
Article Figures & Data
Figures
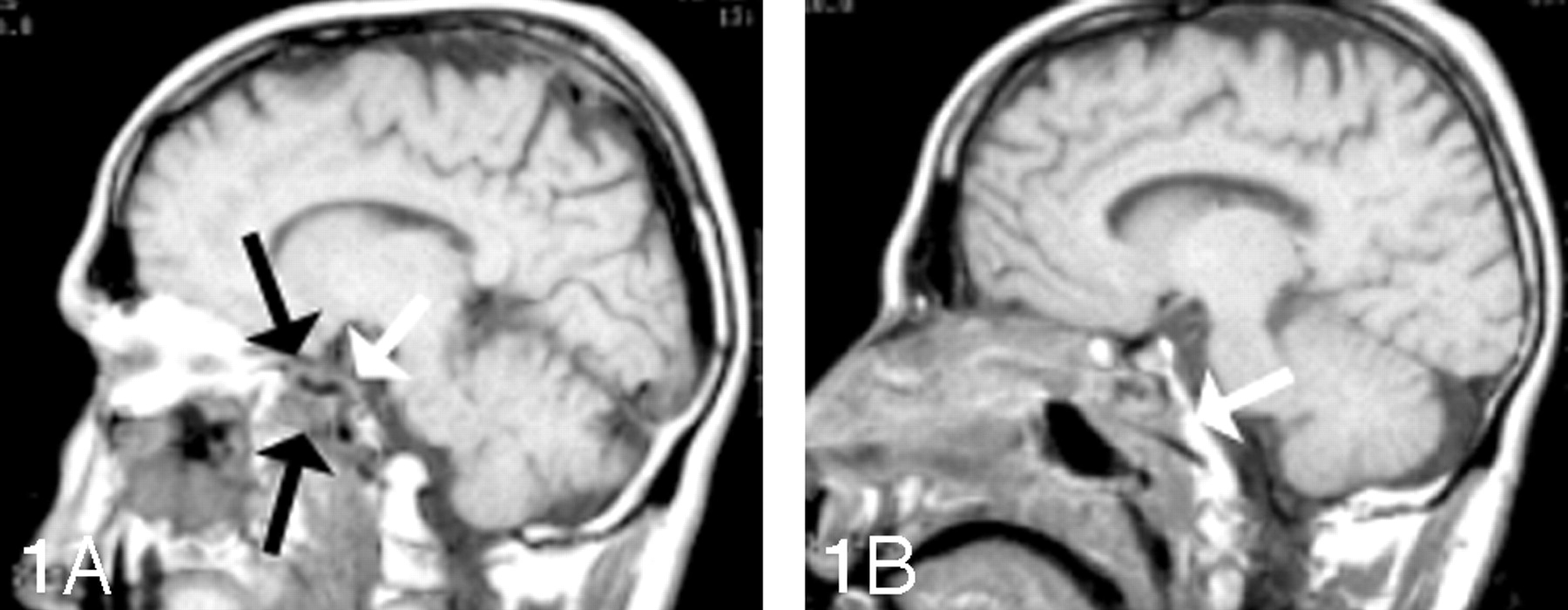
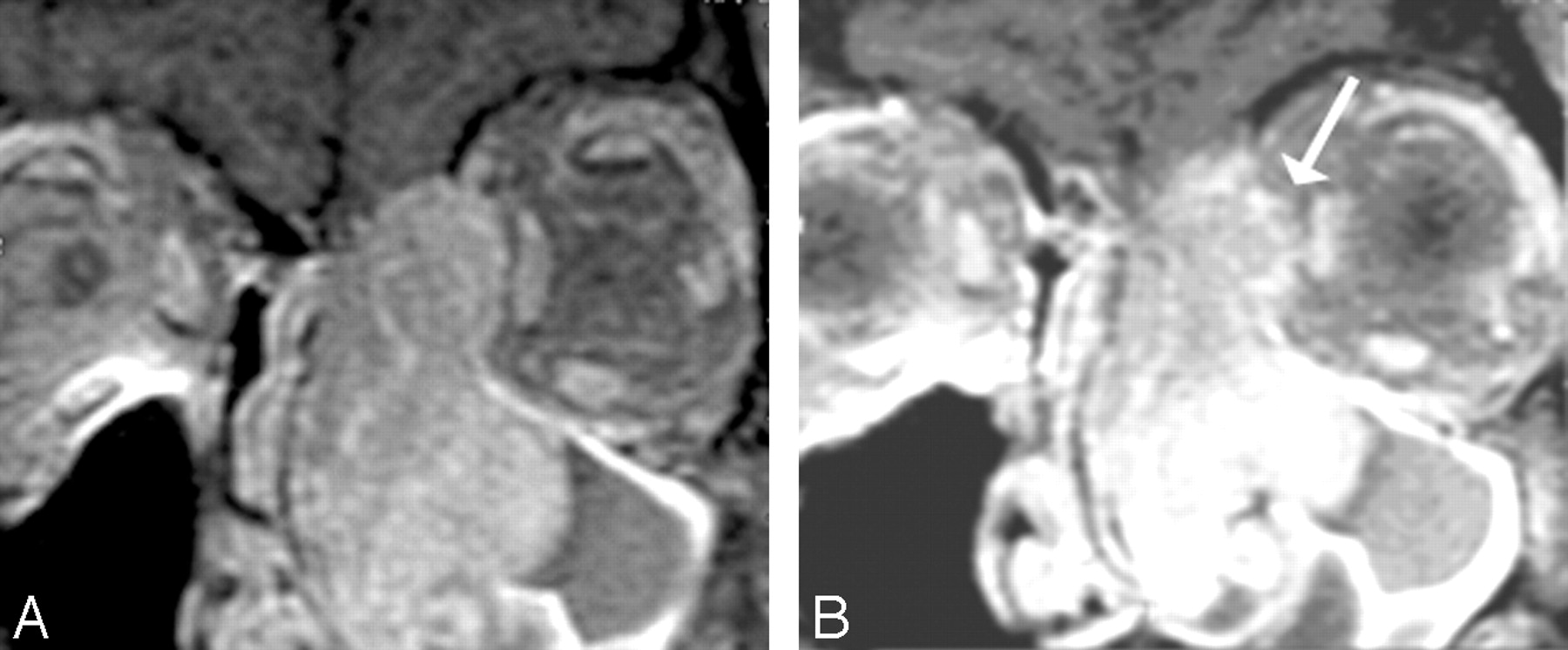
- Fig 1.
