
Abstract
Summary: We present five cases of intraparotid facial nerve schwannoma. In four of the five cases, tumors arising from the main facial nerve trunk were centered just below the skull base near the stylomastoid foramen and had a small cranial extension into the lower facial nerve canal. In three cases, each tumor had higher signal intensity around the periphery on T2-weighted images (target sign). These findings may be highly suggestive of an intraparotid facial nerve schwannoma.
Schwannoma is an ectodermal benign encapsulated tumor arising from Schwann cells. Schwannomas of the facial nerve arise from either the extratemporal or intratemporal course of this nerve (1). Most of these tumors are intratemporal, whereas 9% are located extracranially and usually appear as an asymptomatic parotid mass (2). Intraparotid facial nerve schwannomas account for only two of 142 parotid tumors (1). Hence, it is difficult to establish a correct preoperative diagnosis for facial nerve schwannoma (1). Although most patients with intraparotid schwannomas do not present with facial nerve palsy, it is important to suggest this diagnosis preoperatively because postoperative facial nerve paresis or palsy is common, and these patients can be better informed of this complication before surgery. We herein present our experiences with five cases of intraparotid facial nerve schwannoma and provide an analysis of MR imaging findings and histologic features.
Case Reports
Imaging Technique
Five patients, three women and two men, with pathologically proven facial nerve schwannomas underwent preoperative MR imaging studies on a 1.5-T unit (Signa Horizon, GE Medical Systems, Milwaukee, WI). Each examination consisted of axial T1-weighted (TR/TE, 300–650/9.3–18), axial T2-weighted (TR/TE, 3150–4000/90–120), and coronal gadolinium-enhanced imaging or coronal short tau inversion recovery (STIR) imaging (TR/TE/TI, 3216/36/165) with 5- to 7-mm section thickness. Both surgical and histopathological results were recorded.
Case 1
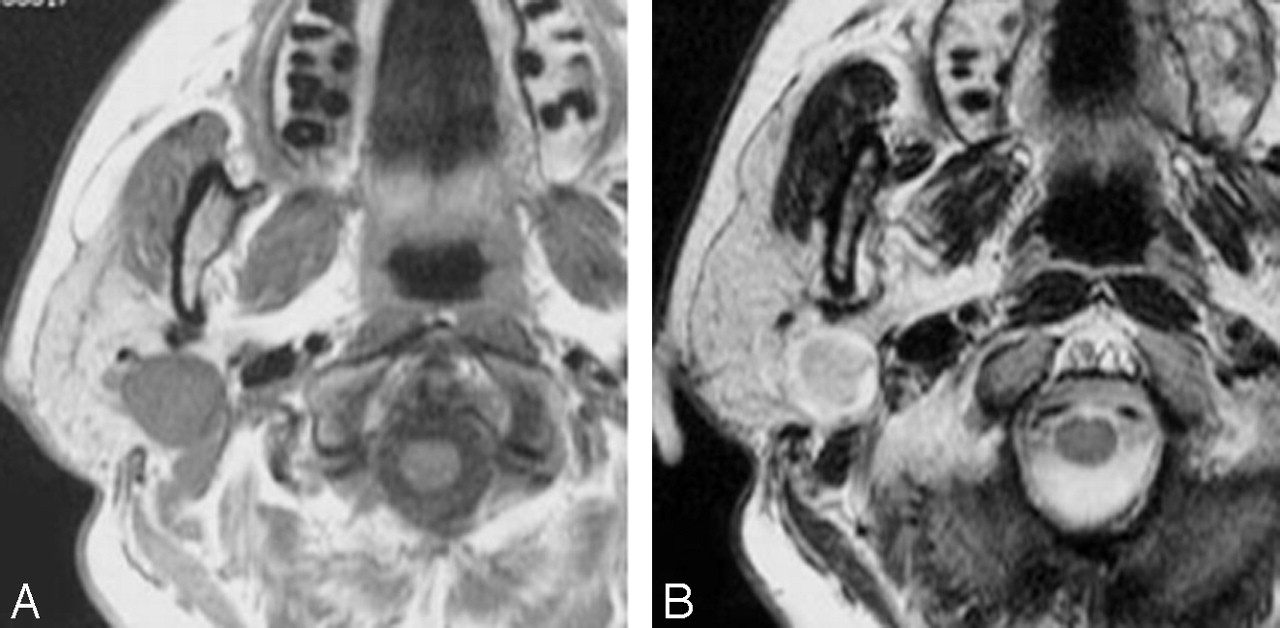
A 50-year-old woman had slight pain and swelling around her right ear in 1992. She did not wish to undergo surgery. Because the tumor enlarged slightly during the subsequent follow-up period, she consulted our otolaryngology department in 2000. MR imaging revealed a well-circumscribed lesion with a diameter of 1.8 cm in the right parotid gland. This tumor was situated directly caudal to the stylomastoid foramen and protruded into it. T1-weighted imaging showed the tumor to be isointense to muscle, and T2-weighted imaging revealed high signal intensity surrounding a central region of lower signal intensity (Fig 1A and B). During surgery, the tumor was found to be located in and adherent to the deep layer of the facial nerve trunk. Removing the tumor from the facial nerve trunk was somewhat difficult, but transecting the trunk was not necessary. The patient had slight facial palsy after the operation, but this gradually improved. The tumor was histopathologically diagnosed as Antoni A type schwannoma. This case of intraparotid facial nerve schwannoma arose from the main trunk of the facial nerve.

