
Abstract
Summary: This report outlines the diagnosis and endovascular management of a rare intracanalicular ophthalmic aneurysm in a patient presenting with progressive visual loss.
Carotid-ophthalmic aneurysms account for 11% of all intracranial aneurysms. True aneurysms of the ophthalmic artery are extremely rare and most often arise at the origin of this artery. A review of the literature revealed several cases of ophthalmic artery aneurysms, but, to our knowledge, an aneurysm of the intracanalicular segment has not been described to date.
Case Reports
In September 2003, a 53-year-old white man presented with a 3-week history of painless, nonprogressive visual loss in the left eye. He had no relevant medical history, specifically no history of peripheral or cerebrovascular disease.
Visual acuity was decreased in the left eye, with evidence of optic nerve compression. Follow-up in February 2004 revealed further decreased left visual acuity to count fingers at 10 cm, with inability to see any color plates.
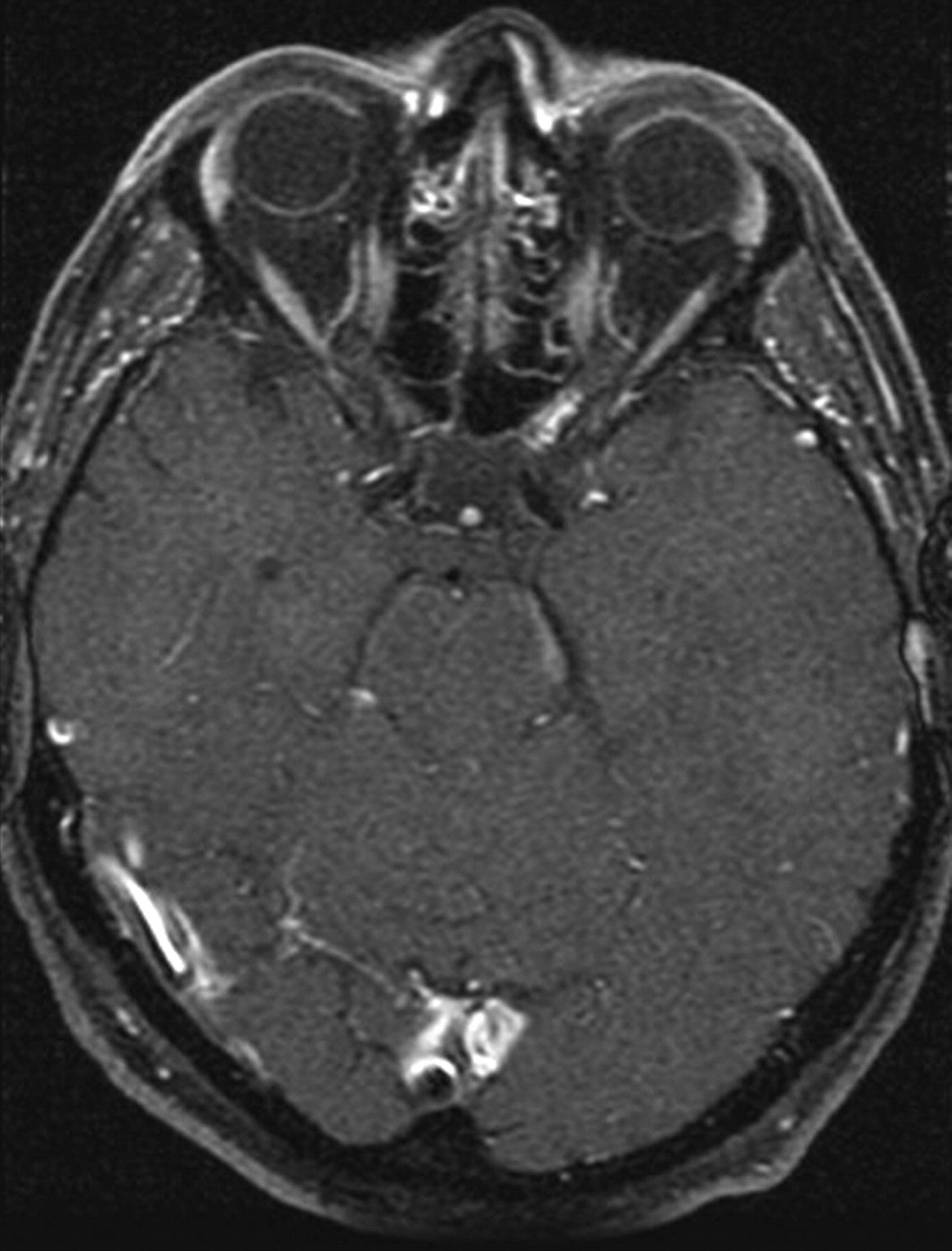
CT examination of the orbits using intravenous contrast material, performed in October 2003, revealed uniform enlargement of the left optic nerve at the orbital apex and intracanalicular portion. MR imaging examination with gadolinium in December 2003 showed a 6-mm linear enhancing region in the intracanalicular left optic nerve (Fig 1).