Carotid encasement; adenoid cystic carcinoma. A, Note the circumferential involvement of the left cavernous artery by a soft-tissue mass with narrowing of the carotid artery in this patient who had adenoid cystic carcinoma from the sinonasal cavity. B, This patient also demonstrates erosion of the clivus with bony infiltration of the skull base.
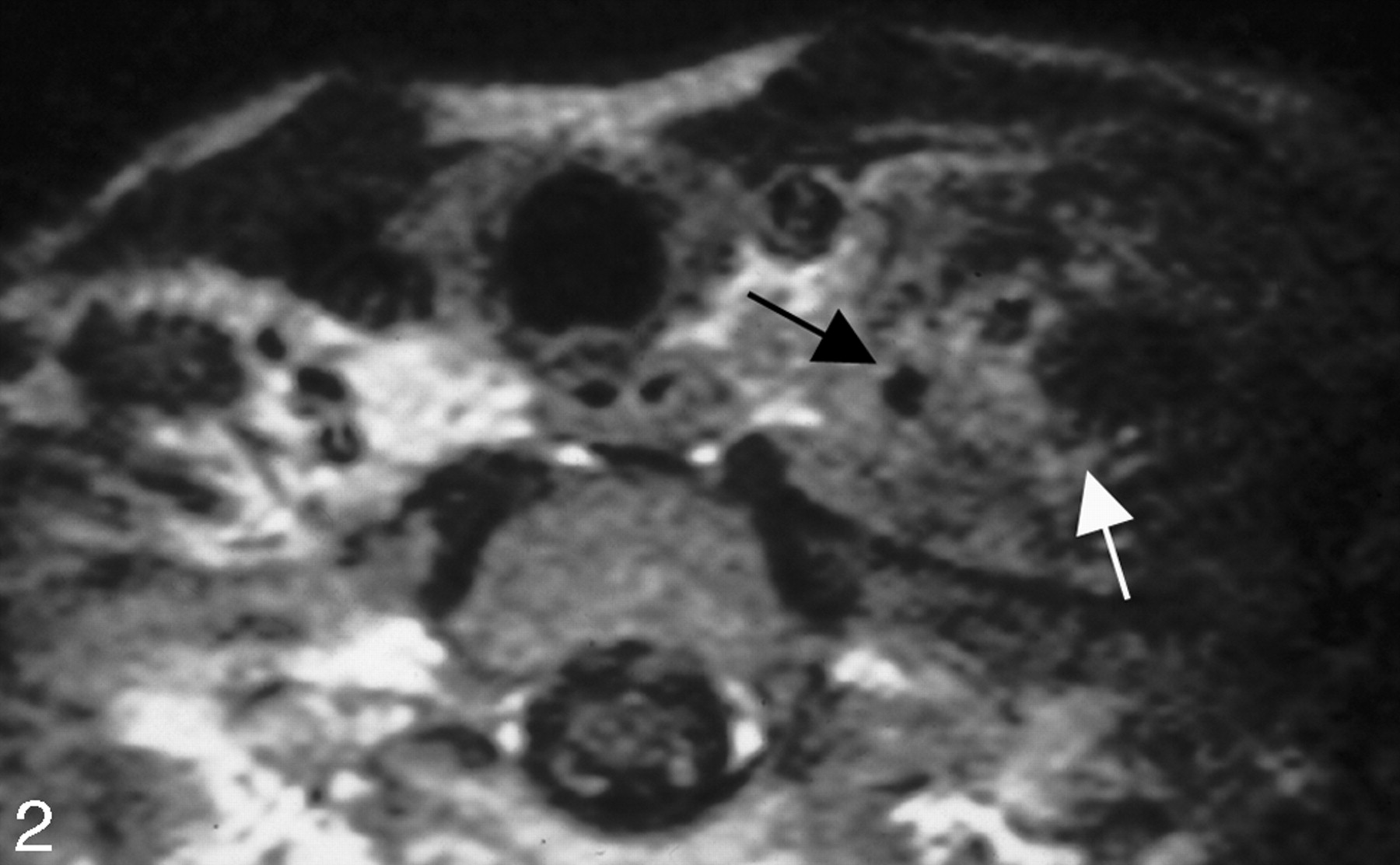
- Fig 2.
Carotid fixation. This patient who had recurrent thyroid cancer in the left side of the neck demonstrates effacement of the fat planes around the left CCA laterally (black arrow). Nonetheless, the tumor does not extend greater than 270° around the circumference of the carotid artery, and the tumor was able to be stripped off the carotid artery at surgery. Note also the tumor abutting the anterior scalene muscle on the left side (white arrow). In many instances, the head and neck surgeons believe that this is a contraindication for further surgery due to the potential for brachial plexus involvement.
- Fig 3.
Prevertebral muscular infiltration. This T1-weighted scan demonstrates a left tonsillar carcinoma, which causes effacement of the fat of the retropharyngeal space on the left. Compare the left side with the right side. The irregular margin of the muscle belies the infiltration of the longus colli in this patient with fixation of tumor.
