
Abstract
Summary: We describe a case of traumatic pseudoaneurysm of the middle meningeal artery in a patient after a head trauma. The aneurysm was found incidentally and resolved spontaneously without any intervention; this outcome suggests that middle meningeal artery aneurysm may not require treatment in all cases and can be followed conservatively with follow-up conventional angiography.
Aneurysms of the middle meningeal artery are rare, and most present with intracranial hemorrhage and are therefore treated (1). However, the natural history of middle meningeal artery aneurysms, particularly when discovered incidentally, remains unclear. We report a traumatic pseudoaneurysm of the middle meningeal artery discovered incidentally, which spontaneously regressed at 1-month follow-up; this finding suggests that these pseudoaneurysms may not require treatment in all cases.
Case Report
A 39-year-old male construction worker fell 2 stories from a roof. At the scene, he was awake and moving all 4 extremities and then had a witnessed seizure. He was intubated and sedated. Findings of physical examination showed lacerations of the forehead and the left orbit and bilateral hemotympanum. He was extubated the next day, and his neurologic examination revealed a left sixth nerve palsy and incomplete left facial weakness.
CT of the head demonstrated pneumoencephaly, traumatic subarachnoid hemorrhage, and a small left epidural hematoma. An extensive basilar skull fracture and multiple facial fractures were seen. CT angiography revealed a small smoothly rounded superior hypophyseal aneurysm. Angiography of the internal carotids was performed, which confirmed this finding; external carotid injection was not performed at this time. Although the possibility of traumatic pseudoaneurysm could not be excluded, the lesion had the appearance of a saccular nontraumatic aneurysm and was followed conservatively.
On hospital day 3, the patient developed brisk epistaxis. Internal carotid angiography was performed, largely to exclude rupture of the known superior hypophyseal artery aneurysm into the sphenoethmoidal sinuses. Findings showed no change in the superior hypophyseal aneurysm and no source of epistaxis. The external carotid arteries were then injected in preparation for embolization to arrest the epistaxis. The left external carotid injection revealed an irregular aneurysm of the middle meningeal artery. Embolization of the internal maxillary artery distal to the middle meningeal artery with polyvinyl alcohol particles (150–250 μm) was uncomplicated, and the epistaxis was arrested. No treatment of the middle meningeal artery aneurysm was performed at this time.
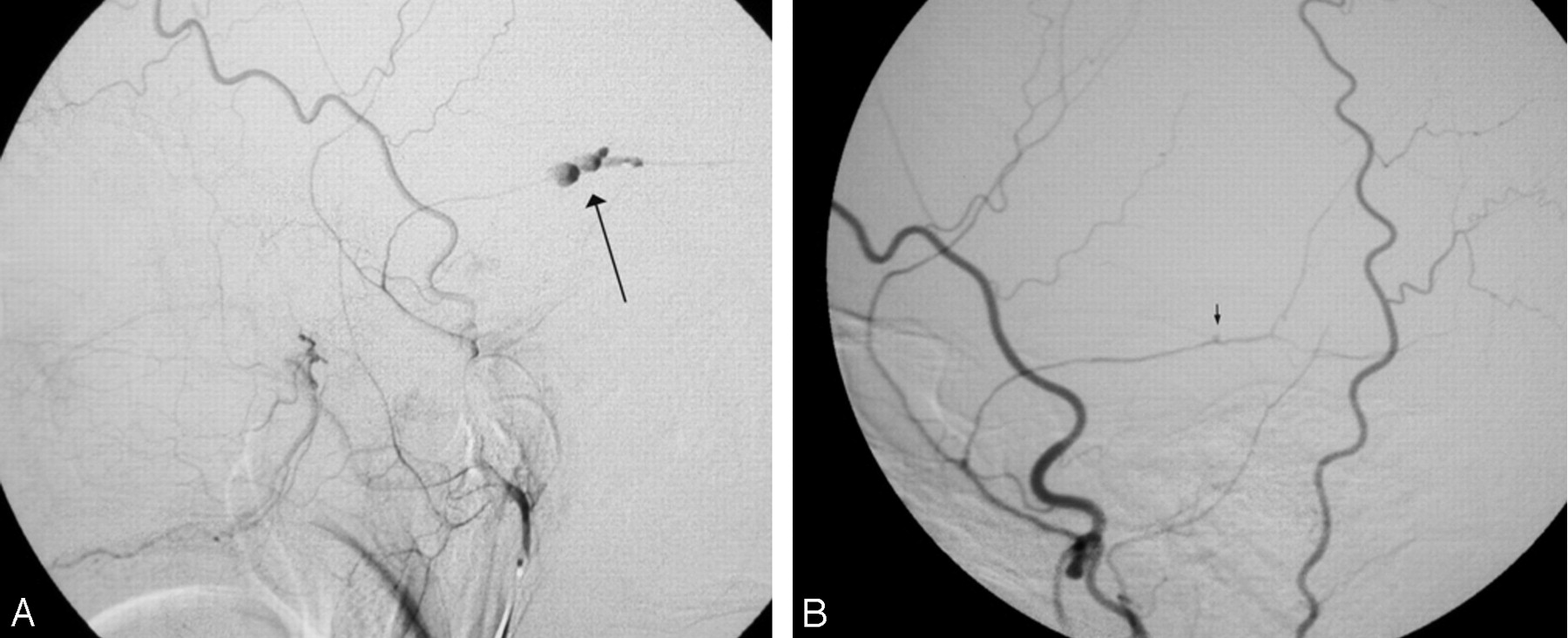
During the next few days, the patient’s condition improved, and he was discharged home. Follow-up angiography 1 month later showed no change in the aneurysm of the superior hypophyseal artery. External carotid injection revealed that the middle meningeal artery aneurysm had resolved, with only a subtle contour abnormality evident at the affected segment (Fig 1A, -B).