MR imaging with gadolinium shows linear enhancement in the region of the intracanalicular left optic nerve.
CT angiography was performed in January 2004. An area of enhancement was seen within the left optic canal, extending for a length of 7–8 mm, a width of 4 mm, and a height of 3 mm, appearing contiguous with the ophthalmic artery (Fig 2A, -B). Cerebral angiography was performed in February 2004 and revealed a fusiform irregular aneurysm in the canalicular segment of the left ophthalmic artery, measuring 3–4 mm in diameter with a length of 10 mm, extending throughout the optic canal; its origin was near or at the origin of the ophthalmic artery from the left internal carotid artery (Fig 3). The distal ophthalmic artery appeared normal. No other aneurysms were seen.

A,B, CT angiograms show enhancement within the left optic canal, appearing contiguous with the ophthalmic artery.

Cerebral angiogram reveals fusiform aneurysm of intracanalicular left ophthalmic artery. Origin of aneurysm is at or near the origin of the ophthalmic artery from the left internal carotid artery; the distal ophthalmic artery is normal.
The patient was referred for neurosurgical consultation. Because of the significant compression of the left optic nerve, decompression of the optic canal with proximal clip ligation of the aneurysm was thought to be the initial preferred approach. To assure adequate collateral perfusion of the retina, we performed test occlusion. A left carotid occlusion tolerance test was performed using a microballoon catheter (HyperGlide, 4 × 15 mm, Micro Therapeutics, Inc., Irvine, CA), which was inflated in the internal carotid artery just proximal to the ophthalmic artery origin, following systemic anticoagulation. A common carotid angiogram with the balloon inflated demonstrated complete occlusion of the internal carotid artery and retrograde perfusion of the left ophthalmic artery through the external carotid artery collaterals, back through the aneurysm at the ophthalmic artery origin to the supraclinoid carotid segment of the internal carotid artery. There was no change in the patient’s neurologic status or vision throughout the procedure, indicating that proximal occlusion of the left ophthalmic artery would be safely tolerated.
Left frontotemporal craniotomy was performed in April 2004. The clinoid was removed to unroof the optic canal throughout the length of the optic nerve to the posterior aspect of the orbit, to provide exposure for attempted clipping. Unfortunately, the aneurysm was not amenable to surgical clipping because of adherence to the inferior aspect of the optic nerve.
The aneurysm was subsequently treated using an endovascular approach. With the patient sedated by anesthesia and with systemic intravenous anticoagulation, we placed a 6F sheath via a right femoral puncture and advanced a 6F guide catheter into the left cervical internal carotid artery. Injections revealed no change in the fusiform left ophthalmic artery aneurysm, starting in the subarachnoid space and extending anteriorly through the optic canal. Under road mapping, an SL 10 microcatheter (Excelsior, Boston Scientific, Natick, MA) was placed coaxially over a 0.014 microwire (Transend, Boston Scientific) into the proximal aspect of the left ophthalmic artery, just proximal to an abrupt angulation of the artery (Fig 4). The ophthalmic artery was then occluded at its origin from the internal carotid artery with one 2 × 4 mm coil (GDC UltraSoft, Boston Scientific) (Fig 5). A left external carotid artery injection showed a choroidal blush, and the ophthalmic artery was visualized, confirming continued collateral circulation. General anesthesia was reversed after all catheters and sheaths were removed.

Excelsior SL10 microcatheter (Boston Scientific, Natick, MA) was placed coaxially over the Transend 0.014 microwire (Boston Scientific) into the proximal left ophthalmic artery, just proximal to an abrupt angulation.