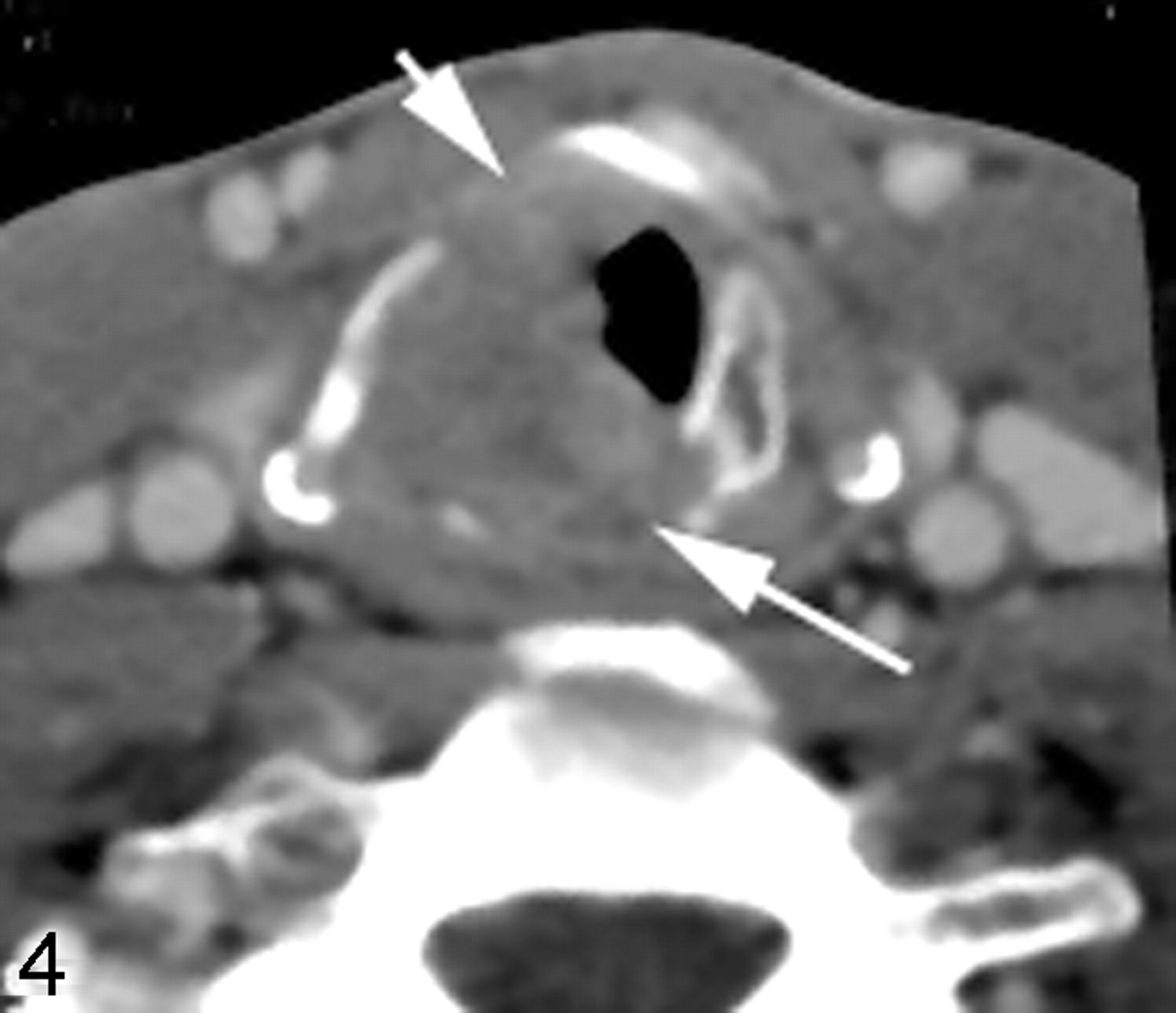
- Fig 4.
Gross infiltration of the laryngeal cartilage. Erosion of the right side of the cricoid cartilage (long arrow) is well demonstrated in this patient with laryngeal carcinoma with subglottic extension. Additionally, the anterior margin of the right thyroid cartilage (short arrow) appears to be invaded.
- Fig 5.
Laryngeal cartilage sclerosis. Axial postcontrast CT scan at the level of the true vocal cord shows sclerosis of the right arytenoid cartilage (arrow), associated with thickening of the true vocal cord. This finding is suggestive of cartilaginous invasion or perichondrial reaction.
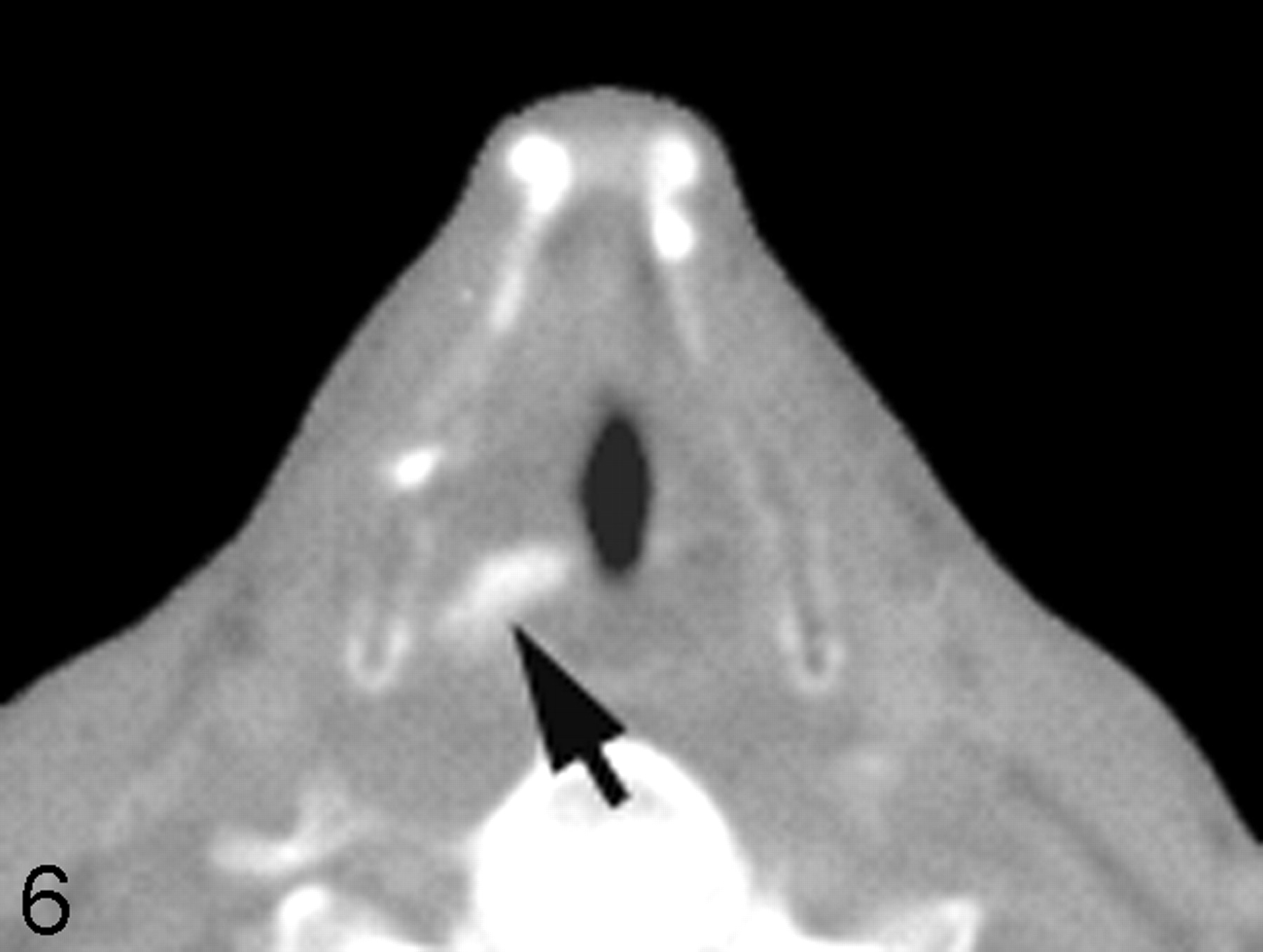
- Fig 6.
Arytenoid sclerosis in laryngeal carcinoma. Axial CT scan with bone windows shows a sclerotic right arytenoid cartilage (arrow) in a patient with true vocal cord cancer. Despite the sclerosis, there was no evidence of cartilaginous invasion on histology.
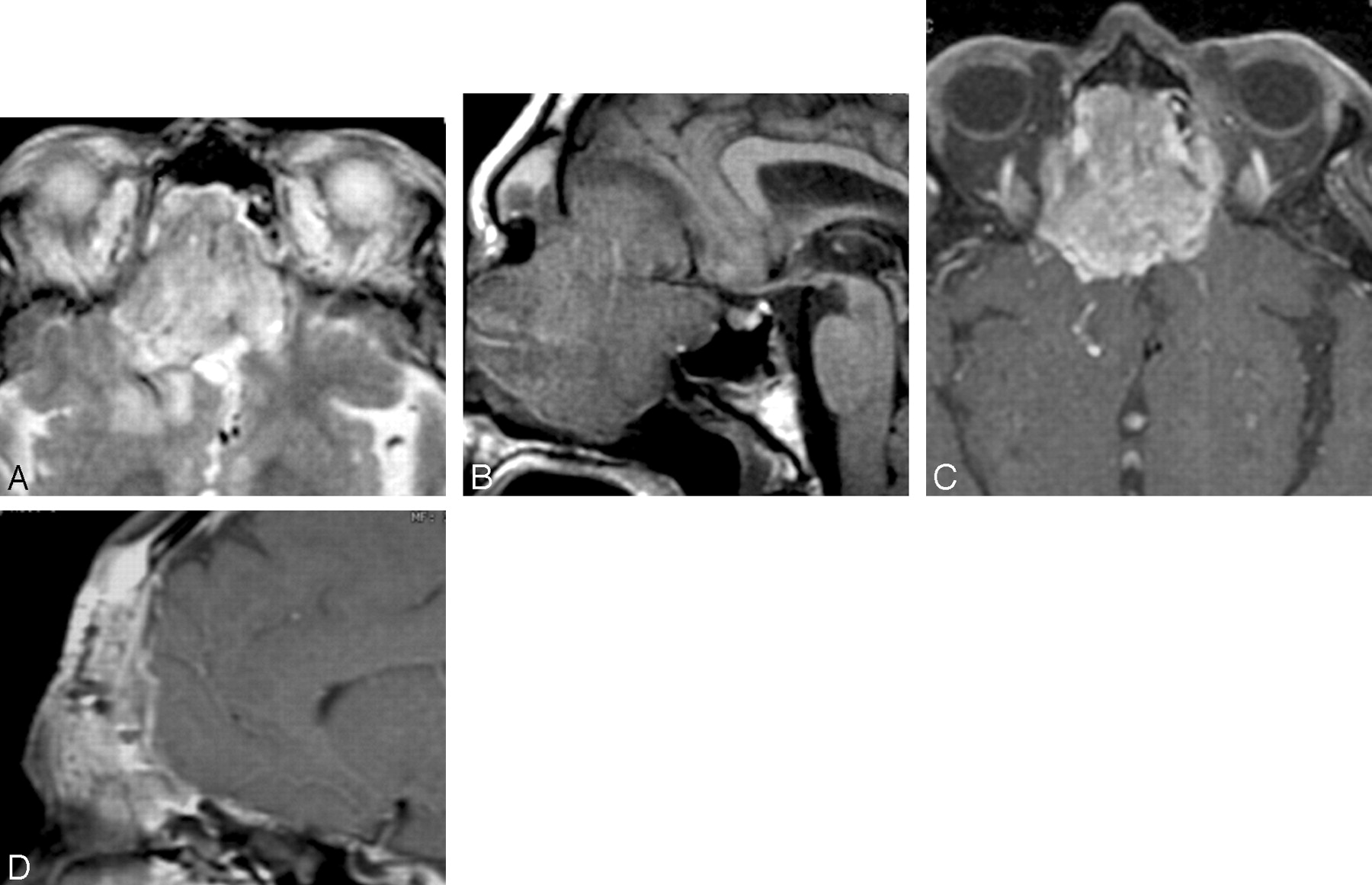
- Fig 7.
