
Abstract
Summary: Spinal artery aneurysms are usually found with arteriovenous malformations or other entities that increase hemodynamic stress. Isolated spinal artery aneurysms are rare. Four patients who presented with the acute onset of lower back pain underwent MR imaging, which revealed spinal subarachnoid hemorrhage. In all patients, work-up yielded a diagnosis of isolated spinal aneurysm, and operative treatment was successful. In the appropriate clinical setting, spinal aneurysm should be considered as a possible cause of spinal subarachnoid hemorrhage.
Other than trauma, the most common cause of intracranial subarachnoid hemorrhage is rupture of a cerebral aneurysm. However, isolated spinal artery aneurysms are rare, and few cases have been reported (1, 2). Spinal artery aneurysms associated with arteriovenous malformations are more numerous (3). Spinal artery aneurysms may also be associated with other entities that increase hemodynamic stress, such as aortic coarctation or bilateral vertebral occlusion in cases in which the spinal artery circulation is recruited as the collateral pathway (4).
Case Reports
We report 4 patients who presented with the acute onset of lower back pain. Their evaluation included MR imaging and conventional spinal angiography. In all 4 patients, spinal subarachnoid hemorrhage related to a spinal aneurysm was diagnosed.
Subsequently, they all underwent successful surgical treatment.
Case 1
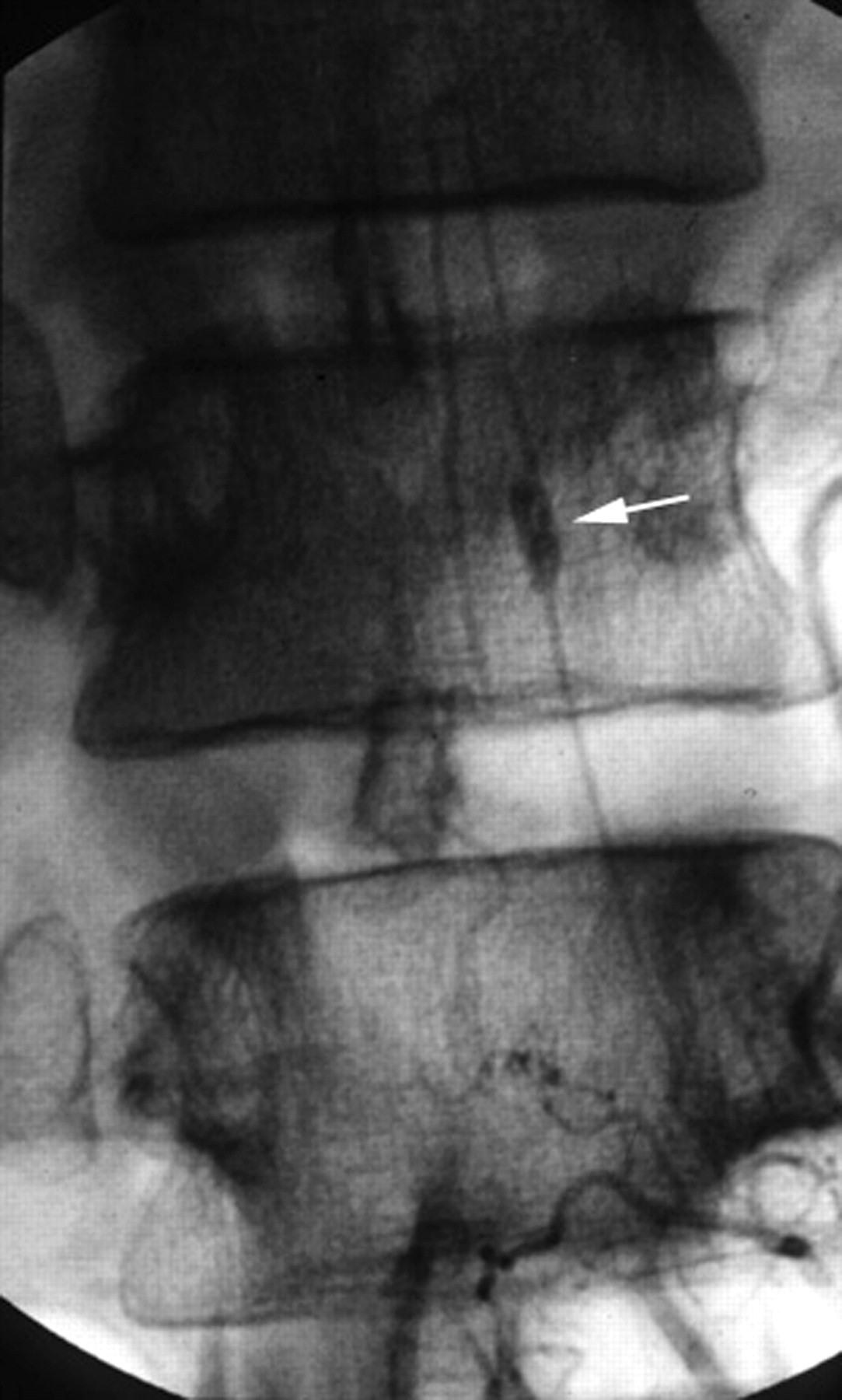
A 30-year-old man presented with the acute onset of back pain and lower extremity weakness and paresthesias. On examination, he was neurologically intact with minimal weakness in the lower extremities. MR imaging showed a flow void and subdural hemorrhage in the middle-to-lower thoracic canal. Spinal angiography showed a fusiform aneurysm suggestive of a dissecting aneurysm arising from the artery of Adamkiewicz (Fig 1). The patient underwent a transthoracic partial T11 vertebrectomy with muslin wrapping (5) of the dissecting aneurysm. His baseline neurologic status was maintained without obvious neurologic deficits.

