
Abstract
BACKGROUND AND PURPOSE: Isolated dissecting aneurysms of the posterior inferior cerebellar artery (PICA) carry a high risk of rebleeding with an associated increased mortality rate. Although rare, they present a therapeutic challenge. Surgical treatment carries a significant risk of neurologic complications, predominantly lower cranial nerve deficits because of the close relationship of the aneurysm with the brain stem and cranial nerves. The purpose of this article is to show that endovascular treatment of dissecting aneurysms of the PICA can be effective and can allow the patient to avoid the complications associated with surgery.
METHODS: Six patients (age range, 28–70 years) with dissecting aneurysms of the PICA were treated at our center by endovascular occlusion with Guglielmi detachable coils or glue and followed for up to 30 months. Inclusion of patients in the study was based on careful angiographic assessment of the vascular anatomy and collateral supply of the posterior fossa. When on the basis of the anatomy, potential lack of sufficient collaterals was suggested, a test occlusion was performed to determine the feasibility of an endovascular approach. Four additional cases, which have been described in the literature, were included in the analysis of results.
RESULTS: In all patients, the aneurysm was successfully occluded with no apparent procedure-related complications. Follow-up studies showed stable and complete occlusion of the aneurysm in all patients with no long-term neurologic deficits.
CONCLUSIONS: Endovascular treatment by aneurysm and parent artery occlusion is a relatively safe and reliable alternative to surgery for isolated dissecting aneurysms of the PICA.
Aneurysms of the posterior inferior cerebellar artery (PICA) are uncommon, accounting for 0.5%–1% of all intracranial aneurysms. Most arise near the origin of the PICA from the vertebral artery.1,2 Isolated dissecting aneurysms of the PICA are rare.2–13 Traditionally, surgical treatment included surgical wrapping, clip ligation, or trapping (with or without anastomosis)2,3,7,8,10–13; however, these surgical procedures carry a high risk of neurologic complications due to the proximity of the aneurysm to vital structures such as the brain stem and cranial nerves.14 Recently, endovascular treatment has been proposed as an alternative to surgery.5,10,12,15,16
There are only 4 reported cases in the medical science literature of endovascular treatment of isolated dissecting PICA aneurysm.5,10,15,16 We present our experience with endovascular treatment of 6 additional dissecting PICA aneurysms by occlusion of the aneurysm and parent artery. To our knowledge, this is the largest reported series of such cases.
Patients and Techniques
Between January 1999 and December 2004, 260 patients with 330 intracranial aneurysms were treated in our tertiary referral center. Six patients had isolated dissecting PICA aneurysm. All 6 were treated by an endovascular approach.
Demographic details, clinical presentation, grading of subarachnoid hemorrhage (Hunt and Hess scale), imaging findings, postprocedure course, and complications were recorded. Nondissecting aneurysms and dissecting aneurysms associated with arteriovenous malformation were excluded. We added the data of 4 additional cases of isolated PICA dissecting aneurysm treated by endovascular embolization, reported in the National Library of Medicine data base from 1966 to 2003.5,10,15,16
Endovascular Treatment
Diagnosis and endovascular treatment were performed in our neuroradiology interventional suite, equipped with a Philips biplane digital unit (Philips Medical Systems, Bothell, Wash) with road-mapping and 3D capabilities. The procedures were performed with the patient under general anesthesia and monitored by using pulse oximetry and electrocardiography.