A, Lateral film from conventional angiography shows contrast agent filling an irregular aneurysm along the course of the posterior division of the middle meningeal artery (arrow). This aneurysm is presumed to be a pseudoaneurysm on the basis of its configuration.
B, After 1 month, a follow-up repeat angiogram shows a subtle contour abnormality along the posterior division of the middle meningeal artery (arrow).
Discussion
Seventeen cases of nontraumatic aneurysm and 40 cases of traumatic pseudoaneurysm of the middle meningeal artery have been reported in the literature (2). Nontraumatic aneurysms of the middle meningeal artery have been found in association with meningioma, Paget’s disease, angioma, moyamoya, cavernous hemangioma, hypertension, posterior cerebral artery occlusion, dural arteriovenous malformation, and neurofibromatosis type 2 (3–6). Nearly all cases of traumatic middle meningeal artery pseudoaneurysms are associated with fracture that extends across the temporal region of the middle meningeal artery (2). Both traumatic and nontraumatic middle meningeal artery aneurysms are associated with epidural, subdural, subarachnoid, intraparenchymal, and intraventricular hemorrhage (7).
The first case of traumatic middle meningeal artery pseudoaneurysm was reported by Schulze in 1957 (8). The natural history of traumatic middle meningeal artery pseudoaneurysms is unknown, and different theories explain the formation of the middle meningeal artery aneurysm. Bruneau et al (2) postulated that the traumatic pseudoaneurysm develops from the partial transection of the meningeal artery, which is not large enough to give rise to an acute epidural hematoma. Extravasated blood is rapidly contained by the clot formation, which remains in continuity with the arterial lumen. The sac of the traumatic pseudoaneurysm is then formed by the fibrous organization of the clot within a few days (9). Histologically, none of the normal arterial layers are present, and a fibroconnective tissue surrounds a hole in the arterial wall. Eighty-five percent of traumatic pseudoaneurysms are found in the temporal region, 10% are occipital, and 5% are frontal (7). There have been case reports of association of middle meningeal artery pseudoaneurysm with arteriovenous fistula (10), which can resolve spontaneously without surgical treatment. On the other hand, traumatic pseudoaneurysms tend to develop delayed hemorrhages (11). Angiographically, traumatic middle meningeal artery pseudoaneurysms are peripherally located, at a distance from a branching point, and do not show evidence of a neck. The sac is generally irregular, with delayed filling and emptying so that the contrast medium has time to settle at the bottom of the aneurysm and the pre- and postaneurysm segments of the meningeal artery are not opacified at the same time. These features explain why traumatic middle meningeal artery pseudoaneurysms are usually visible only in the late injection stages of the selective external carotid angiography (2, 9).
Our case is unusual because we found a middle meningeal artery pseudoaneurysm incidentally while performing embolization of the internal maxillary artery for epistaxis. Although we considered that the middle meningeal artery was inadvertently occluded during the embolization, this possibility seemed highly improbable for several reasons: First, the tracker catheter was positioned in the distal internal maxillary artery well beyond the takeoff of the middle meningeal artery. Second, the embolic material was mixed with dilute contrast material and injected under fluoroscopic visualization to ensure that there was no reflux. Finally, an image taken at the completion of the embolization demonstrated that there was no vasospasm and the descending palatine and infraorbital artery trunks were still patent. If these vessels downstream of the emboli were still open, then it is unlikely that the upstream middle meningeal artery could have been occluded by errant emboli material.
It is unknown how many patients with skull fracture and/or asymptomatic epidural hematoma will have abnormalities of the middle meningeal artery on angiography because external carotid angiography is not performed routinely in this setting. It is quite possible that middle meningeal artery lesions are common in this setting and also possible that they generally are benign in course but that the literature reflects a more aggressive course because it reflects lesions that came to attention as they became symptomatic.
Endovascular treatment of the middle meningeal artery pseudoaneurysm at the time of discovery was contemplated but not performed. Because the natural history of the incidentally discovered middle meningeal artery pseudoaneurysm was unknown and thus the benefit of the intervention unclear, we chose conservative management. A follow-up angiogram obtained after 1 month showed dramatic resolution of the middle meningeal artery pseudoaneurysm. This finding seems appropriate in retrospect, given the benign course of the lesion in this patient. This outcome suggests that at least some middle meningeal artery pseudoaneurysms may have the potential for a benign course, with spontaneous resolution, that conservative management should be considered, and that in those cases, the patient should be followed with conventional angiography.
There is only one case report in the literature, by Tsutsumi et al (12), in which middle meningeal artery pseudoaneurysm was managed conservatively, but this case was complicated by cavernous sinus fistula formation, which was treated with endovascular embolization. It is impossible to generalize our case to all cases of middle meningeal artery pseudoaneurysms, as the true natural history of traumatic and nontraumatic middle meningeal artery aneurysms remains to be defined.
References
- Received April 6, 2005.
- Accepted after revision April 21, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Republished: Intercostal artery pseudoaneurysm with spontaneous resolution in the setting of an artery of Adamkiewicz
- Intercostal artery pseudoaneurysm with spontaneous resolution in the setting of an artery of Adamkiewicz
- Intraparenchymal haematoma related to true middle meningeal artery aneurysm: a case report