Selective angiogram of the left artery of Adamkiewicz at T11 showing a fusiform aneurysm (arrow). Reprinted with permission from Lippincott Williams & Wilkins.
Case 2
Four days before his evaluation, a 69-year-old man with a history of hypertension, stroke, and right carotid endarterectomy experienced the sudden onset of excruciating lower back pain that radiated to both legs. The pain was worse on his left than on his right side. A lumbar puncture was positive for spinal subarachnoid hemorrhage. On admission, MR imaging showed spinal subarachnoid hemorrhage in the left side of the spinal canal. The spinal cord was slightly displaced to the right. At spinal angiography, injection of the left L1 spinal artery showed 2 aneurysms. The larger aneurysm was located more superiorly than the smaller one (Fig 2A, -B). The anteroposterior projection showed the large aneurysm to the left of midline, involving a radicular artery. The second smaller aneurysm, which was located more inferiorly, involved the same vessel.

(A) Selective angiogram of the left L1 spinal artery showing 2 aneurysms (arrows). (B) Additional view of left L1 spinal artery injection showing 2 aneurysms (arrows).
The patient underwent a T12-L2 laminoplasty, and the dissecting aneurysm was dissected off the L1 radicular branch. The appearance of the lesion was consistent with a dissecting aneurysm, and the diagnosis was confirmed by histopathologic analysis. Postoperative spinal angiography showed no residual aneurysm. At discharge, the patient was oriented and walked with minimal assistance.
Case 3
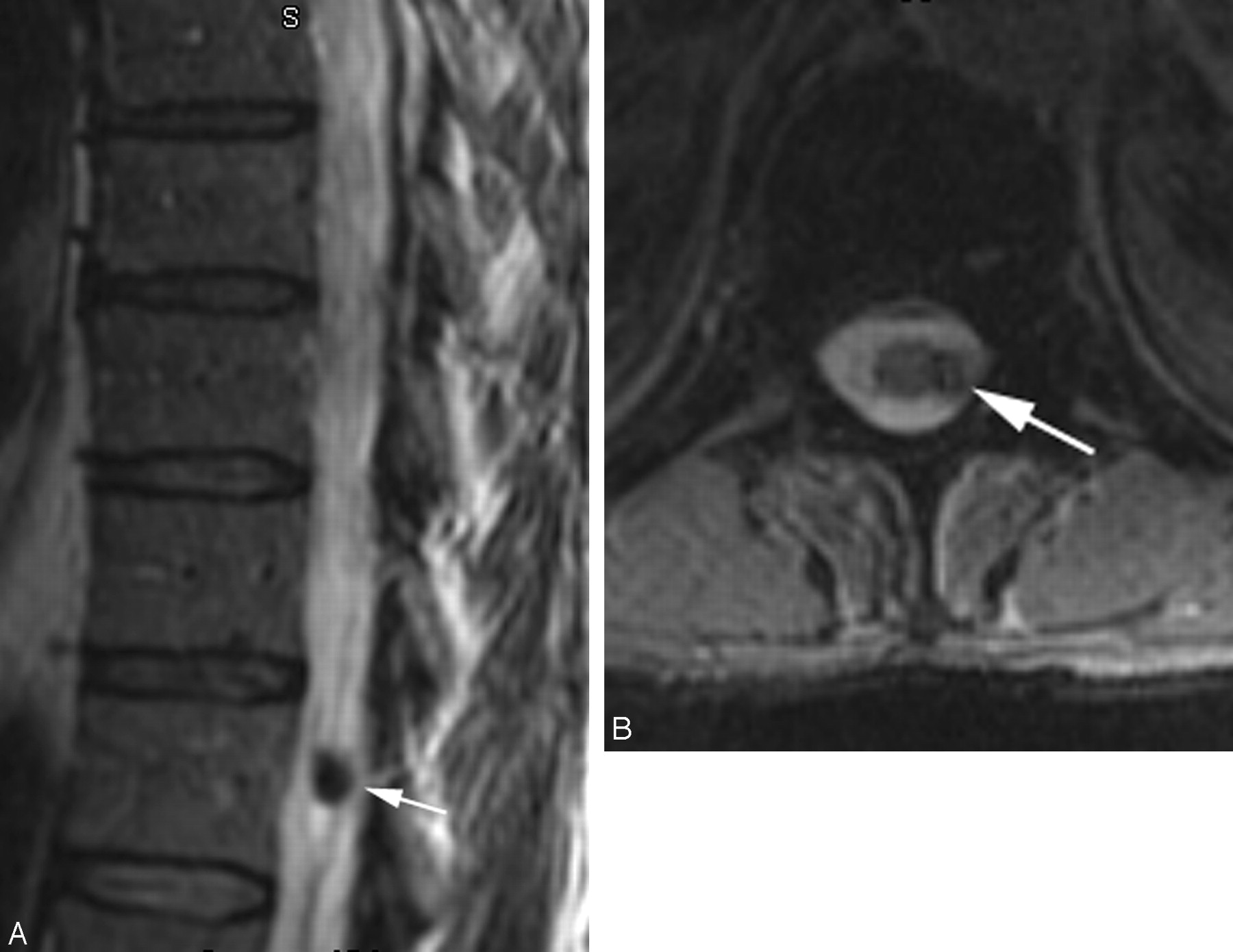
