
Abstract
Summary: We report a case of a patient who developed a remote dural arteriovenous fistula involving the left sigmoid sinus 4 months after successful transarterial embolization of a carotid cavernous fistula. This rare occurrence has been reported after transvenous embolization, but this represents the first case, to our knowledge, after transarterial coil embolization. We present our findings along with a brief review of the literature.
Dural arteriovenous fistulas (dAVFs) are commonly diagnosed secondary to intracranial hemorrhage or other symptoms such as pulsatile tinnitus. dAVFs in adults may be acquired lesions after trauma, venous outflow obstruction, or recanalization of a thrombosed sinus (1). These lesions typically involve the transverse, cavernous, and sigmoid sinuses (2). We report a case of a left-sided dAVF involving the sigmoid sinus that developed following bilateral transarterial embolization of a carotid cavernous fistula (CCF). The lesion was successfully treated by using transarterial particulate embolization.
Case Report
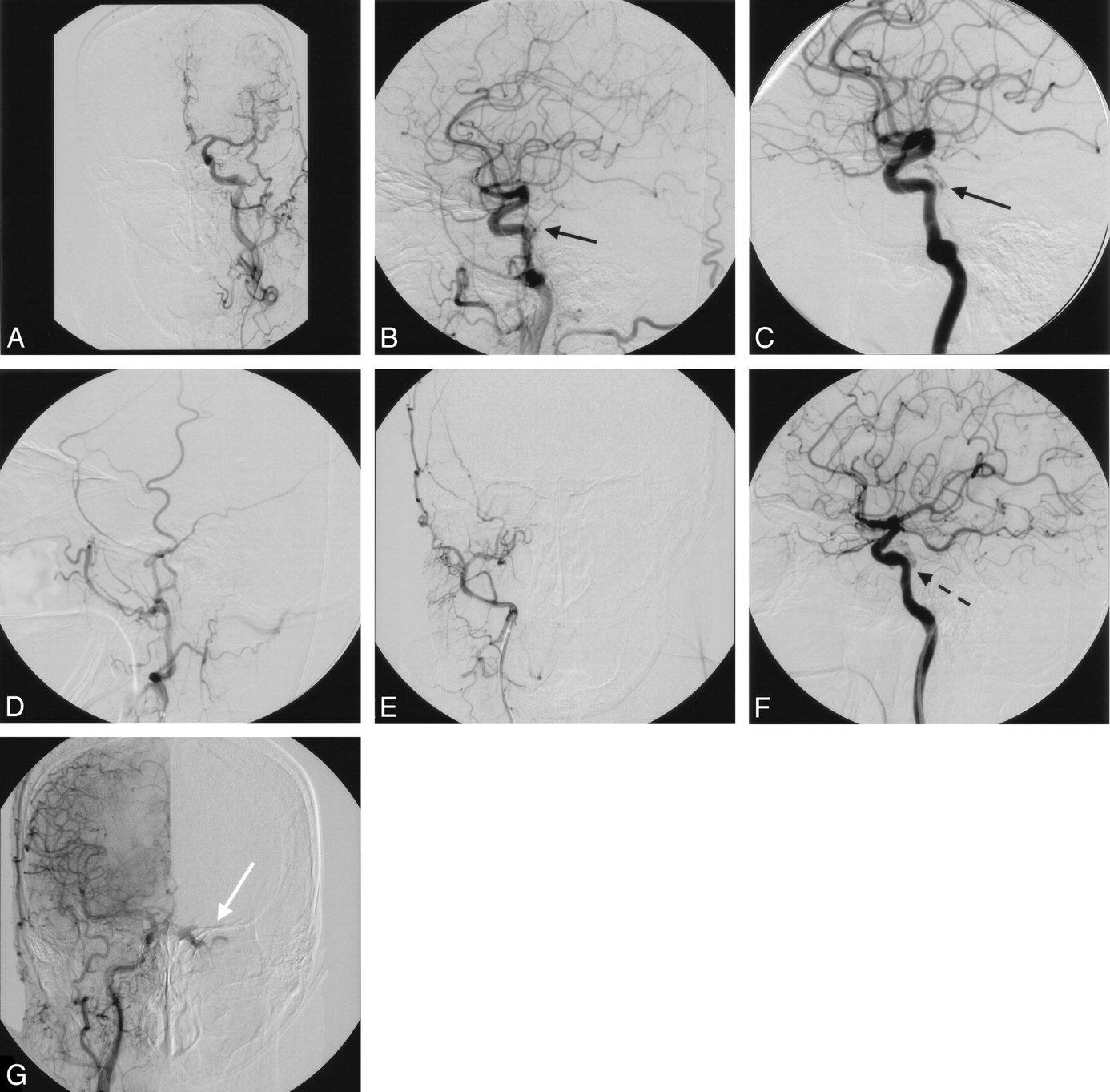
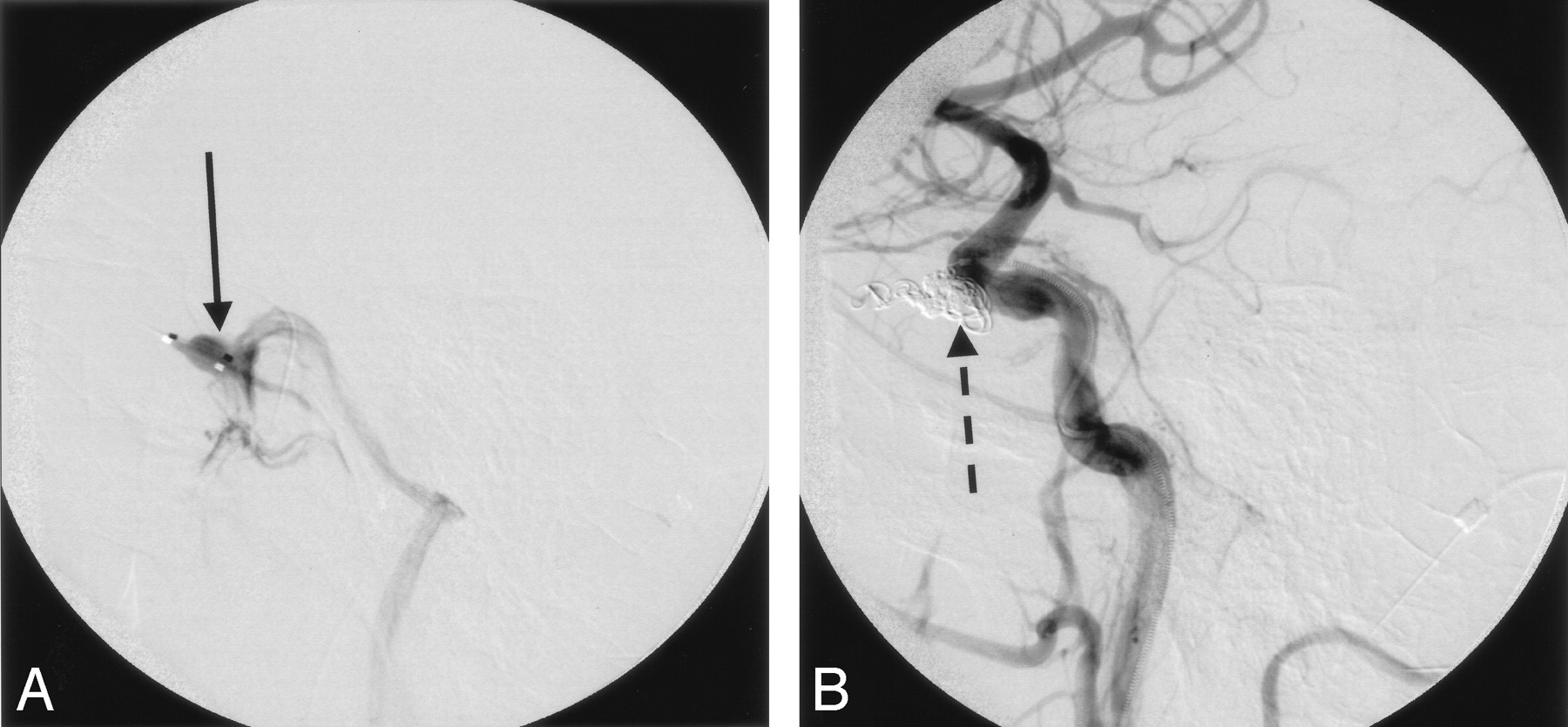
A 59-year-old woman presented with a CCF manifesting with severe proptosis, chemosis, and complete visual loss in the left eye. Cerebral angiography demonstrated supply to the fistula from the cavernous segments of both internal carotid arteries (ICAs; Fig 1A–G). A direct fistula (tear in the vessel) was noted involving the cavernous sinus on the right side. After the ICA tear was traversed with a RapidTransit microcatheter (Cordis Neurovascular, Miami, FL), a selective run demonstrated venous drainage into the left inferior petrosal sinus (Fig 2A). Platinum coils were deployed through the microcatheter across the fistula to occlude the opening (Fig 2B). A subsequent selective injection of the left ICA revealed an