Case 1.
A, Axial T1-weighted image (spin-echo: TR/TE, 650/10.7) shows a low-signal-intensity well-defined mass in the right parotid gland.
B, Axial T2-weighted image (fast spin-echo: TR/TE, 3150/108) shows peripheral high signal intensity surrounding a central region of lower signal intensity.
Case 2
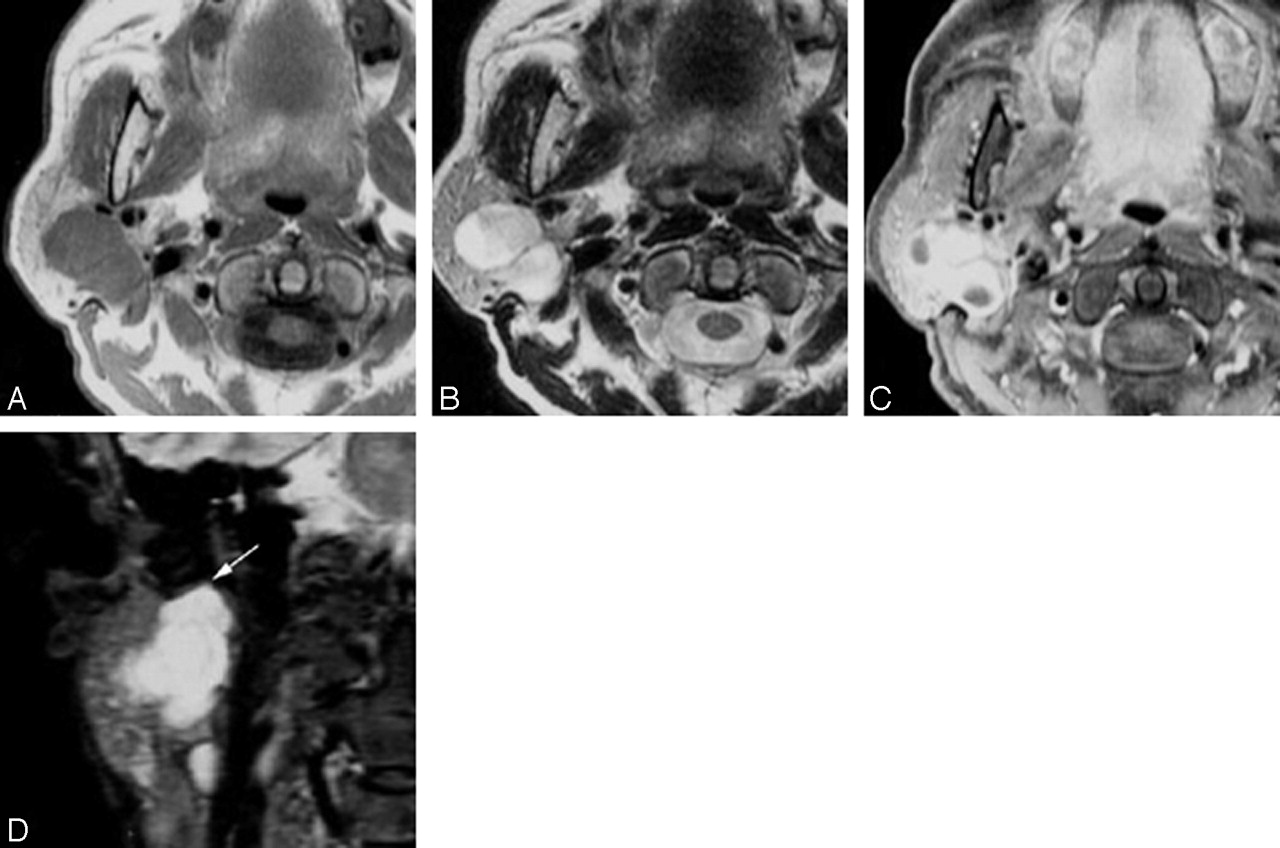
A 55-year-old woman presented to a local otolaryngologist with swelling in the right parotid gland in 2000. Aspiration biopsy cytology was conducted, and findings showed no malignancy. In 2001, the patient was admitted to our otolaryngology department for removal of the tumor. MR imaging showed a well-circumscribed lobulated lesion (2.0 × 1.5 cm) in the upper right parotid gland. The tumor was situated directly caudal to the stylomastoid foramen and protruded into it. T1-weighted imaging showed the lesion to be isointense to muscle, and T2-weighted and STIR images revealed heterogeneous hyperintensity and cystic degeneration. Gadolinium-enhanced T1-weighted imaging showed an area of increased density (Fig 2A-D). During surgery, we observed that the tumor was adherent to the deep layer of the facial nerve trunk, and the central side of the trunk was transected and reconstructed with the great auricular and transverse cervical nerves. The patient had postoperative ipsilateral facial palsy. The tumor was histopathologically diagnosed as Antoni A4 type schwannoma. This case of intraparotid facial nerve schwannoma arose from the main trunk of the facial nerve.

Case 2. A, Axial T1-weighted image (spin-echo: TR/TE, 650/9.3) shows a lobulated mass in the right parotid gland, with a low-signal-intensity well-defined mass in the right parotid gland.
B, Axial T2-weighted image (fast spin-echo: TR/TE, 3150/108) shows a heterogeneous hyperintense mass.
C, Axial gadolinium-enhanced T1-weighted image (spin echo; TR/TE, 650/9.3) shows a mass in the right parotid gland with heterogeneous enhancement.