A 54-year-old man sought treatment for lower back pain that radiated to both hips and lower extremities. He had no significant medical or surgical history. MR imaging performed at an outside institution showed a large amount of spinal subarachnoid hemorrhage at the thoracolumbar junction level (Fig 3A, -B), but no definite focal lesion was noted. Eleven days later, spinal angiography performed with injections at T7 through L4 showed no evidence of a spinal arteriovenous malformation or dural arteriovenous fistula. MR imaging performed at our institution 1 day after angiography showed a small rounded focal area of signal-intensity abnormality contiguous with the left side of the conus medullaris at T12 (Fig 4A, -B). Loss of signal intensity was evident on T2-weighted fast spin-echo and gradient-echo sequences without enhancement. On the patient’s initial study performed at the outside institution, this focal area had been obscured by a large amount of hemorrhage. Exophytic cavernous malformation, myxopapillary ependymoma, and hemorrhagic metastasis were considered in the differential diagnosis.

(A) Initial sagittal T2-weighted MR image showing a large amount of subarachnoid hemorrhage (arrows) at the thoracolumbar junction but no definite focal lesion. (B) Initial axial T2-weighted MR images showing a large amount of subarachnoid hemorrhage (arrows).

(A) Sagittal and (B) axial T2-weighted images obtained 11 days after the patient’s first MR imaging showing a more focal lesion adjacent to the conus medullaris at T12 (arrow).
The patient underwent surgery. When the dura was opened, spinal subarachnoid hemorrhage and thickening of the arachnoid were visible. A thrombosed aneurysm compressing the spinal cord on the left side at T12 was discovered. The afferent vessel was thrombosed. The efferent vessel was minimally open and bleeding. The thrombosed aneurysm was excised, and the afferent vessel was clipped. The pathologic diagnosis was a T12 dissecting aneurysm with organizing blood clot and proliferation of fibroblasts. The remainder of the patient’s hospital stay was uneventful with no neurologic complications.