Dural and intracranial extension of mass. A, Axial T2-weighted scan demonstrates soft-tissue mass infiltrating the anterior cranial fossa with associated edema of the right frontal lobe. B, Parasagittal T1-weighted scan shows the gross infiltration across the cribriform plate to involve the anterior cranial fossa with massive involvement in an extra-axial location. C, Postcontrast fat-suppressed T1-weighted scan shows intracranial extension as well as dural infiltration and pial extension of tumor adjacent to the midline. D, A different patient with adenocarcinoma of the paranasal sinuses shows considerable thickening of the dural greater than 5 mm, indicative of dural infiltration, confirmed at surgery.
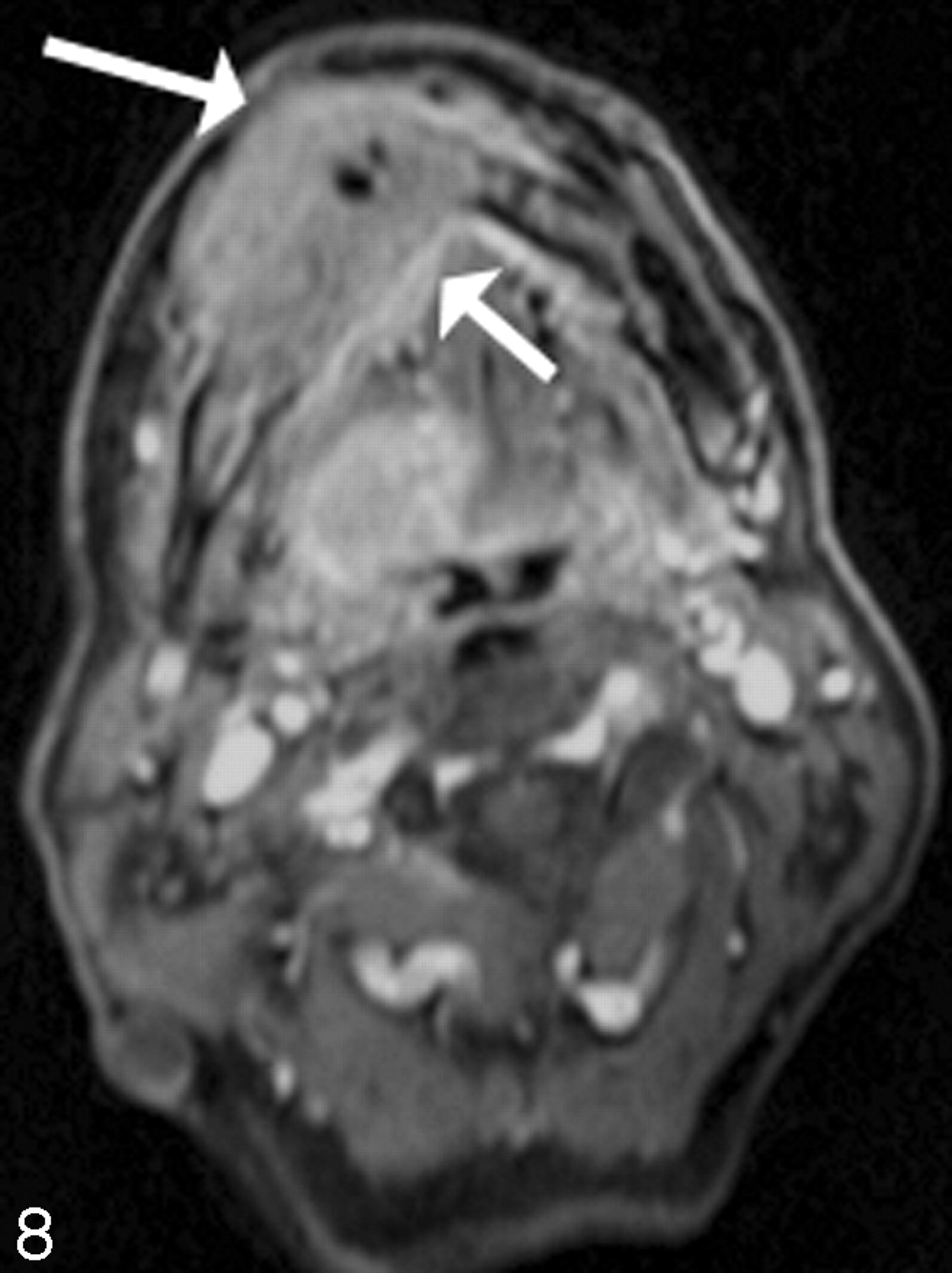
- Fig 8.
Post–gadolinium-enhanced scan through the floor of the mouth demonstrates a contrast-enhancing mass (arrow) infiltrating the right side of the mandible and extending into the subcutaneous tissue. There is an associated mass at the right lateral base of the tongue. Note infiltration of the mandible extends across the midline.
