
Abstract
Summary: Sphenoid sinus mucocele is an uncommon lesion related to inflammatory disease that is diagnosed after surgery or a traumatic event. This report describes an unusual case revealed by bacterial meningitis and cerebral abscess in a 12-year-old child. CT and MR imaging allowed precise extension to the skull base in preoperative management and follow-up investigations. Endoscopic transnasal marsupialisation of the mucocele and antibiotic therapy led to complete remission. There was no evidence of recurrence after 6 months, which suggests that sphenoid mucoceles, regardless of size and complications, can be treated by endoscopic sinus surgery.
Sphenoid sinus mucocele is rare (1, 2) and generally caused by direct trauma (3). Patients with these lesions present with various symptoms and signs that may include nasal problems (4) and cranial nerve palsy (5–7). Few cases have been reported in children (8, 9), and the spontaneous case described here appears to be the first diagnosed in a child in conjunction with an infectious brain complication. Since the introduction of endoscopic techniques and instruments, the efficiency of the transnasal route has been evaluated for sphenoid mucocele removal (10, 11). There is increasing evidence in the literature that endoscopic surgery is safe and has a very low rate of recurrence. In our opinion, the transnasal approach is valid even for the management of complicated sphenoid mucocele.
Case Reports
A 12-year-old boy seen in the pediatric emergency department of the Nantes Teaching Hospital complained of severe diffuse headache and persistent fever. He had no history of cranial traumatism, sinus surgery, or chronic sinusitis. Clinical examination revealed typical acute meningitis but no neurologic palsy or ocular complications. CSF assessment confirmed a bacterial pneumococcus–related infection. Treatment was initiated in the emergency department (injection of amoxicillin 200 mg/kg/day). CT and MR imaging revealed a sphenoid mucocele eroding adjacent bone in the roof of the sinus, associated with a 2-cm-diameter brain abscess diameter situated in the right inferior frontal area (Figs 1 and 2).

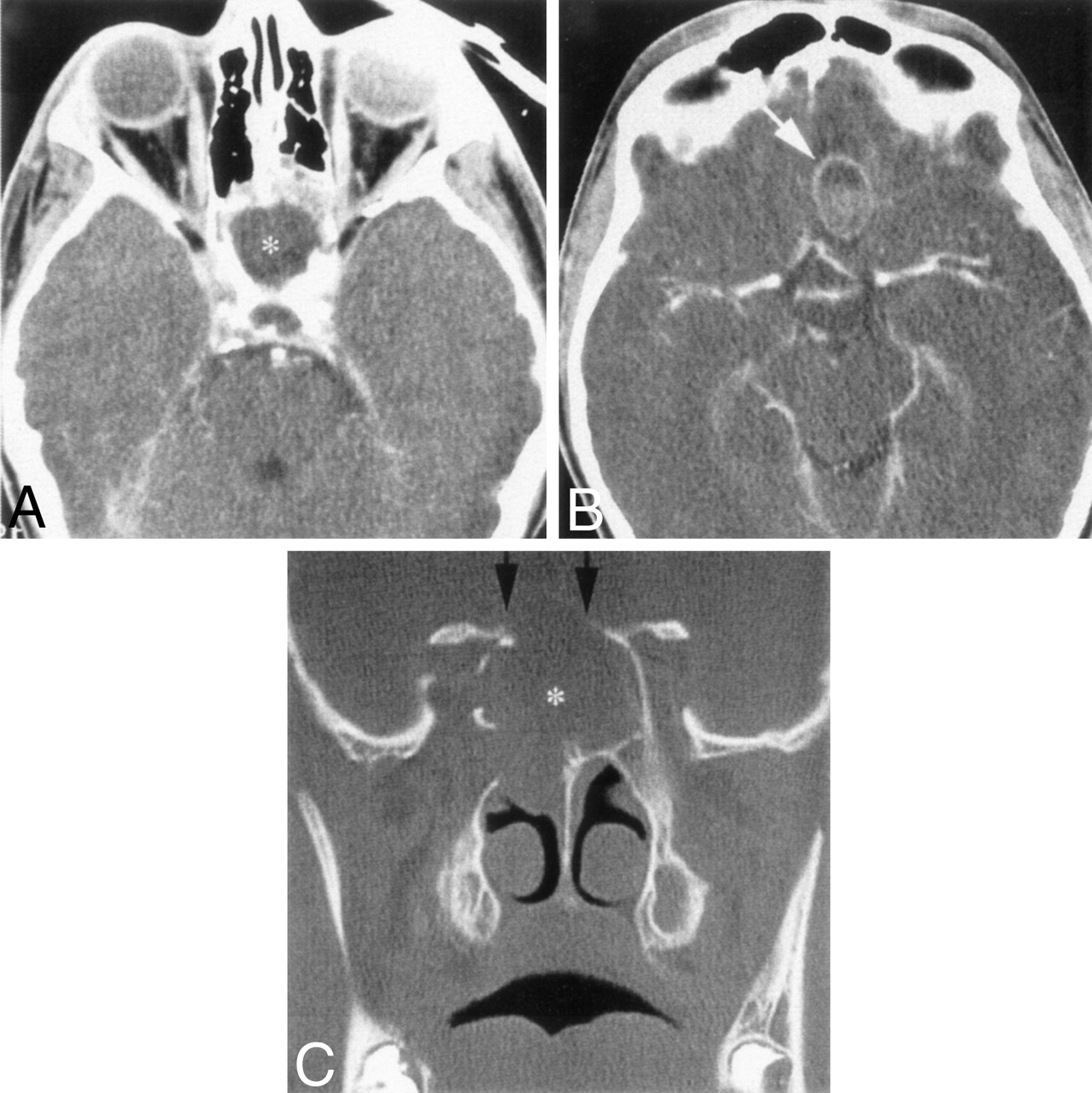
Preoperative CT scans
A, Axial scan showing abnormal opacification of the sphenoid sinus (asterisk [*]).
B, Axial scan showing a right frontal brain abscess (arrow) up to the sphenoid sinus.
C, Coronal scan revealing the sphenoid sinus mucocele (asterisk [*]) with osseous erosion of the sinus roof (arrows).

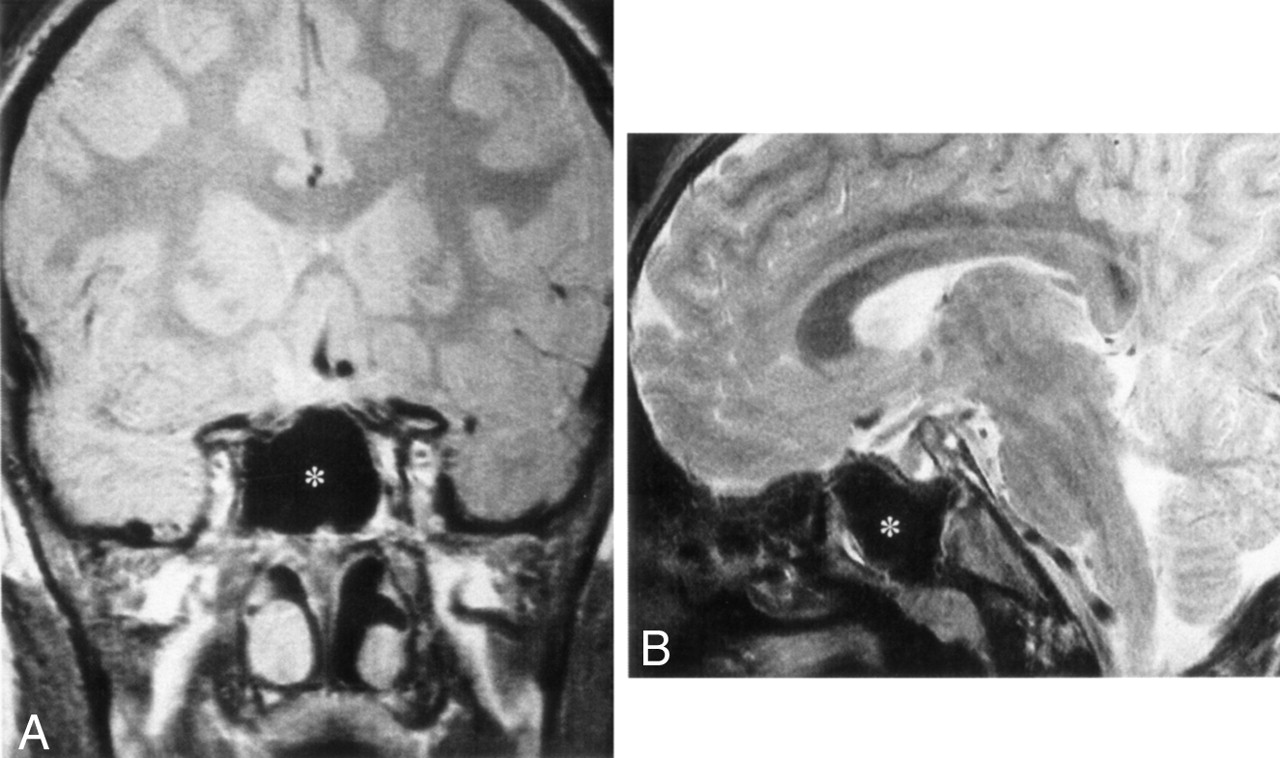
Preoperative T1-weighted MR images.