Case 4
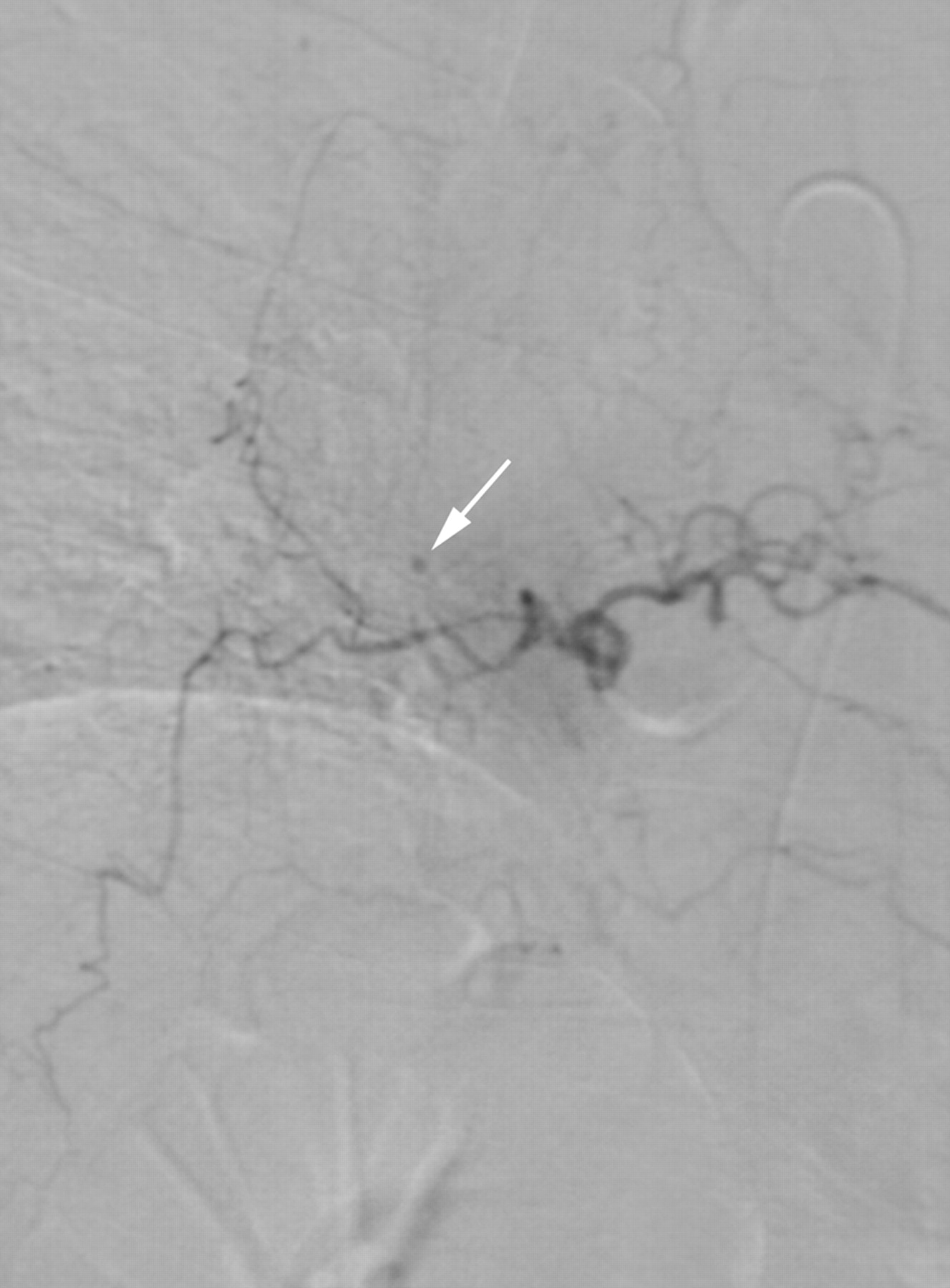
A 73-year-old man presented with left lower extremity weakness that worsened for 2 weeks. On evaluation at our institution, he had nuchal rigidity and questionable meningitis. CT of the head showed spinal subarachnoid hemorrhage. A lumbar puncture was positive for this entity. MR imaging of the brain showed questionable bihemispheric spinal subarachnoid hemorrhage and evidence of an old subinsular infarct on the right. The findings of cerebral angiography were negative. MR imaging of the spine performed at an outside institution showed evidence of hemorrhage and what was thought to be a spinal mass or vascular lesion compressing the spinal cord. An angiographic injection of the left T6 spinal artery, also performed at an outside institution, showed an aneurysm involving the radicular branch (Fig 5). The patient was referred to our institution for surgery.

Selective angiographic injection of the left T6 spinal artery showing an aneurysm (arrow) involving the radicular branch.
The patient underwent a T5-T7 laminoplasty and microsurgical reconstruction of a left T6-T7 ruptured radicular artery aneurysm with 10-0 nylon and muslin. His hospital stay was uncomplicated, and he was discharged on postoperative day 5.