Proximal ophthalmic artery was occluded with a GDC UltraSoft 2 × 4 mm coil (Boston Scientific) with effective occlusion of the ophthalmic artery at its origin from the internal carotid artery.
The patient had transient decreased vision in his left eye postembolization so that only light perception was possible. Several hours later he could detect hand motion; thus, he returned to his preembolization visual status. At last follow-up, August 2004, significant visual improvement was noted.
Discussion
Intracranial aneurysms occur in 0.5% to 1% of the population. Intracranial vascular sites subject to aneurysm formation include the following: anterior communicating/anterior cerebral arteries (39%), internal carotid artery (including posterior communicating and ophthalmic segment) (30%), middle cerebral artery (22%), and vertebrobasilar artery (8%) (1). Ophthalmic segment carotid artery aneurysms (carotid-ophthalmic aneurysms) typically arise along the anteromedial wall of the first bend of the internal carotid artery, just distal to the origin of the ophthalmic artery, and project either dorsally or dorsomedially toward the optic nerve. Carotid-ophthalmic aneurysms account for 11% of all intracranial aneurysms.
The ophthalmic segment of the internal carotid artery (that portion of the internal carotid that lies between the ophthalmic artery and posterior communicating artery) gives rise to 2 major branches: the ophthalmic artery and the superior hypophyseal artery. In 80%–90% of patients, the ophthalmic artery originates immediately after the internal carotid artery emerges from the cavernous sinus, just below the anterior clinoid process, immediately beneath the optic nerve, and is hence intradural (2). The ophthalmic artery enters the orbit inferolateral to the optic nerve and then usually crosses and runs on the superomedial side of the nerve, before terminating as the retinal vascular system and the ciliary vascular system. The ophthalmic artery is divided into intracranial, intracanalicular, and intraorbital segments.
Anatomic variations in ophthalmic artery origin are important for consideration of embolization and carotid surgery. The artery can originate from the middle meningeal artery (meningolacrimal artery), or branches of the meningeal artery may connect with the ophthalmic artery. External carotid-ophthalmic artery anastomoses are numerous and include superficial temporal artery branches, internal maxillary branches, and facial artery branches. Branch anastomoses result in a network of collateral blood supply that is protective should the internal carotid artery occlude.
True aneurysms of the ophthalmic artery are extremely rare and most often arise at the origin of the ophthalmic artery. Most commonly, ophthalmic artery aneurysms present with progressive visual disturbance or exophthalmos, although they may be asymptomatic (3). Intracanalicular segment aneurysms would presumably be more likely to cause optic nerve conduction disorders.
Isolated case reports discuss intraorbital ophthalmic artery aneurysms. Most recently, Ernemann et al (4) reported a case of intraorbital ophthalmic artery aneurysm causing apical compression. Dehdashti et al (5) reported an asymptomatic case of intraorbital ophthalmic artery aneurysm found incidentally with a basilar tip aneurysm. Yanaka et al (6) recently described an ophthalmic artery trunk aneurysm and performed a literature review. They found only 14 case reports of peripheral ophthalmic artery aneurysms; 5 involved the intracranial portion of the ophthalmic artery, and the remainder involved the intraorbital portion of the ophthalmic artery (7, 8). We were unable to find any reports of a fusiform intracanalicular ophthalmic artery aneurysm or its management.
Ophthalmic artery aneurysms include a subset with a relatively low rate of rupture. In our case, significant progressive deterioration in vision motivated the decision to treat, which is a much more difficult one for asymptomatic lesions. Treatment was undertaken in this case to preserve the remaining vision, decrease the risk of rupture, prevent further aneurysm growth, and release the optic nerve compression in the hope of achieving some nerve function recovery. The patient’s vision initially worsened slightly but quickly returned to baseline. A possible reason for deterioration of vision was transient worsening of optic nerve compression or edema due to microcatheter manipulation and coil placement in an aneurysm adherent to the nerve that had been chronically compressed or aneurysmal swelling during thrombosis due to coil occlusion. The rapid recovery to baseline and subsequent improvement in vision attest to the adequacy of retinal perfusion despite proximal ophthalmic artery occlusion.
- Received October 6, 2004.
- Accepted after revision November 15, 2004.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}