A, Coronal MR image showing abnormal opacification of the sphenoid sinus (asterisk [*]).
B, Right parasagittal MR image showing the sphenoid sinus mucocele (asterisk [*]) and the adjacent frontal brain abscess (arrow).
Surgical drainage was performed under general anesthesia 48 hours after antibiotic induction. The patient underwent a bilateral endoscopic procedure by the transnasal route, with video monitoring. A huge mucocele was easily located, emerging from the right sphenoid anterior wall above the choana. Bacteriologic analysis of the pus in the mucocele showed numerous leukocytes, but no bacteria. Marsupialisation was gradually achieved after endoscopic instruments were used to enlarge the sphenoid sinus. Complete removal of the mucocele produced a large opening of the rostrum. Bone erosion in the roof of the sinus had allowed the dura mater to enter the sphenoid sinus cavity (Fig 3). There was, however, no interruption of the dura mater and no CSF leakage. At the end of marsupialisation, a Merocel sponge (Medtronic Xomed, Saint Aubin Le Monial, France) was placed in the nasal cavity for 24 hours to prevent bleeding.

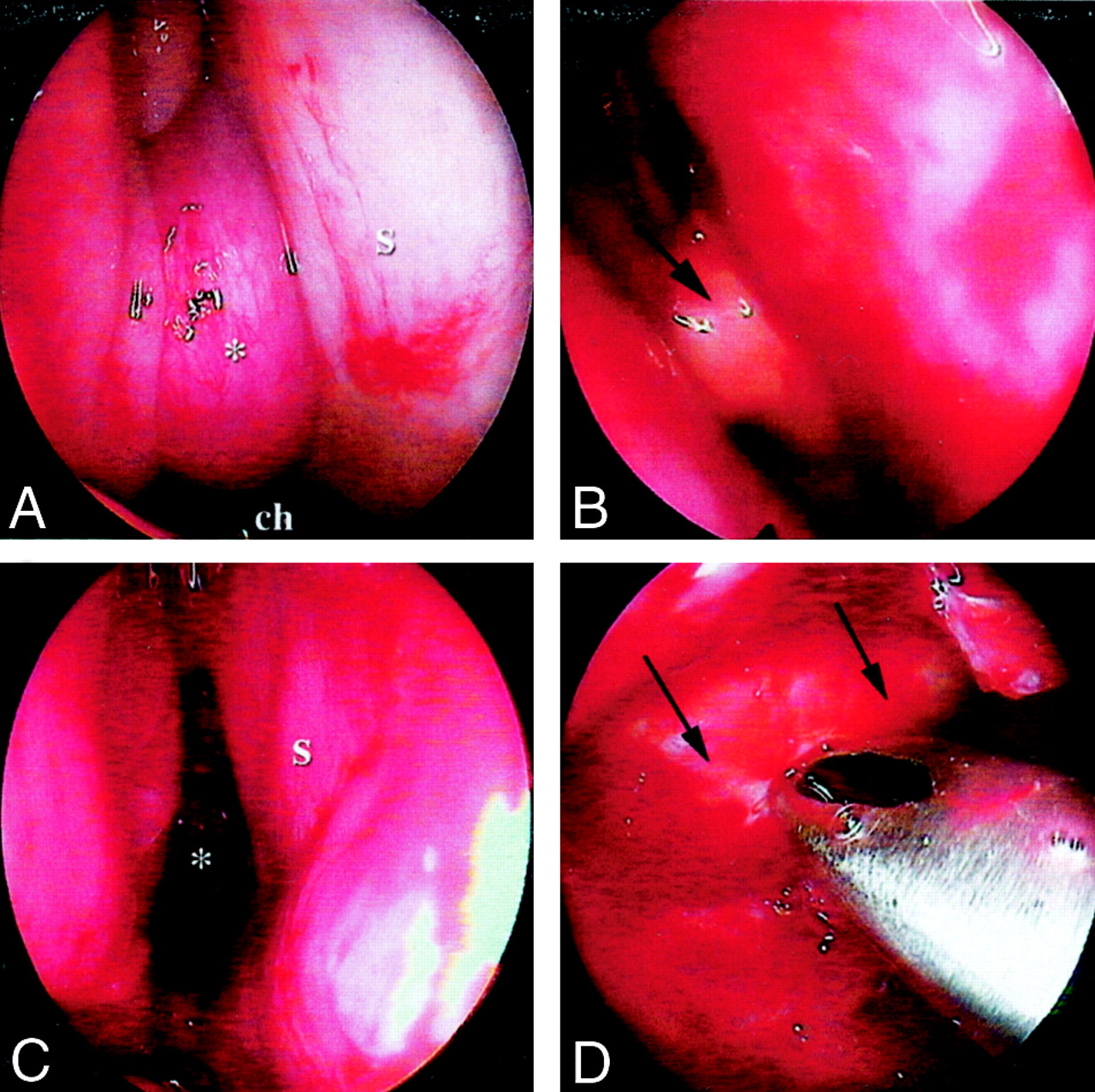
Endoscopic perioperative management.
