
Abstract
BACKGROUND AND PURPOSE: Optimal estimation of cerebral blood-flow volume (BFV) may be an important indicator for better evaluation of the patients with cerebrovascular disorders. In this study, we compared the BFV values at bilateral internal carotid and vertebral arteries of healthy volunteers obtained with color Doppler, power Doppler, and B-flow ultrasound (US) studies and tried to determine which examination is more correlated with MR phase-contrast quantification.
METHODS: BFVs of the internal carotid and vertebral arteries of 40 healthy volunteers (19 men and 21 women; age range, 20–47 years) were measured by using color Doppler, power Doppler, B-flow US and MR phase-contrast imaging. The flow measurements obtained with the sonographic techniques were compared with MR phase contrast, which is accepted as the most reliable method for the estimation of cerebral BFV.
RESULTS: Quantification with power Doppler imaging showed the highest values among sonography techniques, followed by color Doppler imaging, B-flow imaging (BFI), and MR phase-contrast flow quantification. There was a statistically significant difference between the flow-volume values obtained with these 4 different techniques (P < .05). BFI yielded the closest values (internal carotid arteries, 238.84 mL/min; vertebral arteries, 51.16 mL/min) to MR phase-contrast flow quantification study with higher correlation rates.
CONCLUSION: Flow volumes obtained with BFI showed the highest correlation with MR phase-contrast imaging among 3 different sonography techniques. B-flow sonography may be a very effective and cost-efficient alternative for MR phase-contrast studies for the calculation of cerebral BFV.
The quantitative measurement of carotid and vertebral blood-flow volume (BFV), which has been suggested as an estimate of total cerebral BFV is clinically useful in a variety of cerebrovascular diseases. It allows hemodynamic evaluation of a carotid stenosis, the presence of collateral pathways and associated conditions, investigation of vertebrobasilar insufficiency, estimation of the shunt volume in cerebral arteriovenous malformations, and monitoring of cerebral BFV before and after carotid endarterectomy.1–5 Therefore, an accurate BFV measurement technique is of great value in patients with cerebrovascular disease.
The quantitative measurement of cerebral BFV is possible by different noninvasive methods such as stable xenon-enhanced CT, single-photon emission CT, positron-emission tomography, and MR imaging technology. These have proved to achieve reliable and accurate measurements of cerebral BFV. All of these techniques, however, are bulky and expensive. More important, they require the transfer of patients to the imaging or radionuclear facility and therefore are of limited use in critically ill, sedated, or ventilated patients.
MR phase-contrast imaging has been shown to be an accurate technique for flow quantification.6–8 Previous in vitro and in vivo studies have demonstrated a close correlation between phase-contrast MR imaging and Doppler require ultrasound (US).9,10 Color duplex sonography is suggested to be a potentially practical method for the measurement of BFV in the ICA and vertebral artery as an estimate for cerebral blood flow.11,12 Even though sonographic imaging has been shown to overestimate BFV it is still being used because it is practical and widely available compared with other techniques.13 B-flow imaging (BFI), which is a recently introduced non-Doppler technology enabling real-time imaging of blood flow, is a promising technique in real-time visualization of blood vessels.14,15
In our prospective study BFV quantification by color Doppler imaging (CDI), power Doppler imaging (PDI), and BFI were compared with MR phase-contrast quantification, to determine which of these 3 different sonographic BFV measurement techniques is best correlated with MR quantification.
Subjects and Methods
The internal carotid and vertebral arteries of 40 volunteers were evaluated with CDI, PDI, B-flow US, and MR phase-contrast imaging. Twenty-one of the subjects were women and 19 were men. The mean patient age was 33.67 ± 7.98 years (mean ± SD), and the age range was 20–47 years. Sonograms were obtained with a GE Logiq 9 (GE Heathcare, Milwaukee, Wisc.) by using a 4–10-MHz linear transducer. MR phase-contrast flow quantification and MR angiography were performed with a 1T magnet (Signa HiSpeed; GE, Milwaukee, Wis.) by using a standard cervical coil. After the explanation of study protocol, all volunteers had given informed consent before BFV measurements and the study was performed with approval from the institutional review board.
The internal carotid and vertebral arteries on both sides were studied with these 4 techniques within 2 hours and intravascular flow volumes were calculated. All volunteers were allowed to rest on the examination table for 10 minutes before obtaining volume measurements with sonography and MR. The examinations were complete in all patients except for 2 subjects in whom the vertebral arteries could not be visualized at both sides via BFI because of poor flow signal intensity either due to deep location or small vessel size. Before volume flow measurements were performed, a routine examination of the carotid and vertebral arteries was made to exclude any pathologic processes like atherosclerosis or stenosis.