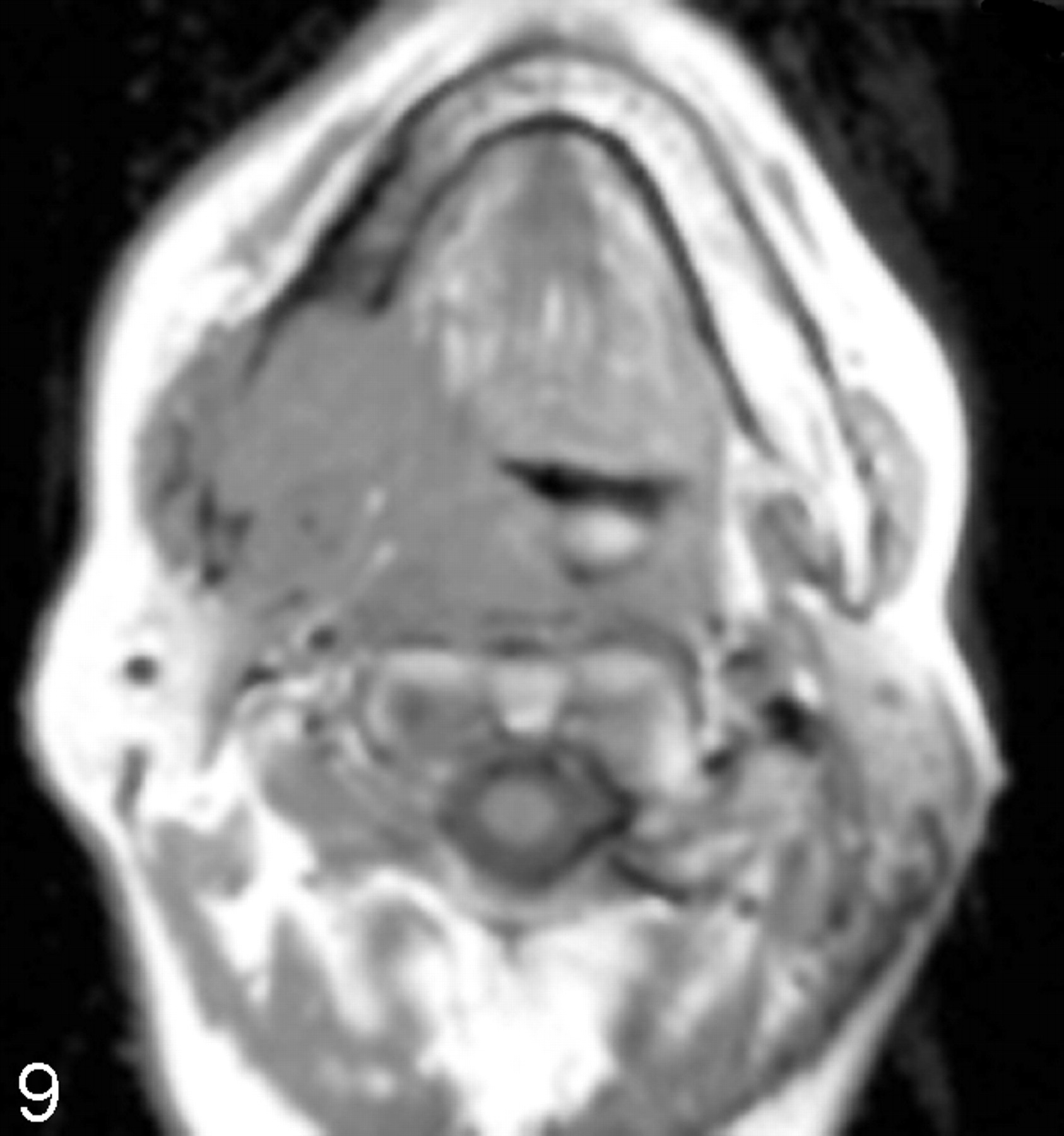
- Fig 9.
Infiltration of the mandible with retropharyngeal spread of tumor. Axial T1-weighted scan demonstrates a large mass emanating from the right palatine tonsil extending along the floor of the mouth posteriorly to infiltrate the right side of the mandible. Note that the signal intensity of the right side of the bone marrow is dark, replacing the bone marrow fat. There is effacement of the retropharyngeal fat on the right side, with tumor abutting the longus colli/capitis muscle complex.
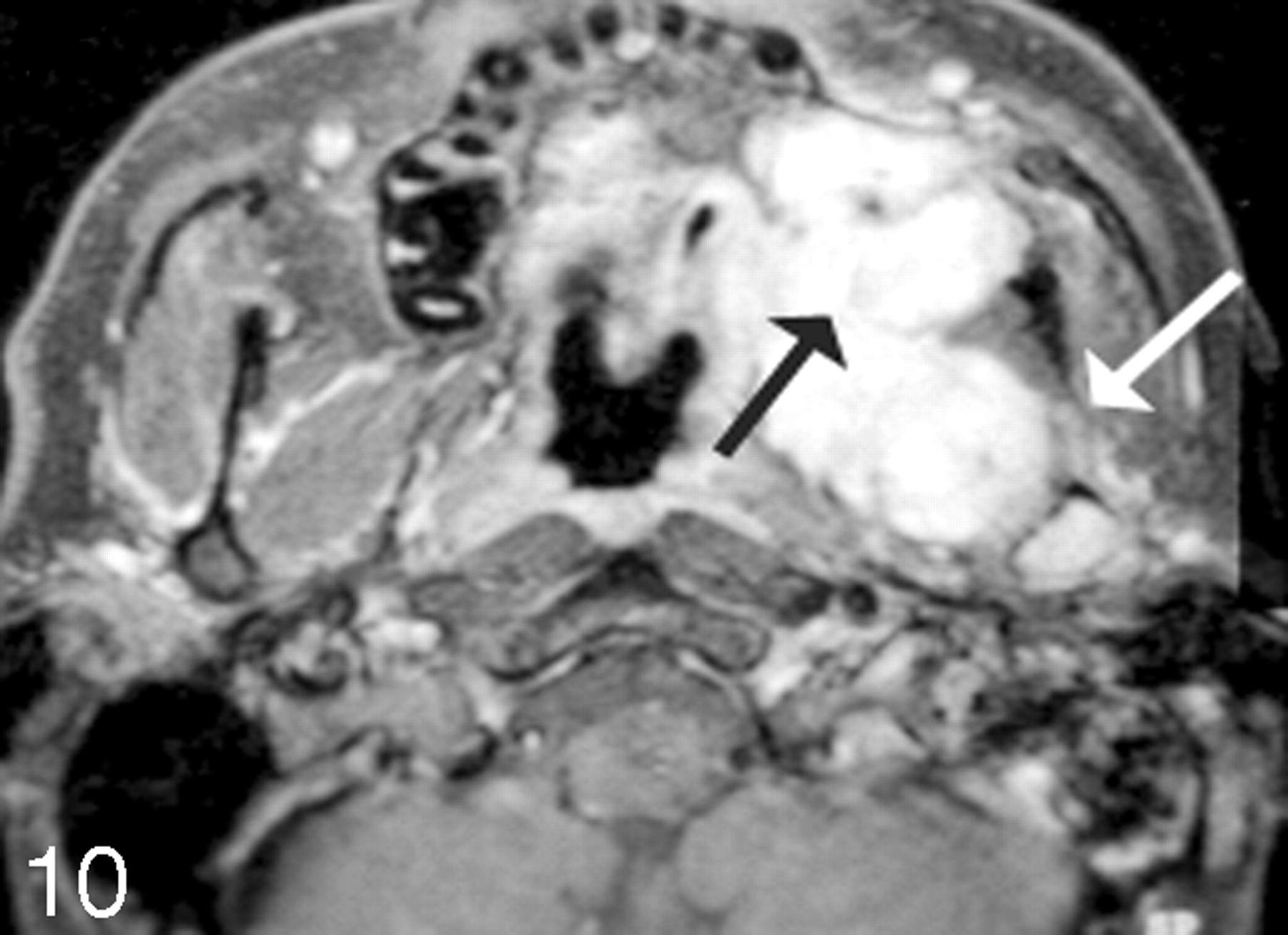
- Fig 10.