D, Coronal STIR image (TR/TE/TI, 3216/36/165) shows a hyperintense mass in the right parotid gland. The tumor is situated directly caudal to the stylomastoid foramen and protrudes into it (arrow).
Case 3
In 1995, a general practitioner diagnosed a right parotid tumor in a 61-year-old man. The patient did not wish to undergo surgery. Because the tumor enlarged slightly during the subsequent follow-up period, the patient was referred to our institution, and we recommended surgery in 1999. No preoperative facial palsy was evident. MR images showed two well-circumscribed lesions in the upper right parotid gland, each of which measured 2 cm in diameter. T1-weighted imaging revealed the lesions to be isointense to muscle, and T2-weighted imaging showed high signal intensity area surrounding a central region of lower signal intensity. Observations made during surgery revealed that the tumors extended from the superficial to the deep lobes of the parotid gland and were surrounded by the zygomatic and temporal branches of the facial nerve. The facial nerve trunk was preserved, and the tumors were extirpated and histopathologically diagnosed as schwannomas. The patient exhibited no postoperative facial palsy.
Case 4
In 2001, a 51-year-old man had swelling below the right ear and a distortion of the right lower lip. MR imaging showed a well-circumscribed lesion with a diameter of 1.7 cm in the upper right parotid gland. The tumor was situated directly caudal to the stylomastoid foramen and protruded into it. T1-weighted imaging showed the mass to be isointense to muscle, and T2-weighted imaging revealed a nonuniform hyperintense lesion with cystic degeneration. Gadolinium-enhanced T1-weighted imaging showed an area of increased density. Open biopsy was attempted, but the facial nerve trunk could not be identified because of the large tumor mass. Electrical stimulation of the tumor elicited contraction of the right side of the face. Histologic diagnosis was schwannoma. This case of intraparotid facial nerve schwannoma arose from the main trunk of the facial nerve.
