
Abstract
Summary: We report a rare complication of autopsy-proven fat and bone marrow embolization following percutaneous vertebroplasty in a patient who had no evidence of cement leakage. Cement injection was done during one patient encounter, covering 3 vertebral levels by using a unipedicular approach. Patients may have complications even without polymethylmethacrylate leakage.
With the introduction of percutaneous vertebroplasty (PV) in 1984,1 interventional radiologists have had success with patients with pain associated with vertebral body compression fractures.2–5 The incidence of complications has been reported to be between 1% and 3%. Potential complications include hemorrhage, infection, pulmonary embolism, local trauma to nerve roots, spinal cord, or lung, fracture of the pedicle, and recurrent pain. These conditions are highly associated with cement leakage.2 In this report, we show that major complications can occur in the absence of cement leakage and that assessment of a high-risk patient is fundamental in the decision-making process of whether vertebroplasty should be attempted.
Case Report
A 69-year-old woman with past medical history of emphysema (requiring home oxygen), pulmonary hypertension with cor pulmonale, acid reflux, coronary artery disease, cardiac arrythymias, and hypertension was referred for interventional radiology with onset of intractable back pain for 3 months. Despite use of propoxyphene (100 mg)/acetaminophen (650 mg 3 times daily), the patient continued to complain of pain (8 of 10 in severity) with both dull and sharp components. The patient could not recall any precipitating factors. Sagittal T1/T2/short T1 inversion recovery (STIR) and limited axial T2-weighted images of the thoracic spine showed acute/subacute compression fractures of T7–T12 with no retropulsion.
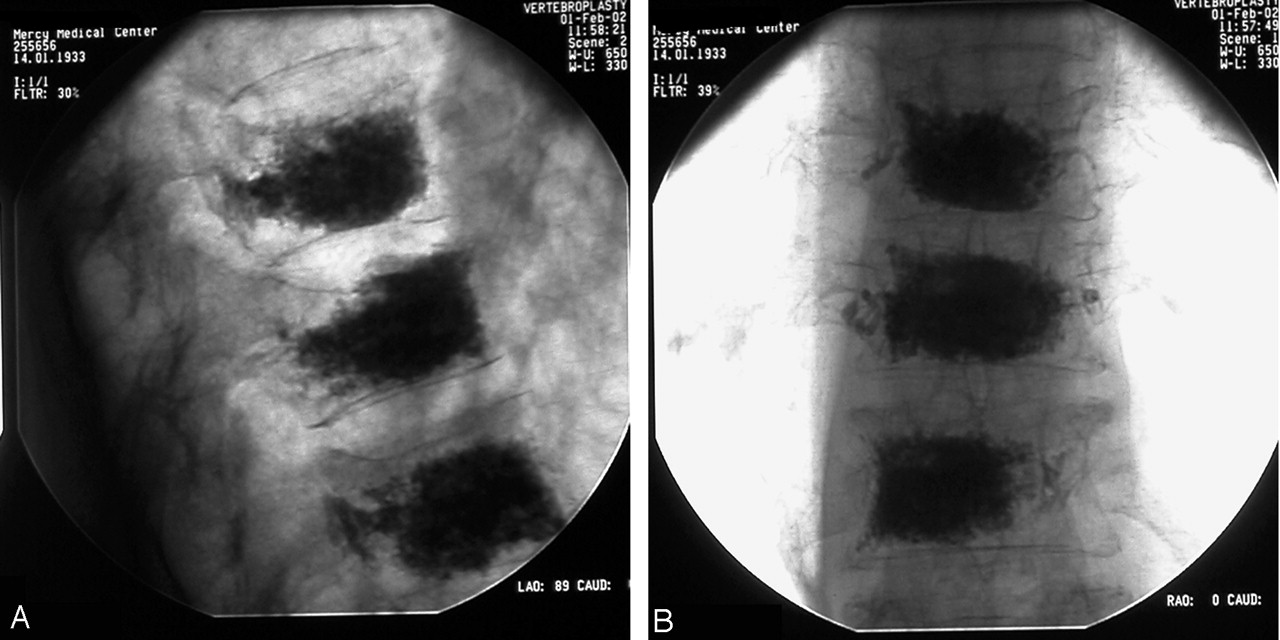
She was admitted for outpatient vertebroplasty. Her preoperative electrocardiogram revealed normal sinus rhythm, and right ventricular hypertrophy with right axis deviation, consistent with cor pulmonale. Following anesthetic preparation, the patient was placed prone on the angiographic table. Initially the T12 level procedure was accessed by using an 11-gauge trocar placed via a left transpedicle approach. Delivery of methylmethacrylate was administered by using a PCD device by Codman Cranioplastics (Raynham, Mass). By using this same technique, T11 was treated, followed by T10. There was a 5-minute dwell time between each level treated to obtain hemostasis. The patient’s vital signs remained stable. Volumes used are as follows: 5 mL were injected at T10, 6 mL were injected at T11, and 5 mL at T12 (Fig 1). The procedure lasted from 10:40–12:07, and the operator reported good filling and results. In postoperative recovery the patient was dressed with assistance after gradually awakening at 14:30. She was alert and oriented and, in keeping with our protocol, was discharged. Her husband explained that on the way home she became very sleepy, so much so that he had to hold up her head. When they arrived home, she was unresponsive and cardiopulmonary resuscitation was begun. Emergency medical services were called, and she was taken to the emergency department, where she did not recover and was pronounced dead at 16:57.