The subjects were examined with CDI first, followed by PDI, and BFI. For flow-volume measurements, a straight segment of the internal carotid artery at least 2 cm above the carotid bulb, and any intertransverse straight segment of the vertebral artery were selected. The same sagittal plane was used for the flow measurements, maintaining the plane of section as constant as possible. Windows of color Doppler, power Doppler, and B-flow images were used to place the sample volume for supplemental pulsed wave (PW) interrogation at the selected site of measurement. The sample volume was extended over the entire vessel diameter.
Angle of insonation was adjusted at or below 60° and was kept constant while alternating between different modes. For color and power Doppler US, the imaging parameters (color gain, wall filter, etc) were adjusted for each image with optimal color saturation with no aliasing or color “bleeding” over the lumen. As for B-flow sonography, high sensitivity levels were used with a single focus positioned just below the range of interest.
Cross-sectional diameter of the vessels was measured by using color Doppler, power Doppler, and B-flow images. The luminal diameter, measured on the magnified color, power Doppler, and B-flow images of the vessel, was determined as the distance between the parallel walls of the vessel contrasted by color Doppler, power Doppler, or B-flow signals. The diameter of the vessel was measured as close to the line of interrogation as possible, for better accuracy. The intravascular BFV measurements were automatically calculated by the built-in software of the sonography device after the image was frozen, as the product of angle-corrected, time-averaged flow velocity and the cross-sectional area of the vessel.
The flow measurements were repeated 3 times for each vessel and for each US technique and then averaged to provide the BFV estimates of each vessel to minimize the random errors to an acceptable level. All sonographic examinations were performed by a single radiologist experienced in sonography.
MR angiography images of the neck vessels were obtained by 2D time-of-flight sequence in the axial plane (TR/TE, 18/7; flip angle, 60°; section thickness, 3 mm; excitation, 1; field of view [FOV], 32 cm; matrix, 256 × 256). To obtain MR phase-contrast flow quantification of the internal carotid and vertebral arteries, a 2D nontriggered phase-contrast pulse sequence was used (TR/TE, 29/7.7; section thickness, 5 mm; excitations, 2; FOV, 26 cm; matrix, 256 × 256). The velocity encoding was 120 cm/s. The scan plane for velocity images was chosen perpendicular to vessel of interest on maximum intensity projection 2D time-of-flight MR angiography images. Flow measurement was made at the straight portion of the artery between the carotid bifurcation and the petrous segment of the skull base for the internal carotid artery and any extracranial straight segment for vertebral artery.
Volumetric flow rate was calculated by drawing a region of interest manually around the vessel encompassing all pixels on the magnified velocity image. In the selected section, another region of interest was placed as background region of interest to correct the phase offset. The volumetric blood flow rate during the acquisition time was calculated by integrating the time averaged velocity and the area on the velocity image in the region of interest. The flow measurements were repeated 3 times by the same operator, and the flow values were averaged.
Statistical analysis was performed with a commercially available statistical software program (SPSS 11.0, Chicago, Ill). A paired sample t test was used to determine the statistical significance of differences between different sonographic techniques and MR phase-contrast flow quantification, and the Pearson correlation test was used for the evaluation of correlation between BFV measurements. The level of statistical significance was set at P ≤ .05.
Results
The overall results of flow volume measurements of the internal carotid arteries and vertebral arteries obtained by sonographic techniques and MR phase-contrast imaging are summarized in the Table 1.
Mean of blood flow volume measurements for different imaging techniques
Among all techniques PDI gave the highest flow volume values in the vessels, followed by quantifications obtained by CDI, B-flow, and MR phase-contrast velocity imaging (Figs 1A–D and 2A–D). There was, however, a significant difference between BFV measurements of the internal carotid artery and vertebral artery, when each sonographic technique was compared with MR phase-contrast imaging (P < .05). Peak velocity measurements did not differ significantly between color Doppler, power Doppler, and B-flow techniques, which were 77.22 cm/s, 76.79 cm/s, and 76.72 cm/s, respectively, for internal carotid arteries and 43.79 cm/s, 44.63 cm/s, and 44.61 cm/s, respectively, for the vertebral arteries (P > .05); however, diameter measurements obtained with these 3 sonographic techniques, namely color Doppler, power Doppler, and B-flow US differ significantly (0.53 cm, 0.55 cm, and 0.44 cm, respectively, for internal carotid arteries and 0.33 cm, 0.35 cm, and 0.26 cm, respectively, for the vertebral arteries; P < .05).

A, Flow volume measurement of internal carotid artery by different sonographic techniques and MR phase-contrast imaging in a healthy 29-year-old man. With CDI, the vessel diameter at the area of interest was measured as 0.46 mm and the flow volume was calculated as 294.99 mL/min.
B, The flow volume measurement with PDI from the same segment as panel A. The vessel diameter was measured as 0.48 mm and blood-flow volume was calculated as 317.92 mL/min.