Sarcoma growing into the left maxilla. Postcontrast fat-suppressed images demonstrate soft-tissue enhancement emanating from the retromolar trigone region (black arrow), with growth into the posterior margin of the left maxilla and abutting the coronoid region of the left mandible. There is likely perineural spread as seen on the axial scan with enhancement into the inferior alveolar canal (white arrow).
- Fig 11.
Nasopharyngeal carcinoma with infiltration of the prevertebral musculature, skull base, and cavernous sinus. A, Postcontrast fat-suppressed T1-weighted scan shows a large nasopharyngeal carcinoma, which demonstrates contrast enhancement of the prevertebral musculature on the left side (arrow). B, Note the growth through the foramen ovale (arrow) into the Meckel cave and cavernous sinus on the left side via cranial nerve V. C, The cavernous sinus extension on this axial postgadolinium fat-suppressed scan is well demonstrated (arrow). There may also be enhancement in the pterygopalatine fossa on the left side.
- Fig 12.
A and B, Orbital infiltration. Postcontrast fat-suppressed T1-weighted scans show soft-tissue infiltration in the superior medial aspect of the left orbit, with irregular margins in the extraconal fat. Although there are portions of the tumor in which there still appears to be periosteum containing the tumor, the irregular margins seen more anteriorly (arrow) suggest infiltration requiring orbital surgery.
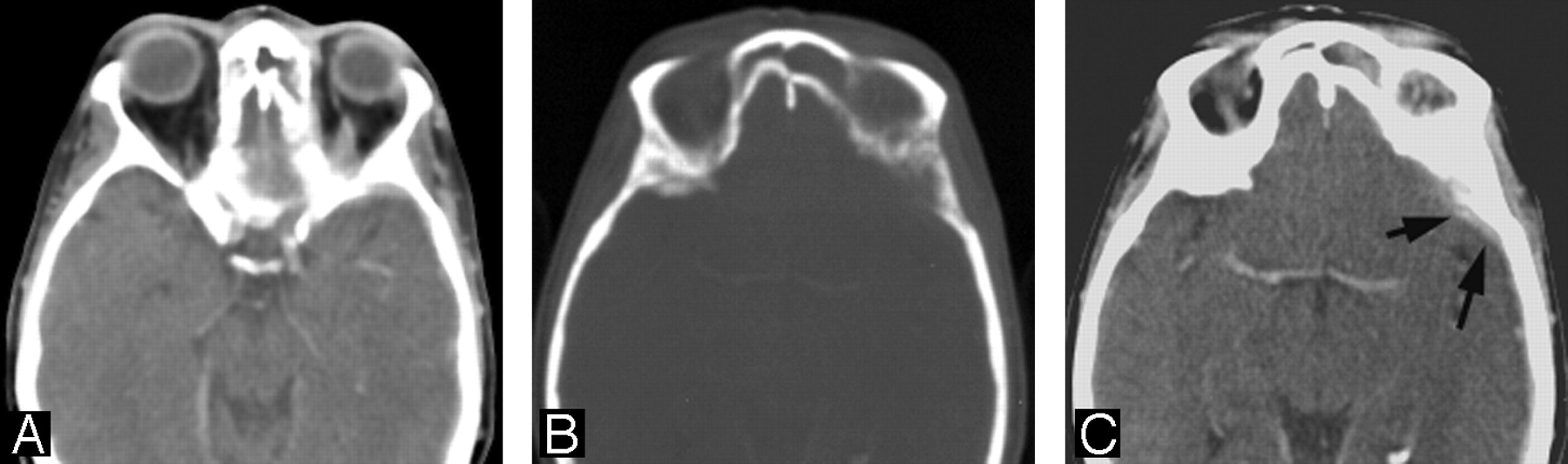
- Fig 13.
Orbital infiltration. A, Soft tissue is seen in the posterior left orbit in this patient with metastatic disease to the bone. The infiltration of the intraconal fat suggests the need for orbital exenteration surgery, if surgical treatment is even contemplated. B, Note the erosion at the junction of the posterior left orbit with the frontal bone. C, One can see that there is dural extension of the tumor accompanying the orbital infiltration (arrows).