Case 5
In 1998, a 70-year-old woman found a swelling in her right parotid gland. In 1999, she was admitted to our otolaryngology department for removal of the tumor.
MR imaging showed a well-circumscribed lesion with a diameter of 2.8 cm in the upper right parotid gland. The tumor was situated directly caudal to the stylomastoid foramen and protruded into it. T1-weighted imaging showed the lesion as isointense to muscle and T2-weighted imaging revealed almost uniform hyperintensity. Gadolinium-enhanced T1-weighted imaging showed an area of increased density.
Because the cystic tumor had developed along the direction of the facial nerve, it was enucleated from the facial trunk. After surgery, the patient exhibited right-sided facial palsy. The tumor was histopathologically diagnosed as schwannoma with partial myxoid degeneration (Antoni B type). This case of intraparotid facial nerve schwannoma arose from the main trunk of the facial nerve.
Discussion
Schwannomas are benign tumors that arise from the nerve sheath. Preoperative diagnosis of this tumor in the parotid gland is generally difficult because of the low frequency of the disease and few typical signs associated with it. The estimated frequency of parotid tumors originating in the facial nerve ranges from 0.2% to 1.5% (3). In addition, preoperative diagnosis of a parotid tumor as a schwannoma is difficult in the absence of facial nerve dysfunction (4), which is an uncommon feature when the tumor arises from the facial nerve trunk. In this study, four of the five cases presented only as a parotid mass without facial nerve dysfunction.
This study was undertaken to analyze radiologic findings of intratemporal and extratemporal schwannomas (ETS) (4). We presented five cases of intraparotid facial nerve schwannoma representing ETS and retrospectively analyzed the MR imaging findings. Four of the five cases of intraparotid facial nerve schwannomas arose from the main trunk of the facial nerve. Findings in these four cases showed that the main facial nerve trunk was centered just below the skull base near the stylomastoid foramen and had a small cranial extension into the lower facial nerve canal. Chung et al (4) described cases of ETS that were located in the posterolateral to the retromandibular vein and extended toward the stylomastoid foramen, consistent with the characteristic position of the facial nerve.
Martin et al (5) described MR imaging findings in four facial nerve schwannomas. All tumors were slightly heterogeneous lesions that were isointense to brain on T1- and T2-weighted images. In the present study, all tumors were well defined, and signal intensities were isointense to muscle on T1-weighted images and hyperintense to muscle on T2-weighted images. Three of the five facial nerve schwannomas exhibited a target sign characterized by increased peripheral signal intensity and decreased central signal intensity on T2-weighted images. Previous authors have described a target sign of neurofibroma that is almost pathognomonic of that lesion (6). This feature suggests neurogenic neoplasm, although it can also be seen in schwannomas and malignant peripheral nerve sheath tumors (PNST). It is common in plexiform neurofibromas and less frequent in malignant PNST (7). In schwannoma, the target sign corresponds to more cellular Antoni A regions centrally and to more myxoid Antoni B regions peripherally (7).
In case 3, multiple schwannomas arose from side branches of the peripheral facial nerve. The pathogenesis of multiple facial nerve schwannomas is not clearly understood (3). However, Chiang et al (3) presented a case of multiple intraparotid facial nerve schwannomas, and their finding of a developing schwannoma forming from a grossly normal nerve sheath may support the multicentric hypothesis of multiple facial nerve schwannoma development.
Pleomorphic adenomas are the most common tumors of the parotid gland, typically exhibiting high signal intensity on T2-weighted images, lack of homogeneity, and sharp demarcation from the adjacent parotid gland (8). These findings are similar to those of intraparotid facial nerve schwannoma; however, if the tumor has a growth toward the facial canal, facial nerve schwannoma may be reasonably suspected.
Adenoid cystic carcinoma is known for its tendency for perineural invasion. In these malignant tumors invading the facial canal, MR imaging can show the extent of nerve involvement (9). However, continuity between the parotid mass and the well-delineated enlargement of the facial nerve seems to exclude this method of diagnosis (8).
Conclusion
Preoperative diagnosis of intraparotid facial nerve schwannoma is difficult. However, the present study suggests that the presence of a target sign and a growth toward the facial canal are distinguishing features of this tumor that are very useful in preoperative diagnosis.
References
- Received March 9, 2004.
- Accepted after revision August 6, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.