C, The flow volume measurement obtained with BFI revealed the lowest values. The vessel diameter was measured as 0.45 mm and blood-flow volume was calculated as 260.56 mL/min.
D, MR phase-contrast flow quantification (TR/TE, 29/7.7) of the same internal carotid artery revealed a blood-flow volume of 246.9 mL/min.

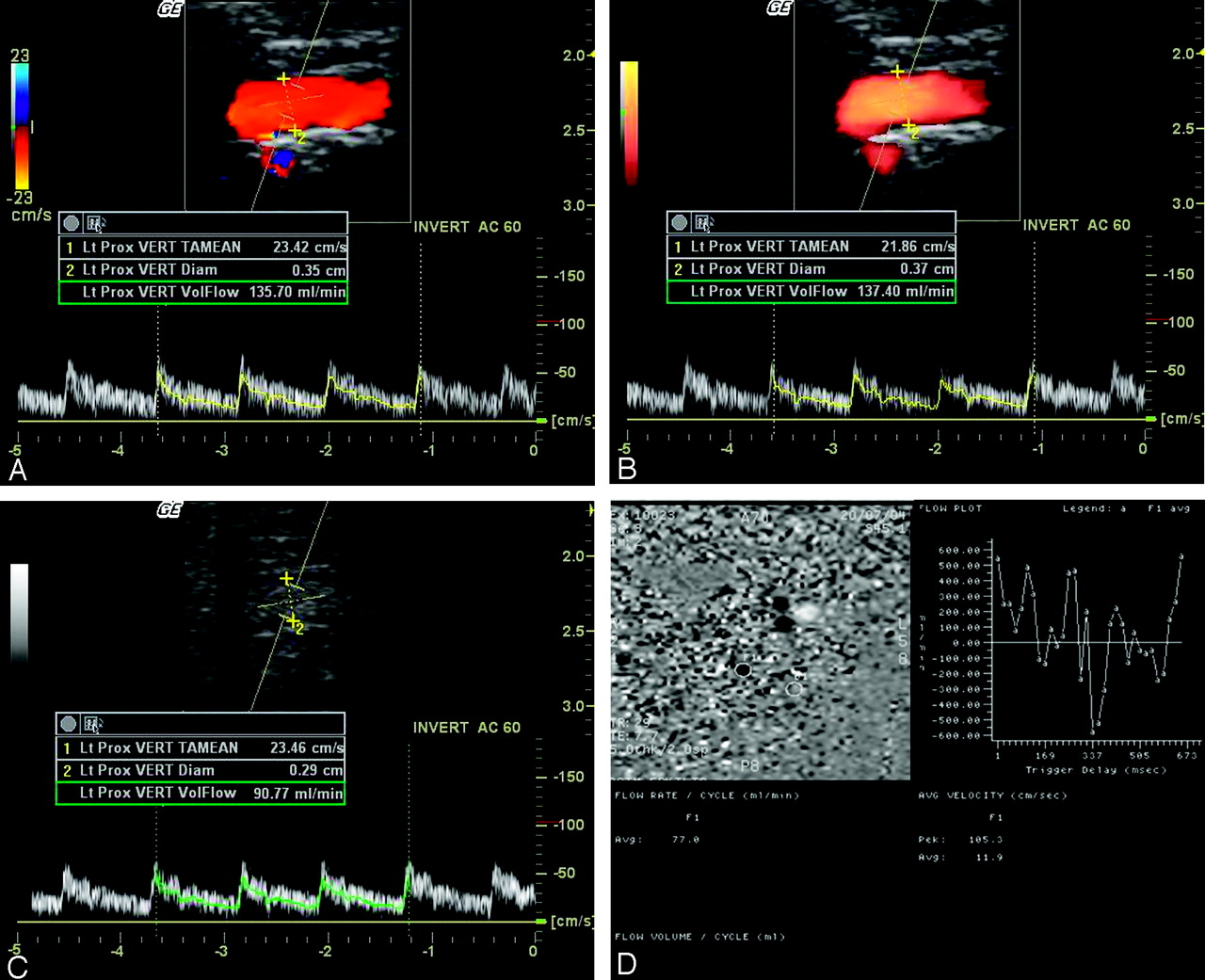
A, Flow volume measurement of left vertebral artery by different sonographic techniques and MR phase-contrast imaging in a 29-year-old subject. With CDI the vessel diameter was measured as 0.35 mm and the flow volume was calculated as 135.70 mL/min.
B, With PDI, the vessel diameter was measured as 0.37 mm and the flow volume was calculated as 137.40 mL/min.
C, With B-flow imaging the vessel diameter was measured as 0.29 mm and the flow volume was calculated as 90.77 mL/min.
D, MR phase-contrast flow quantification (TR/TE, 29/7.7) of the same vertebral artery revealed a blood-flow volume of 77.0 mL/min.