A, Endoscopic view (0°) by a right transnasal route showing the mucocele (asterisk [*]) up from the choana (ch) and laterally from the nasal septum (s).
B, Endoscopic view (0°) after opening of the mucocele, showing a huge pus discharge (arrow).
C, After marsupialisation of the mucocele, 0° endoscopic view of the right sphenoid sinus (asterisk [*]) lateral and posterior to the nasal septum (s).
D, Endoscopic view (60°) inside the left sphenoid cavity, showing bone erosion of the sinus roof. Dura mater, inspected directly by endoscopy, was not ruptured (arrow).
The patient had no postoperative complications. Because of its depth, the brain abscess was not surgically treated first. The patient’s course was rapidly satisfactory under antibiotics. After 10 days, injections were replaced by oral administration of 6 g/day of amoxicillin, and the patient was allowed to return home. Antibiotics were maintained for 10 weeks, until CT and MR control imaging showed complete extinction of the brain abscess. No signs of recurrence were observed after 6 months of follow-up (Figs 4 and 5).

Postoperative axial (A) and coronal (B) CT scans 4 months after marsupialisation, showing normal opening and ventilation of the sphenoid (asterisk [*]). There is no evidence of recurrence of the mucocele and no outstanding abscess.

Preoperative coronal (A) and sagittal (B) T1-weighted MR images showing normal ventilation of the sphenoid sinus (asterisk [*]) and complete abscess extinction.
Discussion
Trauma and chronic inflammation (polypoid sinusitis) are frequent causes of mucocele (3). In addition, many of the mucoceles are simply related to inflammatory disease, without accidental or postsurgical evidence; to our knowledge, mechanisms of expansion have not been elucidated in literature. The development of a sphenoid mucocele in a child has been reported in only a small number of articles (6, 9, 12).
To our knowledge, this clinical case is the first report of sphenoid mucocele in a child revealed by meningitis and a brain abscess. Because sphenoid sinus mucoceles represent only about 1% of all paranasal mucoceles (11), it is difficult to determine their standard clinical features. Pain (vertex or occipital headache) seems to be the most common symptom (1), and eye-threatening complications often reveal the lesion.
Accurate imaging is required to define the precise extension and boundaries of the mucocele. Both CT and MR imaging are recommended before a surgical approach (13). Mucoceles can show various imaging features, depending on the contents (especially water). When the water rate is high, the space occupied by the lesion is hypoattenuated at CT. The sinus wall may be very thin because of constant and prolonged pressure and be conducive to extensive destructive growth on surrounding components. Sinus cavities are hypointense on T1-weighted MR images and hyperintense on T2-weighted MR images but without enhancement. Because of a large increase in the protein rate, a hyperintense signal can be observed on T1-weighted MR images. Thus, in some cases, images can be very difficult to analyze.
An external surgical approach was used in the past for mucocele management, but an exclusively endoscopic transnasal route has become the standard and generally uncontested treatment (4, 11). Some authors, however, have suggested using an endoscopic technique combined with a navigating system (14). In our opinion, the transnasal approach is valid even for the management of complicated sphenoid mucoceles regardless of their size and preoperative complications. This type of treatment is clearly radical, postoperative care is reduced, and sequelae are quite limited.
References
- Received May 21, 2003.
- Accepted after revision August 26, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.