, but patients with Laron syndrome have high serum levels of growth hormone and undetectable serum IGF-1 (2, 5). Most adult patients with Laron syndrome at our center were found to have sleep disturbances, and some of them were referred for imaging of the upper airway. The aim of the present study was to investigate the abnormal features of the upper airways and cervical spine, which are assumed to be due to congenital IGF-1 deficiency, in patients with Laron syndrome.
Methods
Patients
The study included 11 patients with Laron syndrome (six female and five male patients) who were prospectively examined between April 1999 and September 2001. Ten were adults aged 36–68 years; the single child (female) was 9 years old (Table 1). Diagnosis was based on marked short stature with high basal level of growth hormone and low serum levels of IGF-1. All 10 adults were untreated; the girl had been treated with IGF-1 (150–180 mg/kg/d) since she was aged 3 years. Because these examinations were part of the diagnostic evaluation of sleep apnea, institutional review board approval was not required.
Pertinent clinical data of 11 patients with Laron syndrom
Protocol
Nine patients underwent MR imaging of the cervical spine, and one (patient 5) underwent MR imaging of only the head. We used a system that operates at 0.5 T with a neck coil. Sagittal T1- and T2-weighted as well as axial T1-weighted sequences were performed. The images were reviewed by two radiologists (L.K., G.H.). The width of the spinal canal was evaluated visually and quantitatively, and the anteroposterior diameter of the vertebra was measured; measurements were taken on the sagittal images at the level of C3. The ratio of the two parameters was then calculated and compared with recently published standard values (6). Though the reference values were obtained from lateral conventional radiographs of the cervical spine, we considered them valid also for MR sagittal images because we referred to only the ratio between the parameters. In addition, all abnormal findings were recorded.
Lateral conventional radiographs of the cervical spine were available in nine patients, including one (patient 4) who did not undergo MR imaging. Anteroposterior open-mouth view of the dens and flexion and extension radiographs were obtained at the discretion of the radiologist, or as feasible. Four patients also underwent CT of C1-C2.
The dimensions of the oropharynx were evaluated on the axial MR images. We measured the minimal anteroposterior and mediolateral dimensions (at retropalatal level) and compared the measurements with reference values (7). On the sagittal images, we assessed the maximal thickness of the soft palate and compared it with that of a control group of nine age-matched female patients referred for MR imaging for unrelated reasons.
Statistical Analysis
One-way analysis of variance was performed. P values equal to or less than .05 were considered to indicate a significant difference. Using reference values, we calculated the 95% confidence interval for the spinal ratio between the width of the canal and the vertebral body.
Results
Cervical Spine
Measurements of the cervical spine and description of the abnormal findings are given in Table 2. The most common pathologic finding was cervical spinal stenosis, present in seven of the eight examined untreated patients, with a confidence interval of 95% (Fig 1). The child receiving long-term IGF-1 treatment demonstrated normal width of the cervical spine (Fig 2).

Patient 1. Sagittal T2-weighted images (4000/160/16 [TR/TE/NEX], 4-mm thickness) show stenosis of the cervical spine. Note bulging disks at multiple levels, causing compression of the thecal sac.

Patient 11. Sagittal T1-weighted MR image (450/25/2, 3.2-mm thickness) of the cervical spine shows that the spinal canal is of normal width. Dens is intact. Arrows indicate the level of measurement of soft-palate thickness.
Cervical spine measurements and additional findings in nine patients with Laron syndrom
Atlanto-odontoid Joint
These findings are shown in Table 3. Three patients demonstrated anomaly of the dens. The dens was present but showed a gap between the base and the cranial part, findings compatible with os odontoideum (patients 2, 3, and 4). Flexion and extension radiographs showed atlantoaxial instability. On MR images (available in patients 2 and 3), focal myelomalacia at the C1 level was visible (Fig 3). In the other adult patients (except patient 6), lateral cervical spine radiographs and anteroposterior open-mouth views of the dens revealed an intact dens, which seemed to be bulky and sclerotic. CT scans were available in three of these patients (patients 5, 7, and 9) and confirmed the presence of cortical thickening of the dens and the atlas, with narrowing of the atlantoaxial joint, compatible with degenerative changes. On MR images, compression of the subarachnoid space was seen at the same level (Fig 4). In patient 6, both conventional radiographs and MR images of the C1-C2 region revealed no abnormalities.