Among the sonographic techniques, BFI provided the closest flow-volume values to MR phase-contrast flow quantification with a smaller mean and range of difference within the 95% limit of agreement (mean, 20.30–51.98 for the internal carotid artery; 1.26–8.51 for vertebral artery). Range of differences within the 95% limit of agreement and coefficient correlation values were summarized in Table 2. Correlation of sonographic flow volume measurements of internal carotid and vertebral arteries with the measurements obtained with MR phase-contrast technique are exhibited in Figs 3A–C and 4A–C.


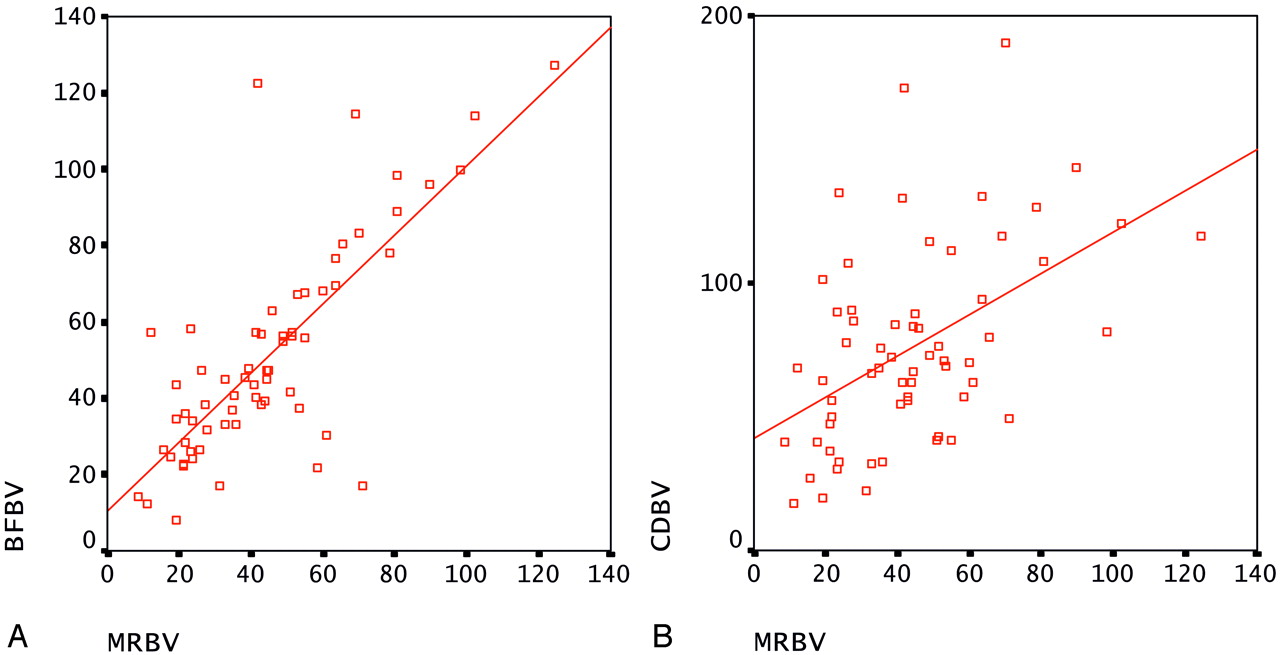
A, Graphs show correlations between sonographic and MR phase-contrast volume measurement values for internal carotid arteries. Most of flow measurements are near the line of equality indicating that BFI provides similar blood volume estimates with MR phase-contrast quantification (BFBV = blood-flow volume obtained with B-flow; MRBV = blood-flow volume obtained with MR phase-contrast imaging).