Vascular access was obtained via the common femoral artery. A 6F guiding catheter (Cordis, Miami Lakes, Fla) was introduced through a femoral sheath to the vertebral artery. A diagnostic angiogram was obtained to define the vascular anatomy of the posterior fossa and assess collateral supply from the anterior inferior cerebral artery (AICA) and superior cerebellar artery (SCA). On the basis of the anatomy, an estimate of each individual patient’s ability to tolerate occlusion of the PICA was made. We reviewed the angiogram carefully to determine whether the aneurysm involved a dominant PICA, to identify an ipsilateral accessory PICA when present, and to verify that the size of both AICAs and the ipsilateral SCA was sufficiently large to provide collateral flow. Because no data are available on angiographic signs to predict that an occlusion of the PICA would be tolerated, our estimate was based on generally accepted principles with other similar vascular abnormalities and personal experience. In our opinion, if the ipsilateral AICA is greater than, equal to, or more than approximately half the size of the PICA, occlusion of the vessel would not be associated with significant sequelae. In those cases in which the AICA was absent or was less than half the size of the PICA, a test occlusion was performed.
Following the diagnostic study, a Prowler 10 microcatheter (Cordis) was advanced coaxially through a 6F guiding catheter to the proximal part of the vertebral artery, with the aid of a Transcend Platinum 10 guidewire (Boston Scientific, Fremont, Calif), and then into the aneurysmal dissecting segment. Ultrasoft Guglielmi detachable coils (GDC) (Boston Scientific) were inserted into the diseased segment. Short, soft, and ultrasoft coils were used to reduce the pressure changes on the fragile wall of the aneurysmatic segment. A control angiogram was obtained at the end of the procedure to verify occlusion of the aneurysm and filling of the territory of the artery distal to the aneurysm by collaterals.
A CT scan was obtained within 24 hours of the procedure. All patients underwent postoperative evaluation in the Neurosurgical Intensive Care Unit. Patients were assessed clinically over a period of 6–18 months in the appropriate outpatient clinics.
Our routine imaging follow-up consisted of conventional angiography or MR angiography (MRA) performed between 3 and 6 months and at 15 months following treatment, provided that the patient remained asymptomatic. If no evidence of recurrent aneurysm was detected, further follow-up was not required. Three cases (cases 1, 2, and 4 in the Table) were followed with MRA, and 3 cases (cases 3, 5, and 6) were followed with digital subtraction angiography (DSA).