Patient 3.
A and B, Lateral flexion (A) and extension (B) radiographs of the cervical spine. Dens is not visualized. Atlantoaxial instability is demonstrated. Note the small vertebral bodies and the narrow cervical canal.
C, Sagittal reconstruction of CT data obtained at C1-C2 shows a gap between the base of the dens and the small bone above it, compatible with os odontoideum.
D, Sagittal T2-weighted MR image (4600/160/1) shows stenosis of the cervial spine. A focus of myelomalacia is seen at the C1-C2 level. High signal intensity from the region of the disrupted dens probably represents reactive tissue.

Patient 9.
A, Lateral radiograph of the cervical spine shows the dens, which appears thickened and sclerotic.
B, Sagittal reconstruction of CT data obtained at C1-C2 shows no malformation of the dens. Note the cortical thickening and the narrowing of the atlantoaxial joint, possibly compatible with degenerative changes.
C and D, Sagittal T1-weighted (C; 500/20/2, 4-mm thickness) and T2-weighted (D; 4000/160/1, 4-mm thickness) MR images show a thin dens. Note the mild compression of the subarachnoid space at the C1-C2 level owing to cortical thickening and sclerosis of the dens.
Findings at the atlanto-odontoid joint in 10 untreated patients with Laron syndrom
Oropharynx
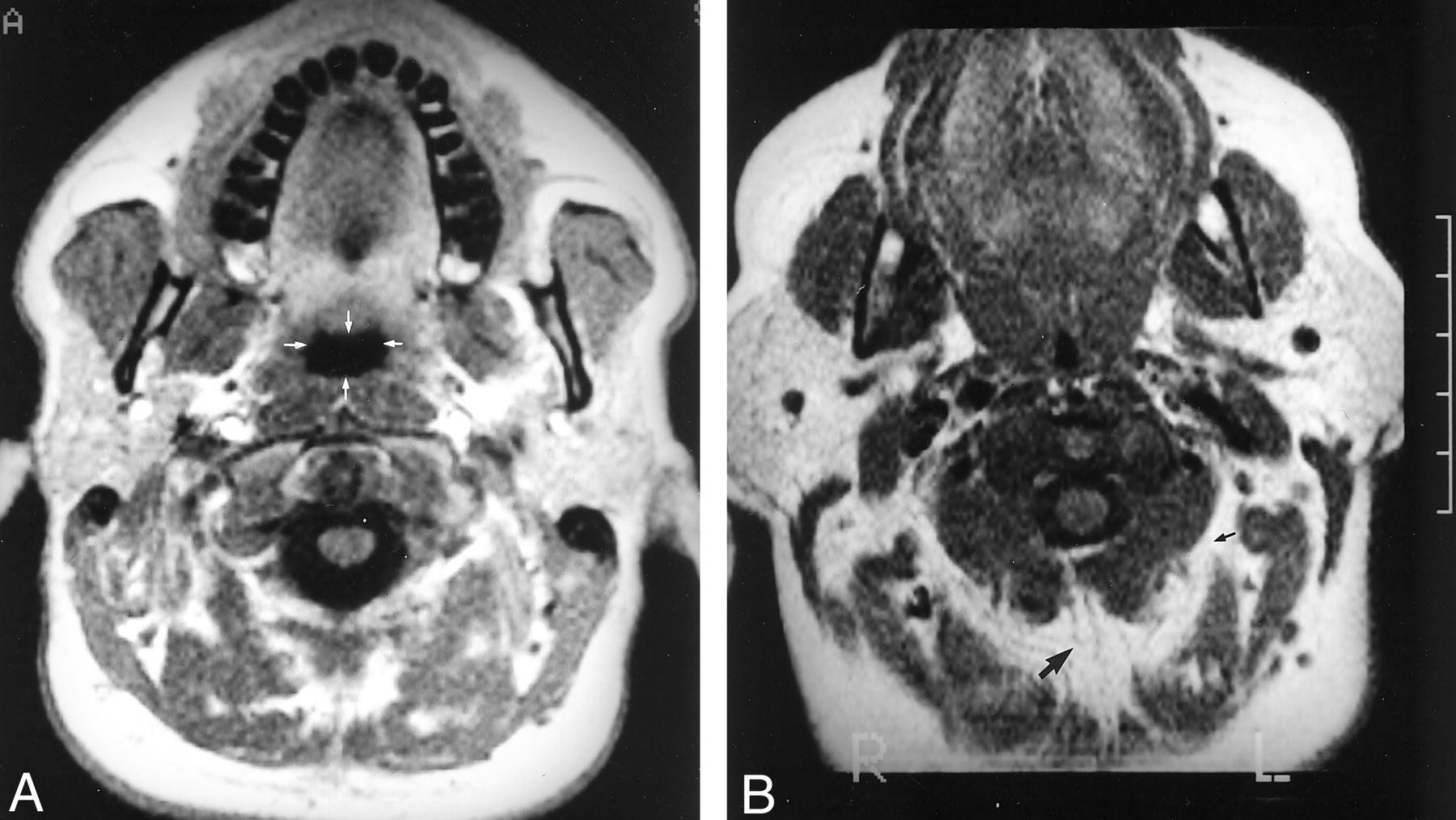
MR images of the oropharynx were available in nine patients (Table 4). (In patient 8, MR imaging was performed with the patient under general anesthesia and was therefore not diagnostic.) The minimal mediolateral diameter of the oropharynx was significantly smaller in patients with Laron syndrome than in control subjects (P < .005). There was no significant difference in the anteroposterior diameter or in the thickness of the palate between the two groups (Table 4, Fig 5).

Axial T1-weighted (500/20/2, 5-mm thickness) MR images of the oropharynx.
A, MR image in control subject for comparison. Arrows indicate the anteroposterior and mediolateral diameters.
B, MR image in patient 5. Oropharynx is strikingly small. Note the abundance of adipose tissue (arrows) between the muscles.
Oropharynx measurements in nine patients with Laron syndrome compared with the normal mea
For the treated child, no reference data were available owing to her young age.