Discussion
Spinal artery aneurysms that are not associated with other entities such as arteriovenous malformations, aortic coarctation, or vasculitides are rare. Few isolated spinal artery aneurysms have been reported. Spinal artery aneurysms usually tend to be associated with an arteriovenous malformation, and these patients typically become symptomatic with back pain, with or without a radicular component, spinal subarachnoid hemorrhage, or progressive paraparesis (6).
In 1981, Vincent (1) reported the first angiographically confirmed rupture of an anterior spinal artery aneurysm. Before his report, there were only 5 documented cases of ruptured spinal artery aneurysm in the literature (7, 8). By 1993, Rengachary et al (2) noted that 17 cases of isolated spinal artery aneurysm had been reported. Since then, there have been very few reported cases of ruptured isolated spinal artery aneurysm (9, 10).
In most cases, intracranial aneurysms that rupture are saccular or berry aneurysms occurring at bifurcation points along the intracranial arterial tree. These aneurysms tend to be found in patients with a connective tissue disease such as Ehlers-Danlos syndrome or fibromuscular dysplasia. Patients with polycystic kidney disease have a high incidence of aneurysms, as do patients with family members who have had aneurysms (11).
Aneurysms form in response to high blood flow within a vessel. This phenomenon would account for aneurysms that develop along feeding vessels to an arteriovenous malformation. This mechanism would also explain the formation of an aneurysm in the region of the anterior communicating artery in patients with carotid occlusions associated with resultant collateral blood flow through the anterior communicating artery to the contralateral cerebral circulation. It would also explain a higher rate of aneurysms in the spinal circulation that have been reported in association with aortic coarctation related to the recruitment of collateral circulation from the spinal vascular system (12).
The angiographic appearance of mycotic and oncotic aneurysms is similar. Both tend to be fusiform along the course of the artery rather than occurring at branch points. Mycotic aneurysms are caused by infectious or inflammatory processes. Oncotic aneurysms are commonly associated with atrial myxoma.
Traumatic pseudoaneurysms may be caused by a penetrating injury or a closed head injury with an impact that forces the artery in contact with dural structures such as the falx cerebri, tentorium, or cranial fracture fragments that tear the wall of the artery.
In 3 of our patients, the spinal artery aneurysms were fusiform dilations that occurred along the course of the artery and were found to be dissecting aneurysms at surgery. Two of these 3 were excised and were histopathologically confirmed to be dissecting aneurysms. The 2 that were not confirmed by histopathology were not resected and were wrapped or reconstructed at surgery. None of our patients had evidence of other aneurysms, obvious connective tissue disorders, obvious trauma, infections, or neoplastic processes. On the basis of our experience, we found that these spinal artery aneurysms tend to be dissecting aneurysms that occur along the intradural portion of the radicular artery as it courses to the spinal cord.
In our 4 patients, MR imaging showed evidence of spinal subarachnoid hemorrhage. Conventional spinal angiography showed evidence of a spinal artery aneurysm in 3 of the 4 patients. In the fourth patient, a thrombosed spinal artery aneurysm was found at surgery, despite negative findings on an angiographic study.
Our 4 patients underwent operative treatment, and all had successful outcomes.
We propose that the diagnostic images of patients who experience the sudden onset of back pain, lower extremity radiculopathy, or both should be searched for a potential source of hemorrhage when imaging findings indicate the presence of spinal subarachnoid hemorrhage. If a large amount of hemorrhage is present that may obscure its source, short-term follow-up MR imaging (within 1–2 weeks) should be considered. For focal lesions, aneurysms should be included in the differential diagnosis, and angiography should be performed. If the findings of angiography are negative, thrombosed aneurysm should still be considered in the differential diagnosis.
In summary, 4 patients who presented to our institution were correctly diagnosed and treated for isolated spinal artery aneurysms. We conclude that when spinal subarachnoid hemorrhage is present in the appropriate clinical setting, a spinal aneurysm should be considered as a possible treatable cause.
References
- Received September 21, 2004.
- Accepted after revision December 24, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Reasoning: A 36-Year-Old Woman Presenting With Headache Postpartum
- Republished: Ruptured aneurysm of the artery of Adamkiewicz: is conservative management the standard of treatment in the current era?
- Spinal artery aneurysms: clinical presentation, radiological findings and outcome
- Ruptured aneurysm of the artery of Adamkiewicz: is conservative management the standard of treatment in the current era?
- Lateral sacral artery aneurysm of the lumbar spine: hemorrhage resulting in cauda equina syndrome