Clinical and angiographic data for patients with dissecting posterior inferior cerebellar artery aneurysms
In 2 cases (cases 1 and 2 in the Table) that involved the lateral medullary segment, the coils were inserted so that the dissecting part and only a very short segment of the normal artery proximal to it were occluded. We ascertained that the anterior medullary segment that has important perforators supplying the brain stem remained patent (Fig 1). To prevent progression of thrombosis, intravenous bolus injection of 40 IU/kg per hour of heparin was administered as soon as the first coil was placed, and the activated clotting time was maintained at double the normal range for 12 hours.

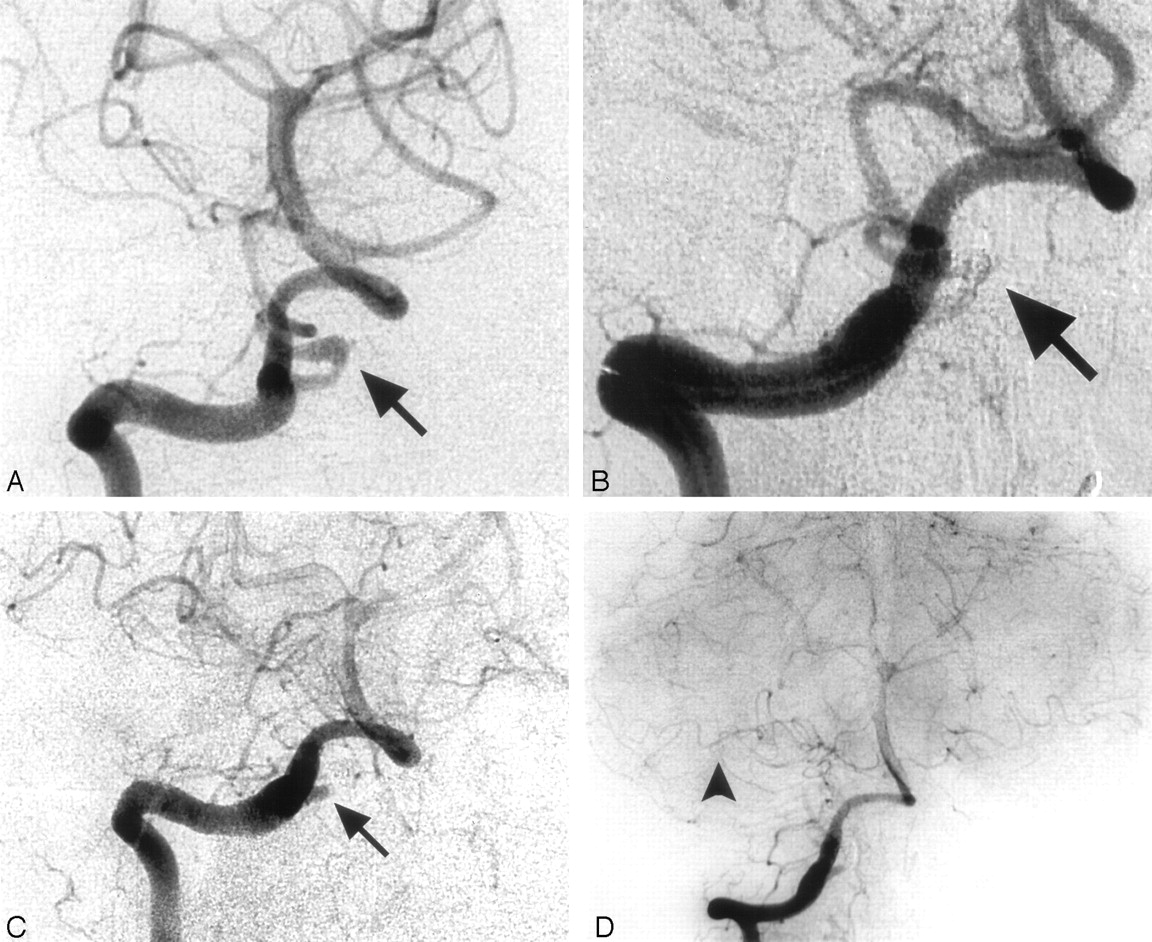
Case 1. Images of a 48-year-old woman with a dissecting aneurysm of the right PICA.
A, Angiogram shows a dissecting aneurysm arising from the lateral medullary segment of the right PICA (arrow).
B, Angiogram obtained after embolization of the dissecting aneurysmatic segment with coils (arrow).
C and D, Control angiogram shows complete obliteration of the dissecting aneurysmatic segment with preservation of the anterior medullary segment (arrow, C) and distal filling from the AICA (arrowhead, D).
In 2 cases (cases 2 and 4), we performed a test occlusion while the patient was under general anesthesia. The signs that were used to determine whether the patient “passed” or “failed” the test were visualization of collateral filling during the arterial phase and/or venous opacification and washout in the territory in question. A delay of more than 2 seconds in venous opacification indicated that the blood supply was insufficient. In case 2 with an apparently small AICA, we performed a balloon test occlusion to evaluate the blood flow from the accessory PICA to the artery distal to the dissection. A nondetachable silicone balloon was placed in the parent vertebral artery at the origin of the PICA. The test showed that there was sufficient blood supply from the accessory PICA distally to enable occlusion. In case 4, in which the dissecting aneurysm involved an AICA-PICA configuration (Fig 2), we performed selective occlusion of the vessel just proximal to the diseased segment by using a GDC coil. The patient failed the test; therefore, only the aneurysmal part was occluded. We took into consideration the likely possibility of reopening of the aneurysm; however, we expected that collaterals would enlarge with time. The patient was closely followed and 3 months after the procedure, MRA demonstrated reopening of the aneurysm. A repeat selective vessel test occlusion showed that there were enough collaterals to enable occlusion of the dissected segment, and re-embolization was successfully performed by using coils.