Discussion
Laron syndrome, also known as primary growth hormone resistance or insensitivity syndrome (1), was first described in 1966 and 1968 in a group of Oriental-Jewish patients (8, 9). Since then, hundreds of patients have been reported worldwide, mostly of Mediterranean or Middle Eastern origin (10, 11).
Laron syndrome is an autosomal recessive disease caused by deletions (11) or mutations in the growth hormone receptor gene (2, 3) or the postreceptor pathways (4), resulting in defects in growth hormone signal transmission and, thereby, an inability to generate IGF-1. IGF-1 is the anabolic effector hormone of pituitary growth hormone. Therefore, affected patients fail to respond to growth hormone of either endogenous or exogenous origin.
Clinically, these patients show progressive dwarfism, with final stature ranging from 3 feet 6 inches (108 cm) to 4 feet 5 inches (136 cm) in women and 3 feet 10 inches (116 cm) to 4 feet 8 inches (142 cm) in men (2, 5, 10). Acromicria, organomicria, and small genitalia and gonads are other common features (8–10). Craniofacial abnormalities include subnormal head circumference (9, 10) and underdevelopment of the facial bones (12, 13); nevertheless, head size is large relative to the short stature. All the children and many of the adults have a high-pitched voice. As adults, they become more and more obese and have hypercholesterolemia and insulin resistance (5). Though both skeletal and sexual maturation are retarded, affected individuals eventually mature and have full reproductive ability (10). With the development of biosynthetic IGF-1, treatment is now feasible (14) but has been offered to only a few children owing to its limited availability.
Only a few radiographic or imaging studies of patients with Laron syndrome have been published so far. These studies reported retarded skeletal maturation (10, 15) or underdevelopment of the facial bones (12, 13), delayed closure of the fontanelle (9), and thin bones (5, 10, 15). Our report shows that congenital deficiency of IGF-1 due to growth hormone insensitivity causes a significant narrowing of the cervical spinal canal and is associated with anomalies of the dens, degenerative changes of the atlanto-odontoid joint, and smaller dimensions of the oropharynx.