A, Lateral fluoroscopic view showing near-complete filling of T10, T11, T12.
B, AP fluoroscopic view showing near-complete filling with leakage into the paravertebral vein and basivertebral venous plexus. There is relative sparing of the right lateral fourth of T10 and T11 and sparing of the right third of T12.
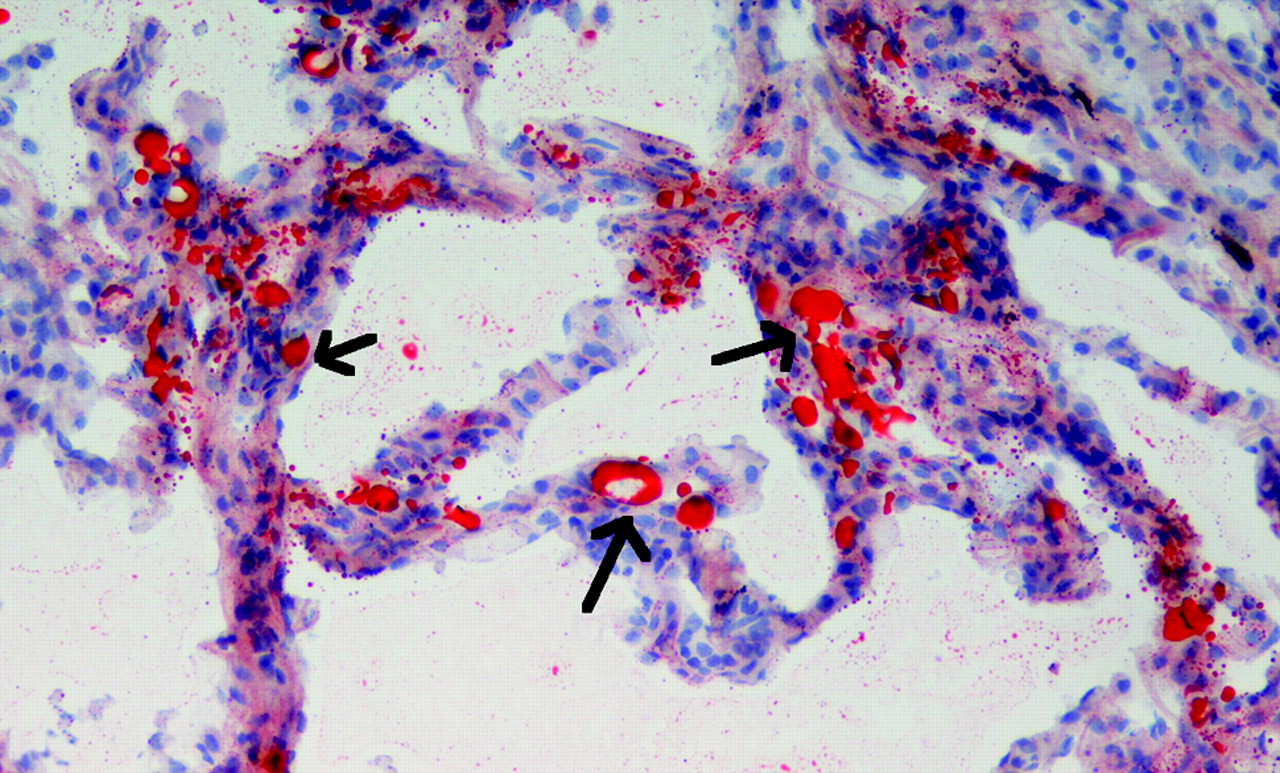
The county coroner ordered an autopsy be performed, which was completed the next day. The pathologist stated on final summary that there was a significant narrowing of the pulmonary artery by a chronic adherent thrombus, causing 80% stenosis of the main branches. More acutely there was diffuse fat and bone marrow embolization to the lungs (Figs 2 and 3). Further findings include cor pulmonale of the heart and lungs and severe diffuse emphysema of centrilobular type. Specifically, no cement leakage outside of the individual vertebrae was noted (Fig 4). The combination of emboli and the disease processes of severe emphysema and pulmonary hypertension resulted in severe compromise of the pulmonary circulation. Therefore, in the light of the case history and the autopsy findings, it was the pathologist’s opinion that this individual died from fat embolization.