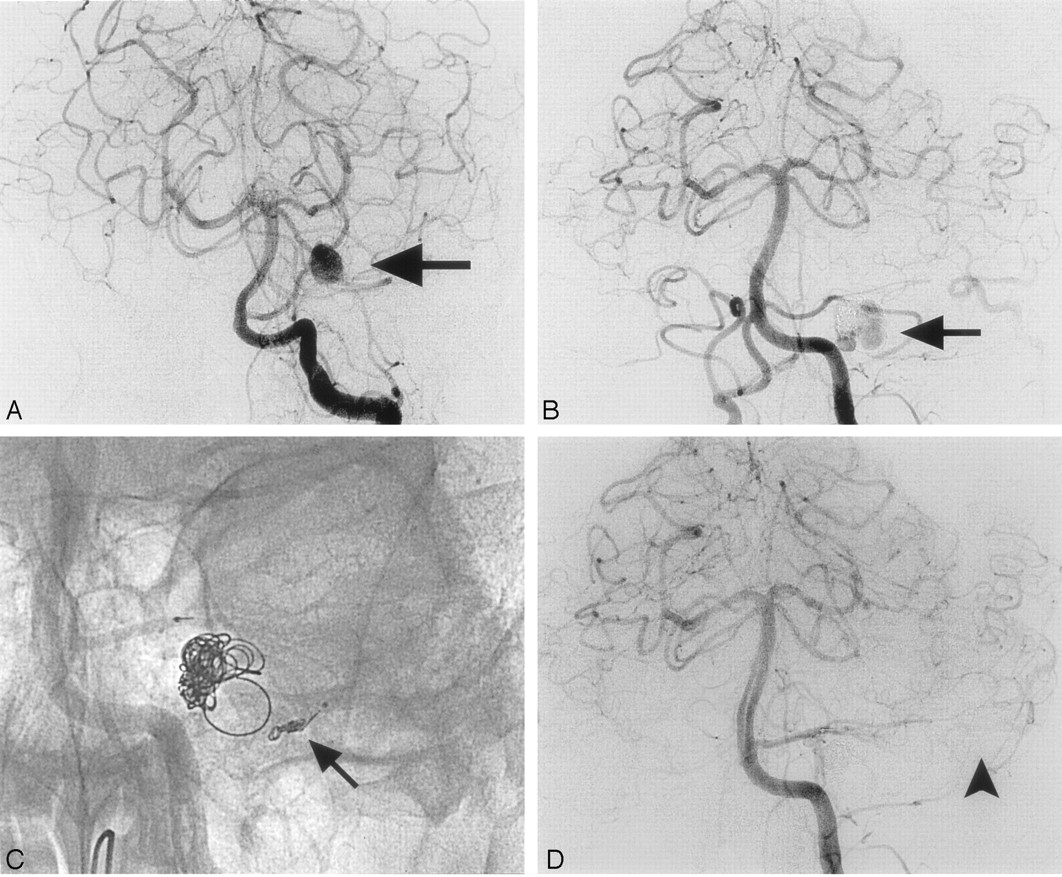
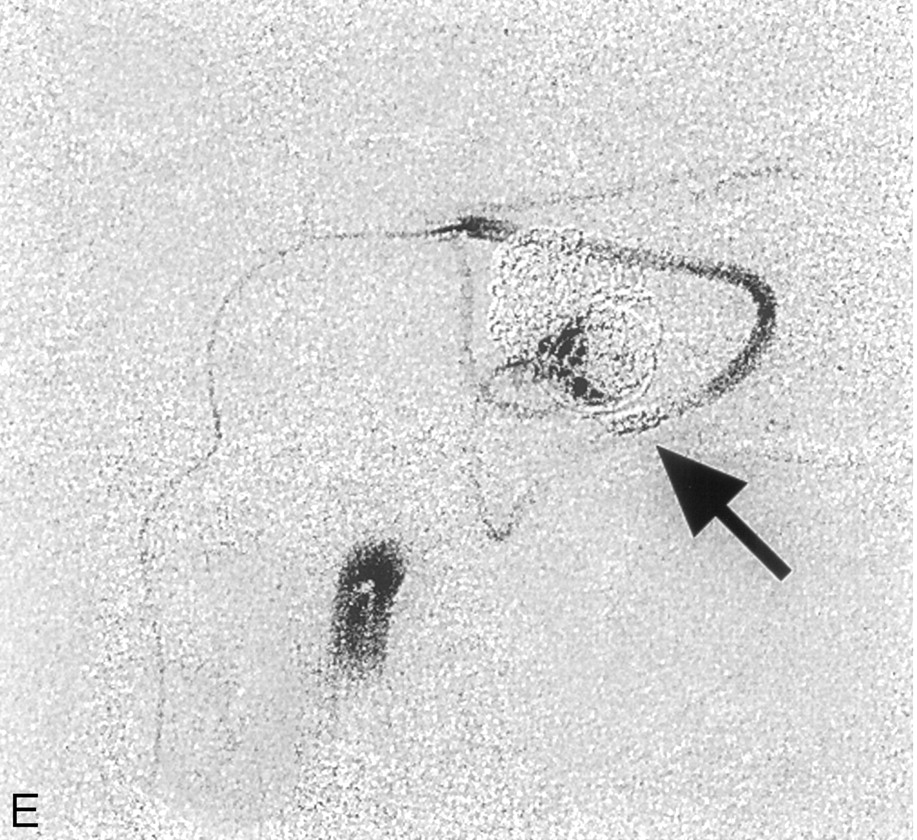
Case 4. Images of a 33-year-old man with a dissecting aneurysm of a left AICA-PICA configuration.
A, Angiogram shows dissecting aneurysm arising from a hemispheric branch of a left AICA-PICA (arrow).
B, Angiogram obtained 3 months after embolization shows reopening of the aneurysm (arrow).
C and D, Selective test occlusion by using a GDC coil (arrow) shows distal filling via collaterals (arrowhead, D).
E, Selective injection to the PICA shows the location of the GDC coils used for the test occlusion (arrow).
In 1 case (case 6), the aneurysm involved the vermian segment. Because of the distal location of the aneurysm and its small size, embolization with detachable coils would have been difficult. The therapeutic approach in this case was to occlude both the aneurysm and a short segment of the proximal parent vessel by injection of glue. A mixture of 25% tissue adhesive (Histoacryl, B. Braun, Melsungen, Germany) and 75% iodized oil (Lipidol, Andre Guerbert, Aulnay sous Bois, France) was prepared in a syringe, and a total of 0.2 mL was slowly injected just proximal to the dissecting segment.
Results
In the 6-year period between 1999 and 2004, we treated 6 patients with isolated dissecting aneurysm of the PICA by the endovascular approach. Another 4 similar cases were published in the English language literature.5,10,15,16 The Table shows the data recorded from the medical files and imaging studies (cases 1–6) and the previously published reports. There were 5 women and 5 men (age range, 28–70 years). Eight of 10 patients presented with subarachnoid hemorrhage, confirmed by CT. Hunt and Hess grading at admission was as follows: grade I, 1 patient (case 4); grade II, 3 patients (Tikkakoski et al15 and cases 1 and 6); grade III, 2 patients (Yamaura et al16 and case 5); and grade IV, 2 patients (cases 2 and 3). No grade was documented in the remainder. In 5 cases, the aneurysm was located on the left side, and in 5, on the right. Anatomically, 3 aneurysms were found in the lateral medullary segment (Lefkowitz et al10 and cases 1 and 2), 4 in the vermian segment (Dinichert et al5 and cases 3, 5 and 6), and 1 in a hemispheric branch (case 4). In 2 cases (Tikkakoski et al and Yamaura et al), no information was available. Aneurysm size ranged from 3 to 15 mm in the longest axis.