Pituitary growth hormone and IGF-1 are the major hormones involved in postnatal longitudinal growth. Growth hormone acts on the differentiation of the prechondrocytes into early chondrocytes, which are then able to respond to IGF-1, which stimulates the division and maturation of the chondrocytes, causing growth (16). This mechanism of growth is present both in the physis of the long bones and in the proliferating cartilage on the upper and lower zones of the vertebral bodies (17). Therefore, growth hormone resistance, such as that in Laron syndrome, results in short stature and acromicria (8–10). In the patients in the current study, we noted an additional characteristic feature: cervical spinal stenosis. The spinal canal grows at the neurocentral synchondroses between the body and the arches of the vertebrae until ages 3–6 years and thereafter only by the midline posterior cartilage between the two arches until age 10 years (17). In patients with growth hormone resistance who lack IGF-1, the capacity for growth in these regions is limited, resulting in a narrow spinal canal; this was demonstrated in seven of the eight examined untreated patients with Laron syndrome. This anatomic configuration places affected patients at greater risk of neurologic deficit at the occurrence of degenerative disk disease and spondylotic changes. Indeed, in one of our patients (patient 1), disk bulge with compression of the thecal sac was evident already at age 36 years. Further studies are needed to evaluate the thoracic and lumbar spine to determine the extent of this anomaly.
The findings at the C1-C2 level are also noteworthy. In three patients, an abnormality of the dens was detected. Aplasia or hypoplasia of the odontoid process is extremely rare and has been reported in association with a variety of congenital dysplasias (18), but not with growth hormone deficiency or insensitivity. Here, the anomaly seems more compatible with os odontoideum. The etiology of os odontoideum remains controversial: Both acquired and congenital mechanisms have been proposed (19, 20). In our patients, the combination of the spinal stenosis and atlantoaxial instability due to the disruption of the dens caused repeated pressure on the cord and focal myelomalacia (21).
In all the other adult patients (except patient 6), the CT or/and conventional radiographs disclosed sclerosis and thickening of the dens with narrowing of the atlanto-odontoid joint. Because of its function and situation, the atlanto-odontoid joint is subject to degenerative changes. These changes are similar to those commonly observed in other synovial joints and are rarely found before age 50 years (22, 23). Only one of our patients was older than 50 years, so the high frequency of degenerative changes observed here is unusual. We suggest that in Laron syndrome the disproportion between head and body size (9, 10) subjects the atlas and dens to increased stress, resulting in thickening and sclerosis at a young age. This disproportion may also be a factor in the increased risk of overstretching of the vascular supply of the dens in the event of trauma, resulting in avascular necrosis and a high frequency of os odontoideum, as seen in our patients.
We also found that in patients with Laron syndrome, the dimensions of the oropharynx were small compared with normal standards (Table 4). Postnatal craniofacial growth appears to be a complex multifactorial process. Currently, all the theories of growth-control mechanisms are speculative. One of the most popular is the functional matrix hypothesis, which proposes that the craniofacial bone grows in response to the structures surrounding it. That is, the pharynx enlarges because of the functional demands for airway, breathing, and eating spaces concomitant with linear growth (24).
The small size and small quantities of food ingested in combination with the IGF-1 deficiency are probably the cause of the impaired growth of the pharynx in patients with Laron syndrome, leading also to the characteristic high-pitched voice. One of the most important clinical outcomes of impaired pharyngeal growth is a greater propensity for sleep apnea (Z. Laron, unpublished data, 2001), noted in several of our patients. Indeed, early cephalometry studies in patients with apnea who have normal stature showed that mandibular, maxillary, and anterior cranial base length are decreased (25), and the minimum airway area is significantly smaller than normal (7, 26). Interestingly, not only size but shape is affected, with the predominant narrowing in the mediolateral dimension resulting in an oval shape, with the longest axis in the anteroposterior dimension rather than the mediolateral dimension (7). All these anatomic features, including narrowing of the airways in the transverse plane (Table 4), are present in patients with growth hormone insensitivity (12, 13). Furthermore, obesity is an important factor in the development of sleep apnea (27). Adult patients with Laron syndrome are characteristically overweight, with a markedly increased fat mass (5, 10).
Conclusion
Untreated patients with Laron syndrome develop cervical spinal stenosis and early osteoarthritic changes of the atlantoaxial joint, and have a small oropharynx. Laron syndrome is associated with os odontoideum. These findings stress the need for IGF-1 replacement treatment in these patients early in childhood. MR screening of the cervical spine is recommended in untreated patients with either growth hormone or IGF-1 deficiency.
Acknowledgments
The authors thank Schlormo Michael and Zvi Cohen for their technical assistance, and Charlotte Sachs and Gloria Ginzach, of the Editorial Board, Rabin Medical Center, Beilinson Campus, for their assistance.
References
- Received April 3, 2001.
- Accepted after revision January 2, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.