Microscopic view (200×) of alveoli stained in oil Red-O by using a frozen section highlighting fat emboli. The fat emboli are seen as red dots within capillaries of the lung.

Hematoxylin-eosin routine stain (200×) showing bone marrow emboli in arteriole. The arrows indicate a bone marrow embolus within an arteriole of the lung. The embolus has hematopoietic cells and fat droplets characteristic of bone marrow.

Gross specimen of T10, T11, and T12 at autopsy showing no leakage of methylmethacrylate outside of individual vertebrae. Tan areas (arrows) represent cement within the vertebral bodies. Bone marrow is seen as the darker brown segments. The tan bands traversing the specimen are the intervertebral disks.
Discussion
Clinically, percutaneous vertebroplasty has been shown to provide relief in 80%–90% of patients treated.1,3,6,8 Complication rates remain low and have been reported to be associated with cement leaks into adjacent structures.4,7,8 To the best of our knowledge, only one case has been reported of fatal fat and bone marrow embolism as a complication of vertebroplasty.9 A study using a sheep model compared the incidence of vertebroplasty and fat embolism, and the results suggest that vertebroplasty provokes fat embolism.10
Fat embolism is characterized by release of fat droplets into systemic circulation after a traumatic event. This is not to be confused with fat embolism syndrome (FES), which is the clinical consequence of fat embolism characterized by a triad of pulmonary distress, mental status changes, and petechial rash 24–48 hours after pelvic or long-bone fractures.11 In 1861, Zenker described the first fat droplets in a lung of a railway worker who had sustained a severe crush injury.12 Since then, numerous papers have been written, but only 2 mechanisms of the pathophysiology of FES have been accepted: the common mechanical pathway, which suggests that, once a fracture has occurred, fat emboli that are released into venous circulation mechanically obstruct the capillaries of end organs; and the biomechanical and inflammatory cascade that states once a fat embolus is enlodged in the pulmonary vasculature it initiates a biochemical and inflammatory cascade that damages lung parenchyma.11 Why this cascade starts in some patients but not in others is unclear. Fat embolism has been shown to be a common complication in patients who undergo hip and knee arthroplasty13,14 and during intramedullary nailing.15,16
In our patient, it is unclear what mechanism may have caused her to have bone marrow emboli. We hypothesize that the methylmethacrylate, when introduced into the vertebral body, caused an increase in the intramedullary pressure. This pressure triggered the marrow to dislodge, forcing it into the path of least resistance, the venous circulation.
To avoid this degree of complication, it may be advisable to lower the cement volumes injected. As represented in Fig 1, near-complete filling was achieved with very little sparing of the vertebral bodies. It may be appropriate to limit the volumes to no more than 4 mL per thoracic vertebra and 6 mL per lumbar vertebra. In our experience, this volume is suitable for adequate pain relief and vertebra stabilization. As noted, the cement and delivery kit used during this procedure was offered by Codman Cranioplastics. We now use Stryker P cement with its PCD device (Stryker-Howmedica Osteonics, Rutherford, NJ).
It is our belief that a controlled fat and bone marrow embolization occurs in all vertebroplasties and kyphoplasties, much as it does in numerous orthopedic procedures. Most patients are able to tolerate the fat and bone marrow embolization that occurs and are thus asymptomatic. It is imperative, however, to recognize the high-risk patient, those with compromised cardiopulmonary reserve, specifically patients with (1) chronic obstructive pulmonary disease (especially those receiving home oxygen), (2) pulmonary arterial hypertension/cor pulmonale, and (3) any patient with a history of deep venous thrombosis or pulmonary embolism. It may be safer for these patients to undergo conservative therapy, because risks may outweigh benefits. We have had experience with numerous high-risk patients who have had as many as 2 levels treated in one session by using Simplex P (Stryker-Howmedica Osteonics) cement with total volumes <8 mL with no complications and excellent outcomes. The safety of this approach, however, has not yet been definitively established, because of the limited sample size. Consideration should be made for overnight admission of these high-risk patients.
In conclusion, vertebroplasty is a safe and effective procedure in experienced hands though, we believe it ought to be considered a controlled fat and bone marrow embolization. Therefore, the concept of high-risk patients for vertebroplasty should be recognized and appropriate modifications in clinical practice advised. Furthermore, it is important to note that severe complications can occur without the presence of cement leakages.
Acknowledgments
We would like to thank the staff of Mercy Medical Center and Community Hospital, especially Cindy Nixon. Special thanks to the Clark County Coroner’s office, including Richard A. Marsh, MD, and Robert V. Stewart, MD.
Footnotes
Presented as an excerpta extraordinaire at the 43rd annual meeting of the American Society of Neuroradiology, May 21–27, 2005, Toronto, Ontario, Canada.
References
- Received December 7, 2004.
- Accepted after revision March 10, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}