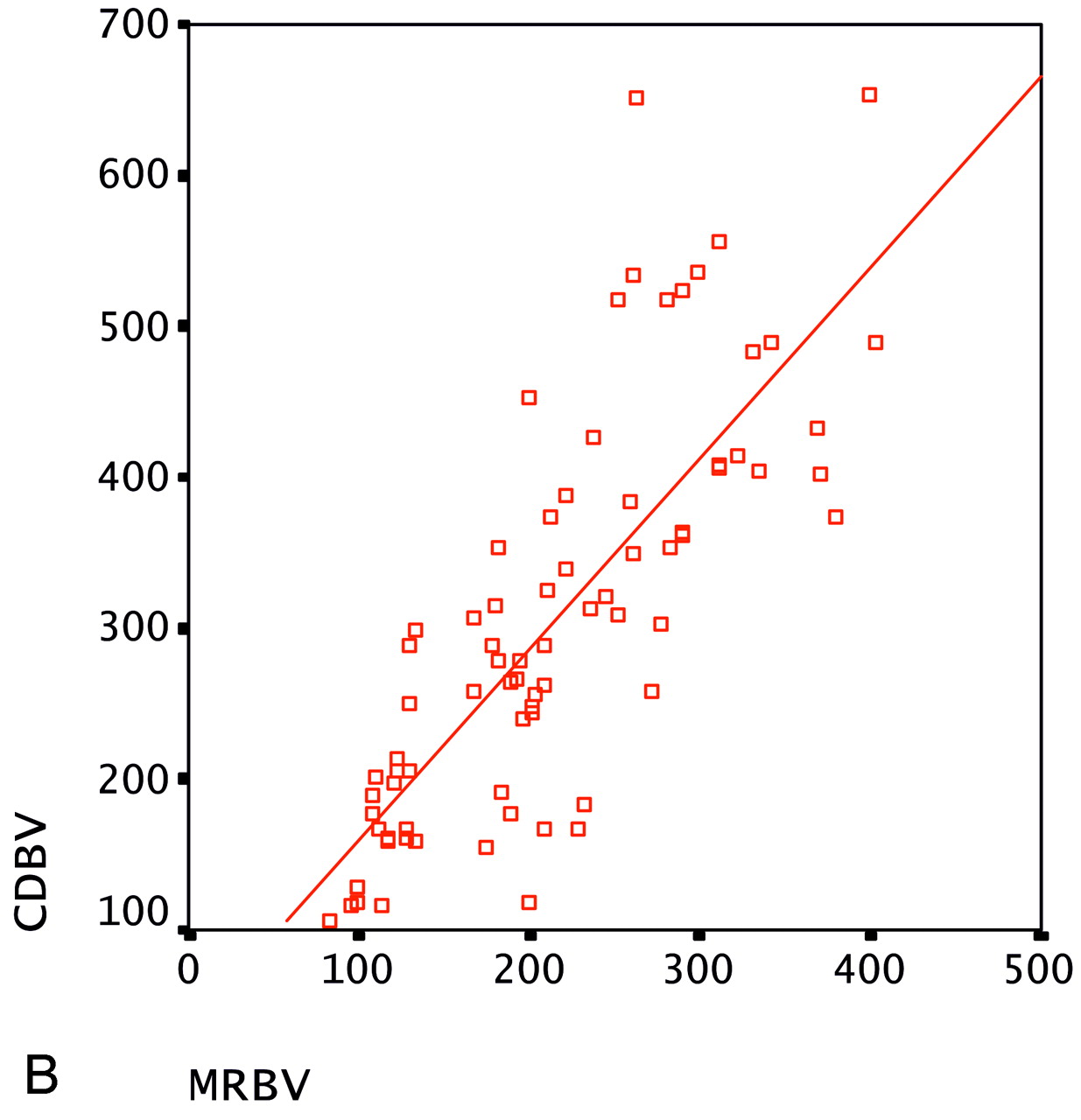
B, Correlation between flow volume measurements of internal carotid arteries obtained with CDI versus MR phase-contrast imaging is shown as scatter plot (CDBV = blood-flow volume obtained with color Doppler).
C, Correlation between flow volume measurements of internal carotid arteries obtained with PDI versus MR phase-contrast imaging is shown as scatter plot. (PDBV = blood-flow volume obtained with power Doppler).


A, Graphs show correlations between sonographic and MR phase-contrast volume measurement values for vertebral arteries. Most of volume measurements are near the line of equality indicating that BFI provides similar blood volume estimates with MR phase-contrast quantification.
B, Correlation between measurements of vertebral arteries obtained with CDI versus MR phase-contrast imaging is shown as scatter plot.