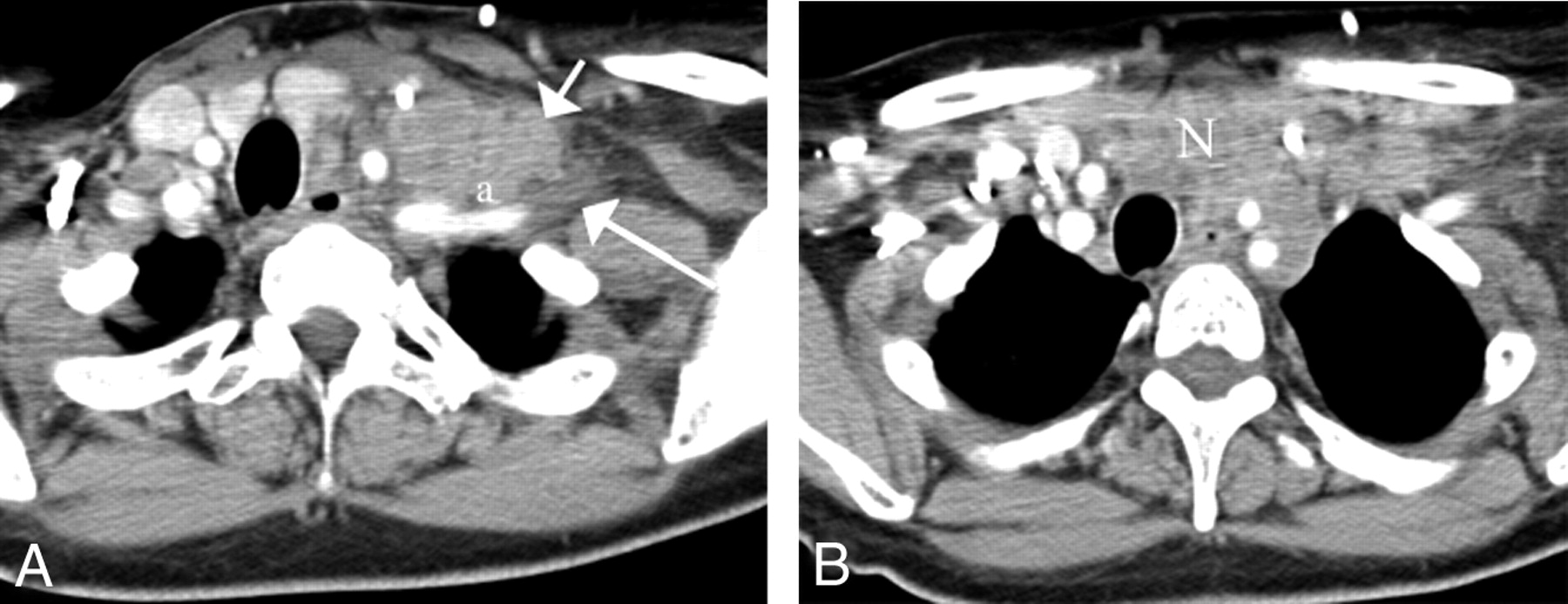
- Fig 14.
A, Nodal metastases from breast cancer (short white arrow) are seen to infiltrate the anterior scalene muscle (a) and the hypodense brachial plexus (long white arrow) on this enhanced axial CT image. A tongue of nodal disease indents the plexus beyond the anterior scalene muscle.
B, This same nodal mass (N) infiltrates the anterior mediastinum and abuts on the supraortic vessels in the left.














Tables
Site T4a T4b Oral cavity Tumor invades adjacent structures, bone, muscle of tongue, maxillary sinus, facial skin Tumor invades masticator space, pterygoid plates, or skull base and/or encases internal carotid artery Oropharynx Tumor invades the larynx, deep muscle of tongue, medial pterygoid, hard palate, or mandible Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base or encases carotid artery Hypopharynx Tumor invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, esophagus, or central compartment Tumor invades prevertebral fascia, encases carotid artery, or involves mediastinal structures Supraglottis, glottis, subglottis Tumor invades through the thyroid cartilage and/or invades tissues beyond the larynx (e.g. trachea or esophagus) Tumor invades prevertebral fascia, encases carotid artery, or invades mediastinal structures Maxillary sinus, nasal cavity, ethmoid sinus Tumor invades anterior orbital contents, skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid or frontal sinus Tumor invades orbital apex, dura, brain, middle cranial fossa, cranial nerves other than V2, nasopharynx, or clivus Salivary glands Tumor invades skin, mandible, ear canal, and/or facial nerve Tumor invades skull base and/or pterygoid plates and/or encases carotid artery Thyroid Tumor grows outside the thyroid capsule into subcutaneous tissue, larynx, trachea, esophagus, recurrent laryngeal nerve Tumor invades prevertebral fascia or encases carotid arteries or mediastinal vessels Ultrasonographic Staging System Stage I Independent carotid artery pulsations and an obvious plane of cleavage visible. Stage II Residual independent mobility of the carotid artery and lymph node during various maneuvers but an obvious cleavage plane not visible. Stage III Loss of independent mobility of the carotid artery with luminal compression. Vascular boundaries no longer visible and circular encroachment of the vessel is presumed. Stage IV Gross invasion of the carotid artery with and without intraluminal tumor present associated with impaired flow velocity in color Doppler US.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Are Gadolinium-Enhanced MR Sequences Needed in Simultaneous 18F-FDG-PET/MRI for Tumor Delineation in Head and Neck Cancer?
- Do Radiologists Report the TNM Staging in Radiology Reports for Head and Neck Cancers? A National Survey Study
- Contrast-Enhanced PET/MR Imaging Versus Contrast-Enhanced PET/CT in Head and Neck Cancer: How Much MR Information Is Needed?
- Imaging of the pharynx and larynx
- Covered stents safely utilized to prevent catastrophic hemorrhage in patients with advanced head and neck malignancy
- 18F-FDG PET as a Routine Posttreatment Surveillance Tool in Oral and Oropharyngeal Squamous Cell Carcinoma: A ProspectiveStudy
- Definitive chemoirradiation for resectable head and neck cancer: treatment outcome and prognostic significance of MRI findings
- Imaging of the pharynx and larynx