
Abstract
SUMMARY: Two patients with a chronic progressive myelopathy were successfully surgically treated and idiopathic hypertrophic spinal pachymeningitis (IHSP) was found on histology. In both patients, an extensive extramedullary mass of low T2 signal with peripheral contrast enhancement was compressing the spinal cord on MR imaging. This imaging appearance in patients with chronic progressive myelopathy should suggest the diagnosis of IHSP.
Idiopathic hypertrophic spinal pachymeningitis (IHSP) is a rare inflammatory disorder that leads to spinal cord compression. We present 2 cases of this condition with a description of MR imaging findings.
Case Reports
Case 1
A 47-year-old woman presented with a 2-year history of truncal and lower extremity weakness, numbness from the nipple line down to the feet, bowel and bladder incontinence, and increased reflexes in her lower extremities. Imaging was not performed at the initial presentation. The symptoms almost completely resolved after a year without treatment but then started progressing again.
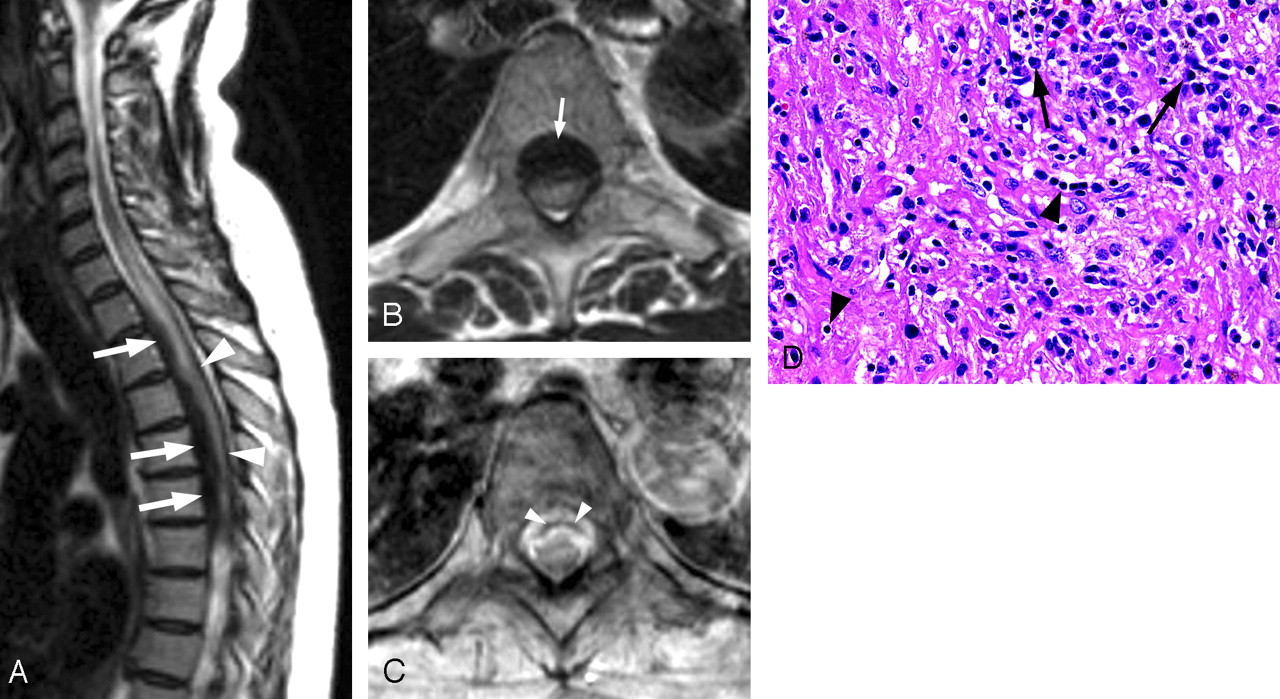
MR imaging of the thoracic spine demonstrated an anterior extramedullary mass extending from T1 to T6 level that was of low T1 and T2 signal intensity with predominantly peripheral enhancement (Fig 1, A–C). The mass was compressing the spinal cord with resultant cord edema. Complete imaging of the neuroaxis was not performed.

A, Sagittal fast spin-echo (FSE) T2-weighted image of the cervical and upper thoracic spine shows a mass of very low signal intensity (arrows) within the spinal canal located adjacent to the posterior aspect of the T1 through T6 vertebral bodies. High signal intensity is present centrally within the spinal cord, indicative of cord edema. There is also thickening and hypointensity of the dura posterior to the spinal cord (arrowheads).
B, Axial FSE T2-weighted image at T5 level shows a hypointense mass (arrow) in the anterior aspect of the spinal canal that appears to be arising from the dura. The lesion is displacing the spinal cord posteriorly and completely effacing the intradural subarachnoid spaces.
C, Axial postcontrast T1-weighted image at a level similar to that of B reveals thick enhancement of the anterior epidural mass with central nonenhancing area (arrowheads).
D, Photomicrograph shows fibrosis with plump reactive fibroblasts. Chronic inflammatory infiltrate is consisting chiefly of plasma cells (arrows) with additional lymphocytes (arrowheads) and scattered histiocytes (macrophages) (hematoxylin and eosin, original magnification 40×).
After T1–T6 laminectomy, a firm tissue adherent to the ventral dura was found compressing the spinal cord, located in both intradural and extradural space. Multiple biopsy specimens were taken, but a complete resection could not be performed. A dural patch was placed posteriorly to expand the thecal sac. Chronic inflammation with fibrosis and lymphoplasmacytic infiltrate was found on histology (Fig 1D). There was a steady significant postoperative recovery and the patient was eventually able to ambulate with normalized bladder and bowel function.