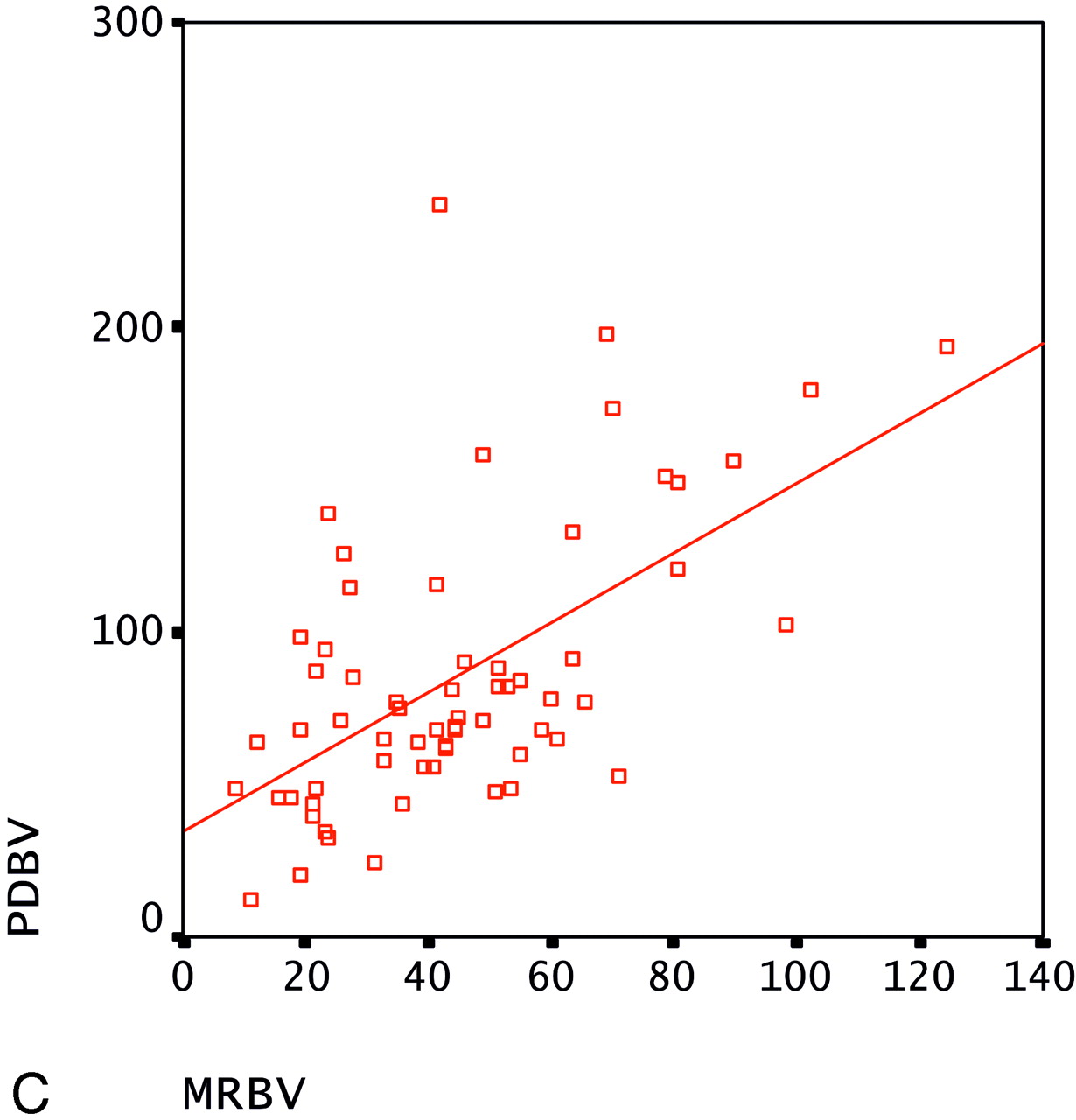
C, Correlation between flow volume measurements of vertebral arteries obtained with PDI versus MR phase-contrast imaging is shown as scatter plot.
Range of differences within the 95% limit of agreement and coefficient correlation values
Discussion
Precise quantification of cerebral blood volume with combined morphologic and hemodynamic data has many potential applications in vascular medicine, neurology, and neurosurgery. Quantification of BFV in individual arteries enables the referring physician to have more clear-cut opinions about not only the current status but also the progress of the patient already being treated. The selection of surgical candidates for carotid endarterectomy may be regarded as a potential application of cerebral blood flow quantification.
Cerebral blood flow can be assessed on the basis of the flow in capillaries or by measuring flow in the supplying vessel of the brain. Quantification of cerebral blood volume is difficult because of inherent limitations of the techniques mentioned. The electromagnetic flowmeter has been traditionally regarded as the gold standard for this purpose. It has, however, several limitations, such as its invasiveness, restriction to intraoperational application, and reported error rate of 10% caused by measuring volume and time intervals. The ionizing radiation is another concerning limitation of this technique.16
Doppler US and phase-contrast MR, which are among the most commonly used noninvasive techniques in daily clinical practice, can measure blood flow in the supplying vessels of the brain. Both Doppler US and phase-contrast MR techniques have the advantages of needing no ionizing irradiation or administration of intravenous contrast agents.17
For sonographic measurement of volume flow, duplex Doppler methods are generally introduced because, with these methods, the artery to be examined can be well delineated and chosen for interrogation. Color Doppler sonography, with adequate filtering and advanced signal intensity processing techniques, is very useful for flow imaging and can yield quantitative velocity information. Despite many advantages, color Doppler sonography has some important and limiting inherent features in visualization of dynamic pulsatile flow in major blood vessels, such as decreased spatial resolution and frame rate, as well as high angle dependency. Color Doppler images have a relatively poor spatial resolution compared with gray-scale imaging. The color picture elements are smaller in number and larger in size than the gray-scale imaging elements and the Doppler pulses are longer than imaging pulses. Both axial and lateral resolution of the color image degrades significantly because of these factors. This is of little importance when large vessels are being displayed. With small vessels, however, it may not be possible to detect flow information, or, when detected, there is almost always an overestimate of the vessel diameter. Therefore, the vessel diameter measurements from a color Doppler image may be erroneous, because the resolution of these systems is poor and the spread of color overlay leads to artifactual increase in the apparent diameter. In patients with tortuous blood vessels, artifacts of the angle of insonation may lead to errors because of less duplex Doppler data. Color information will often not be acquired at Doppler angles close to 90°. Calcified plaques in the carotid artery are another source of error, which can make the Doppler signal intensity unobtainable because of acoustic shadowing.18–20
Because of the disadvantages of color duplex flow imaging, sonographic planimetric measurement methods are used to complement duplex Doppler scanning. PDI is the most widely used among these. PDI expresses blood flow by encoding the power to Doppler signal intensity rather than the mean Doppler frequency shift. The advantage of PDI is that it is more highly sensitive to slow flow than CDI. Other advantages include the absence of aliasing and independence of the angle. It is also suggested that, because of its superior sensitivity the measurement of the vessel diameter with PDI is more accurate. PDI is very sensitive to movement, there are more flash artifacts compared to CDI, and it cannot detect flow direction. Another main disadvantage of PDI is blooming artifact.21–23 In both color and power Doppler US, the flow is presented as an overlay to the B-mode image. As a result, any tissue motion may be registered as a color flash artifact, which may obscure true flow data. Maximizing the color fill-in of vessels with low pulse repetition frequency (PRF), low wall filter, and high color gain settings will result in some overwriting of the vessel wall, which can prevent accurate estimation of the inner luminal diameter, measured between intimal layers.20 Blooming artifacts in PDI can also mask the inner intimal layer.