Two of our patients (cases 2 and 3) presented with hydrocephalus that required placement of a ventriculostomy. All aneurysms were successfully treated on the first attempt, except for case 4, in which the aneurysm reopened at 3 months and was then successfully occluded.
In all patients, a control angiogram obtained on completion of the procedure demonstrated complete occlusion of the diseased segment, with normal blush and distal filling by collaterals from the AICA, SCA, or accessory PICA (Figs 1 and 2). All patients were clinically stable in the immediate postprocedural period, and the duration of hospitalization in 5 of the 6 patients treated in our center was no more than 7 days. Case 2 was an elderly patient who developed hydrocephalus due to intraventricular hemorrhage before the endovascular procedure. He required an extended hospital stay of 62 days due to complicating infection (ventriculitis and pneumonia).
No procedure-related complications were evident on CT performed within 24 hours after treatment. Follow-up angiographic studies showed stable and complete occlusion in all cases. Among the cases described in the literature, 2 patients had transient postprocedural neurologic deficits: the first (Lefkowitz et al10 ) had mild left-sided dysmetria, and the second (Tikkakoski et al15 ) had mild symptoms of hemisensory loss. Both resolved in 2 days. There were no long-term neurologic deficits.
Discussion
PICA aneurysms may be classified into saccular and fusiform types. Fusiform aneurysms are spindle-shaped and arise spontaneously anywhere along the course of the vessel, mainly as a consequence of dissection. Saccular aneurysms typically arise at bifurcations.
Patients with isolated dissecting PICA aneurysms tend to present clinically in 2 ways, though some overlap may occur. Approximately half of all affected patients present with signs and symptoms of subarachnoid hemorrhage (sudden headache, neck pain, vertigo, nausea, vomiting, transient loss of consciousness, or coma). The other half present with symptoms of ischemia, such as Wallenberg syndrome.5,17 All our patients presented with subarachnoid hemorrhage with or without intraventricular hemorrhage.
Patient age ranged from 20 to 70 years, with most in their fourth decade of life.17 Men and women are equally affected.5,17
The cause of dissecting aneurysm of the PICA is unknown. No predisposing factors such as trauma, migraine, Moyamoya disease, Marfan syndrome, angiitis, or homocystinuria have been reported,8 though some authors suggest that hypertension found in 1 of our patients (case 6) may play an underlying role.17
CT and MR imaging may show subarachnoid/intraventricular hemorrhage and/or infarction. Subarachnoid hemorrhage is usually found in the posterior fossa, basal cisterns, or fourth ventricle and may extend into the third and lateral ventricles, resulting in hydrocephalus (as in cases 6 and 7). On angiography, the dissection may appear as a string or pearl and string (indicating a smooth tapered stenosis related to the aneurysm), segmental narrowing, occlusion of the vessel, or a “double lumen” (very rare). In our patients, the initial angiogram revealed a slight, irregular dilation of the PICA with typical pearl and string sign.
Dissecting aneurysm of the PICA carries a 24% risk of rebleeding in the acute phase, associated with a high mortality rate.16 Early intervention is essential; however, management remains controversial. Generally, surgery includes proximal clipping, trapping, and wrapping or resection with PICA end-to-end anastomosis, PICA-to-occipital artery anastomosis, or PICA reimplantation to the vertebral artery. However, manipulating the proximal PICA for clipping poses a high risk of postoperative neurologic morbidity because of the close relationships with the brain stem and lower cranial nerves.4,6,14
There are 24 cases of isolated dissecting PICA aneurysm reported in the literature. Endovascular treatment is reported in only 4 of these cases; however, it is gaining popularity because of improvements in imaging techniques and treatment tools.
Lewis et al11 reported a surgical success rate of only 70% in 20 patients with PICA aneurysm, and Horowitz et al6 reported 66% postoperative neurologic morbidity. In at least half of these cases, morbidity was related to cranial nerve palsy. Analogously, Lee et al9 noted 64% perioperative morbidity in 14 patients, 21% with lower cranial nerve deficits. Andoh et al4 found that surgical treatment of aneurysms located in the vertebral artery near the origin of the PICA often caused cranial nerve deficit.