indirect CCF, with persistent dilation of the left superior ophthalmic vein (SOV). The ophthalmology team felt a cut down to access the SOV was not possible in this particular case and a left ICA balloon test occlusion was therefore performed with xenon CT to determine whether the vessel could be sacrificed. This procedure has been described elsewhere (3). The patient passed the balloon test with xenon CT, which showed normal blood flow to the left hemisphere. Platinum coils were deposited in the left ICA proximal to ophthalmic artery down to the cavernous segment to sacrifice the vessel. Postembolization, the fistula was completely obliterated. The patient’s chemosis and proptosis resolved during the next several days, but she remained blind in the left eye.

A and B, Anteroposterior and lateral projections of the left common carotid artery demonstrate an indirect dAVF involving the cavernous segment (solid black arrow). C, Selective left internal carotid artery injection on lateral projection further elucidates this finding (solid black arrow) with venous drainage to the left petrosal sinus. D and E, Anteroposterior and lateral projections of a selective right external carotid artery injection show no filling of the fistula from external carotid branches. F, Selective right internal carotid injection in a lateral projection reveals a tear in the vessel at the cavernous segment (dashed black arrow). G, Anteroposterior view of a right internal injection shows the presence of a markedly engorged left superior ophthalmic vein (white arrow) that is the cause of the patient’s symptoms.

A, Selective run through the direct fistula (black arrow) of the right cavernous sinus is shown with venous drainage to the petrosal and transverse sinuses. B, Postcoil embolization (dashed black arrow) reveals complete occlusion of the direct fistula.