BFI is a recently introduced non-Doppler technology that enables real-time imaging of particulate constituents within the flowing blood. Under optimal conditions, the imaging quality and precision is comparable with digital subtraction angiography supplying a real-time picture of blood flow. In BFI, basically the echoes are subtracted from one another and the difference amplified. B-flow images are generated by using digitally encoded US technology consisting of a transmit encoder and a receive decoder in a digital beam former. The digitally encoded sound waves are transmitted through soft tissues and vessels. The returning signals are then decoded and displayed. In stationary tissue, the echoes remain the same, but in regions of moving blood there is a change from one pulse to the next. This difference is amplified to provide the display of movement. Blood flow usually cannot be seen in B-mode sonography, because weak echoes from blood cells are partially degraded due to reverberation and other artifacts. In B-mode flow sonography, however, signals from blood reflectors are enhanced while the tissue return signal intensity is suppressed, without the limitations of CDI or PDI. In BFI, a smaller number of digitally encoded wideband pulses are transmitted into the body for each scan line, compared with color imaging techniques. The need for fewer pulses along each line and high-frequency wideband pulses result in better frame rate and axial resolution than in color flow imaging. Unlike the color Doppler flow in which the color signals are superimposed onto gray-scale images, B-flow provides an unobstructed view of the vessel lumen depicting the blood echoes in a gray-scale presentation simultaneously with tissue morphology. Further advantages of BFI, in addition to higher frame rates with better spatial and contrast resolution, include fewer imaging parameters that are easier to optimize and angle independency. B-flow sonography may also be more reliable in the evaluation of small or tortuous vessels than other sonographic modalities, because the flow phenomena are less angle dependent and better demarcated against the vessel walls with simultaneous detection of flow.14,15,20,24–25
MR phase-contrast imaging is accepted as a gold standard for the quantification of cerebral blood flow.7,16,17 In our study, we compared BFV measurements obtained by 3 different sonographic methods with MR phase-contrast measurements and tried to determine which of these methods agree most with MR quantification. Phase-contrast MR imaging is one of the most commonly used imaging techniques for blood flow quantification. Both in vitro and in vivo studies have delineated the reliability of phase-contrast MR studies for accurate quantification of BFV.7–10,16,26,27 This technique enables the measurement of time-averaged blood flow and vessel area from a nongated 2D phase-contrast section with flow encoding to the perpendicular to the examined vessel. Total flow can be estimated by integrating the intravascular flow velocity over the number of cardiac cycles during data acquisition.16 As the flow velocity determined in phase-contrast MR imaging is not subject to nonuniformity problems confronted in color imaging, flow volume is more precise with this technique when compared with Doppler sonography.6 A phantom simulation study recently performed by Ho et al showed poor correlation between BFV measured with spectral Doppler imaging and phase-contrast MR imaging.16 There are also other conflicting results in the literature concerning the accuracy of blood flow measurements with color duplex imaging.5,16,11,28,29
The errors of volume flow measurement in sonographic techniques arise from inaccurate estimation of blood velocity and diameter measurement by off-axis sampling, tortuous vessels, turbulent or nonaxial flow, artifactual color signals, poor color setting, variations of vessel diameter during cardiac cycle, and respiratory vessel movement.13,29 The duplex sonography technique calculates the blood flow as the product of mean blood flow velocity and cross-sectional area of the vessel. The cross-sectional area of the vessel is usually calculated from a static vessel diameter measured at the location of the Doppler sample volume, which assumes a circular vessel configuration. On the basis of the equation of BFV measurement, any minor error in the vessel diameter measurement may dramatically alter the estimated flow volume. Overwriting of the intimal layer in color coding may cause overestimation of the vessel diameter, which is a critical parameter in calculation of BFV, as the volume formula suggests.30