Because endovascular procedures do not involve manipulation of brain stem, cranial nerves, or cerebellar tissue, the complications noted previously may be avoided. Thus, such procedures are gaining in popularity among clinicians.5,10–13,15,16 Lefkowitz et al10 was the first to describe the successful endovascular embolization of an isolated dissecting aneurysm of the PICA in a 45-year-old patient. Yamaura et al16 reported endovascular occlusion with detachable coils in 6 patients with a ruptured dissecting aneurysm in the posterior fossa (5 in the vertebral artery and 1 in the PICA) and concluded that the procedure was reliable and safe.
In both surgical and endovascular treatment, the diseased segment is trapped; perforating vessels in that area are sacrificed. The argument in support of surgical treatment is based on the ability in surgery to create anastomosis that will bridge the diseased segment. Anatomical studies and surgical experience18 however indicate that in most patients with PICA dissection, good collateral flow exists and creating a vascular anastomosis to supply the area distal to the trapped segment is unnecessary. The few patients who might benefit from surgery can be identified by careful angiographic study with or without test occlusion.
The PICA supplies blood to the caudal medulla, cerebellar tonsils, inferior portion of the cerebellar hemisphere, vermis, and choroid plexus of the fourth ventricle. Endovascular treatment involves occlusion of the parent artery and can potentially result in neurologic deficit. We therefore performed angiography before treatment to delineate the vascular anatomy of the posterior fossa and assure the presence of appropriate flow from collateral vessels via the AICA and SCA. The exact location of the dissection was identified, and assessment of size of the vessels in the posterior fossa and their relationship with the dominant PICA was performed. In case 8 in which the aneurysm was located in an AICA/PICA variant and in case 6 in which a large dominant PICA was associated with a small AICA, occlusion carried a higher risk of cerebellar damage. In these cases, a test occlusion was performed with careful consideration of alternative surgical treatment. We followed the advice of Professor Salomon, who stated that “… anastomosis serves only to collateralize circulation to the hemispheric branch of PICA and does nothing to compensate for the loss of perforators in the segment of PICA that is trapped. The effect of the superficial cortical infarct produced by occlusion of distal PICA is usually not clinically significant.”18
The advancement in endovascular tools that are now available enables us to accurately select the length of segment for occlusion with an accuracy similar to that in surgical trapping. We were able to occlude the diseased segment while maintaining the segment proximal to it, thus minimizing damage to brain stem perforators.
Endovascular treatment was successful in all cases, with no aneurysmal bleeding, persistent neurologic deficits, or signs of infarction, and no procedure-related complications. CT and clinical examination are insensitive in detecting small areas of ischemia in the posterior fossa. Long-term imaging follow-up showed complete obliteration of the dissecting aneurysms (Table).
Conclusion
Endovascular treatment of isolated dissecting PICA aneurysms may be a safe and effective alternative to surgery provided that vessel occlusion can be tolerated, as determined by the preprocedure angiographic demonstration of adequate collateral circulation. Additional studies are warranted to establish the criteria and indications for this therapeutic approach and to document its advantages compared with surgery.
References
- Received April 11, 2005.
- Accepted after revision August 14, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular sacrifice of the proximal posterior inferior cerebellar artery for treatment of ruptured intracranial aneurysms
- Endovascular rescue treatment through stent positioning after surgical clipping of intracranial aneurysms complicated by parent artery obstruction
- Endovascular treatment of posterior inferior cerebellar artery aneurysms: a 7-year single-center experience
- Onyx embolization in distal dissecting posterior inferior cerebellar artery aneurysms
- Endovascular treatment of ruptured dissecting aneurysms of the posterior inferior cerebellar artery
- Dissecting Aneurysms of the Distal Segment of the Posterior Inferior Cerebellar Arteries: Clinical Presentation and Management