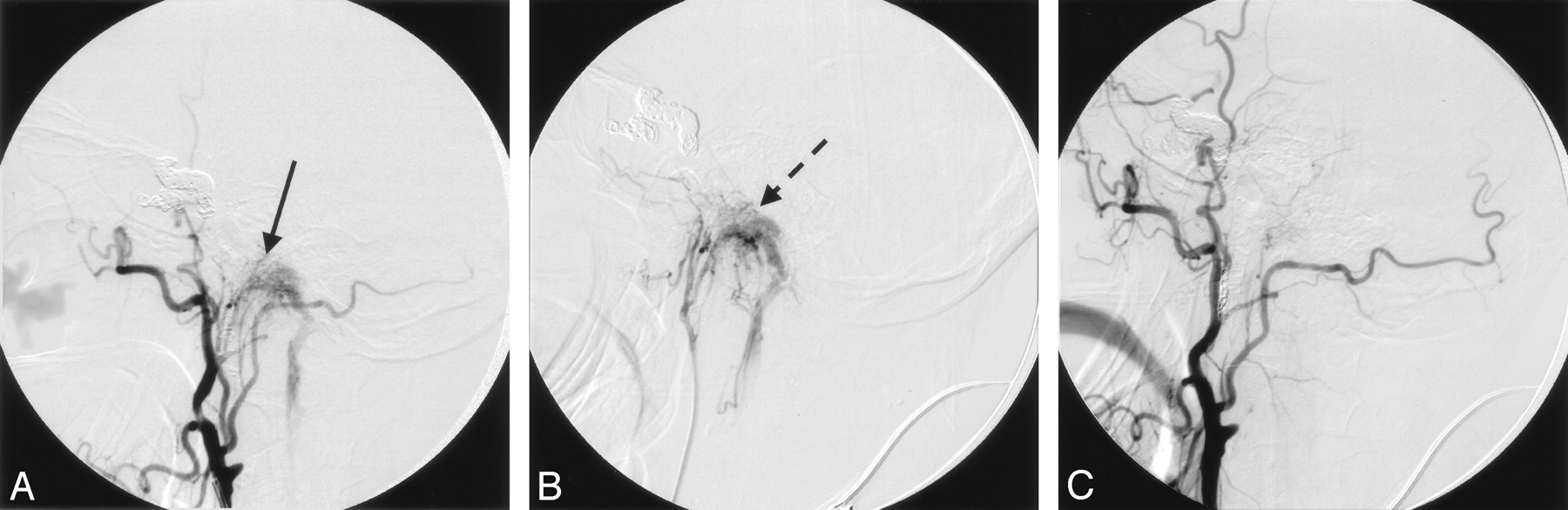
Four months after treatment of the CCF, the patient complained of left-sided tinnitus. Physical examination demonstrated an audible bruit over the left mastoid process. Cerebral angiography was repeated, which revealed continued obliteration of the CCF. An arteriogram of the left external carotid artery (ECA), however, revealed a left dAVF receiving supply from the left posterior auricular artery (PAA; Fig 3A). Following left PAA catheterization with a Simmons 2 diagnostic catheter (Merit Medical, South Jordan, UT), a selective run revealed this artery as the sole supply to the dAVF (Fig 3B). By using the Simmons 2 as a guide catheter, the dAVF was embolized by using 300–500-μ Embospheres (Biosphere Medical, Rockland, MA). The vessel was then sacrificed by using 3-mm to 2-mm fibered coils (Cook, Bloomington, IN). A final ECA arteriogram showed fistula occlusion (Fig 3C). All signs and symptoms resolved immediately. At 1-month follow-up, the patient noted continued resolution of the tinnitus and no audible bruit was appreciated on examination.

A, Selective left external carotid injection at 4-month follow-up reveals a dAVF (black arrow) fed by the posterior auricular artery with drainage into the sigmoid sinus. B, Superselective injection of the posterior auricular artery confirms the arterial supply to the dAVF (dashed black arrow). C, Postembolization run from the left external carotid artery confirms the obliteration of the fistula.
Discussion
dAVFs consist of direct connections between arteries and veins with rapid venous shunt surgery. Although it is felt that most such lesions in adults are acquired, they are rarely reported to develop following endovascular therapy of a remote and unrelated arteriovenous fistula. There have been 6 reports of remote symptomatic dAVFs noted after transvenous embolization of CCFs (Table 1; 4–9). It is interesting that, in all 6 patients, the remote fistula involved branches of the ECA draining into either the transverse sinus or jugular bulb as was seen in our patient.
Summary of case reports of de novo fistulas after transvenous embolization of a carotid cavernous fistula
Our case is unique in that a transarterial approach was solely used to treat the CCF and a de novo fistula appeared in a remote location. The etiology for the new dAVF is not clear, but several theories have been proposed. One theory is that manipulation of the venous anatomy with microcatheters may injure the veins, leading to sinus thrombosis, venous obstruction, and subsequent development of a dAVF. We used a transarterial approach, however, to treat the CCF, and thus this theory is unlikely in our patient. A second possibility is that the architecture of the dAVF was present before treatment of the CCF but was not visible at the time of angiography (8). As subsequent embolization altered the venous outflow to the transverse sinus, the occult fistula might have become clinically and angiographically apparent. A third possibility is that the initial embolization resulted in venous turbulence through the transverse sinus, thereby initiating thrombosis that lead to the development of an AVF as the thrombus was recanalized (7).
This report shows that remote dAVFs can develop after transarterial embolization and may shed light on the etiology of this occurrence. Although the etiology remains unclear for the development of this patient’s de novo fistula, it is important to recognize that such lesions can develop so that patients can be managed and followed appropriately following endovascular treatment of CCFs.
References
- Received February 14, 2005.
- Accepted after revision March 2, 2005.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}