In our study, we also found poor correlation between the duplex Doppler sonography technique and phase-contrast MR imaging, which may be counted as supportive evidence for the inaccuracy of this sonographic technique. BFI provided the closest values to MR phase-contrast flow quantification. The velocity measurement, which is one of the main determinants of volume measurements, did not show any statistically significant difference between different sonographic techniques. So, we can assume that the close proximity of volume measurements between BFI and phase-contrast MR arise from the more accurate measurement capability of the vessel diameter. The accuracy of BFI may be due to elimination of the sonographic artifacts such as color overwriting, aliasing, and blooming, providing better visualization of the lumen.15,20
Despite the advantages of the B-flow technique, it is not completely free of limitations. A limitation of BFI is that excessive pulsation of the vessel leads to movement of the surrounding structures and may blur the exact margins of the vessel wall. The inability to obtain signals from a structure located deep in a calcified structure is another disadvantage of BFI, as with classical sonography imaging techniques. It is often possible, however, to obtain alternative views of the same portion of the artery with good insonation angles and allow the artery to be interrogated by Doppler spectral analysis. Further disadvantages include decreased sensitivity with increased depth, difficulty demonstrating slow flow, and background flash artifacts.14 We had to exclude flow measurements of 4 vertebral arteries of 2 subjects from our study in which no signal intensity could be obtained with BFI, probably because of the deep locations of these vessels and slow flow. The operator dependency, which is among the one of the most concerning disadvantages of sonographic examination, also applies to B-flow sonography.
There are some drawbacks in our study. Flow quantification in subjects is more challenging than in vitro studies because of technical difficulties arising from personal physiologic changes. Therefore, a complete correlation among these 4 techniques would be highly unusual. In addition, this study has been performed in young healthy individuals; there are imaging difficulties in patients having vascular pathology, tortuosity, arrhythmia, cervical osteoarthritis, or in patients with poor general condition. Depending on our clinical experiences, however, we believe that BFI could be helpful in flow quantification of such patients. Further studies are needed to evaluate the applicability of B-flow method in patients who are difficult to image.
In our study, BFI showed the closest values to phase-contrast MR, which is accepted as an accurate volume quantification method. With these findings, we can conclude that BFI is the most reliable sonographic technique for the quantification of cerebral BFV, suggestively due to more accurate measurement of real inner diameter of the vessel with its ability to eliminate artifacts such as aliasing, overwriting, and blooming.
Low operational costs, bedside applicability, and potential use in the monitoring of critically ill patients are among the other advantages of this technique. With all these advantages, we think that BFI may be a highly promising and reliable alternative approach to phase-contrast MR in the estimation of cerebral BFV.
Acknowledgments
We express our gratitude to Reyhan Yilmaz for her technical assistance and to the participants who served as volunteers.
References
- Received March 24, 2005.
- Accepted after revision July 23, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of haemodynamics on the risk of ischaemic stroke in patients with severe vertebral artery stenosis
- Comparison of Transcranial Doppler Ultrasound with Computational Fluid Dynamics: Responses to Physiological Stimuli
- Effect of cervical manipulation on vertebral artery and cerebral haemodynamics in patients with chronic neck pain: a crossover randomised controlled trial
- What to do about fibrin rich 'tough clots? Comparing the Solitaire stent retriever with a novel geometric clot extractor in an in vitro stroke model
- Aneurysmal Parent Artery-Specific Inflow Conditions for Complete and Incomplete Circle of Willis Configurations
- REPLY:
- Internal Carotid Artery Hypoplasia: Role of Color-Coded Carotid Duplex Sonography
- Dampening of Blood-Flow Pulsatility along the Carotid Siphon: Does Form Follow Function?
- Velocity Measurements in the Middle Cerebral Arteries of Healthy Volunteers Using 3D Radial Phase-Contrast HYPRFlow: Comparison with Transcranial Doppler Sonography and 2D Phase-Contrast MR Imaging
- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents
- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents
- Blood volume flow quantification of the brain-supplying circulation in fibromuscular dysplasia using 2D cine phase-contrast MRI