Case 2
A 68-year-old woman presented with a 2-month history of progressive lower and upper extremity weakness and urinary retention, bilaterally decreased sensation in lower extremities, and a poor rectal tone. A lower cervical laminectomy had been performed several years earlier, when the resected tissue was considered a “benign spinal tumor,” according to the available reports.
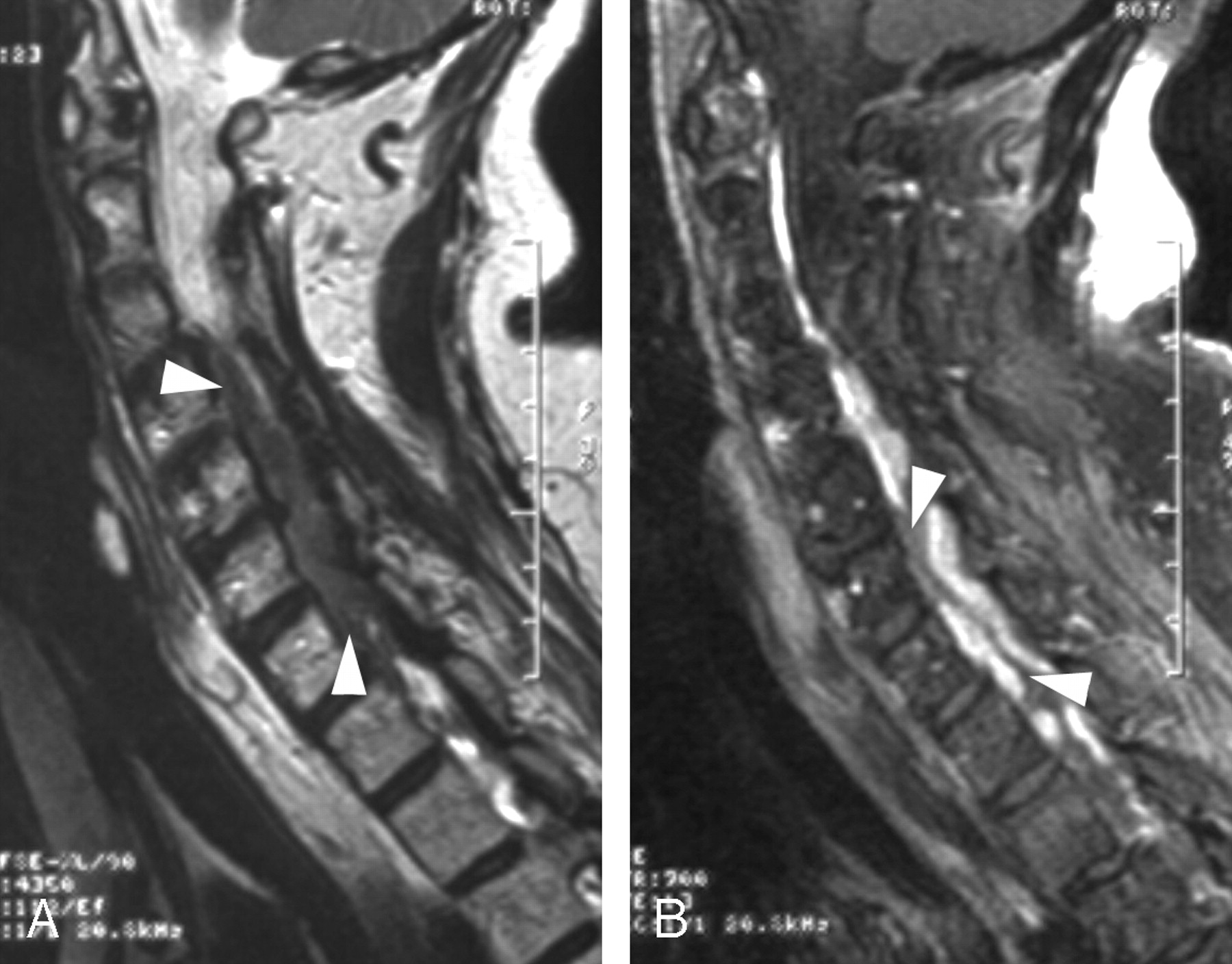
MR imaging showed an extramedullary mass encompassing and compressing the spinal cord, hypointense on T2-weighted and isointense on T1-weighted images with attenuated, predominantly peripheral enhancement (Fig 2). Imaging of the complete neuro-axis revealed no additional abnormalities. The patient was initially treated with corticosteroids and had minimal improvement. After C6–C7 laminectomy, a large amount of intradural granular tissue attached to the dura was encountered and resected. No extradural abnormality was visible from a dorsal surgical exposure. Histology demonstrated fibrosis with chronic inflammatory reaction. The patient slowly recovered most of the neurologic deficits.

A, Sagittal fast spin-echo (FSE) T2-weighted image shows a hypointense mass (arrowheads) in the anterior aspect of the spinal canal that extends from C3 to T1 level.
B, Corresponding sagittal postcontrast T1-weighted image with fat suppression reveals attenuated enhancement of the mass, which is predominantly peripheral with central nonenhancing portions (arrowheads).
Discussion
Idiopathic hypertrophic pachymeningitis (IHP) is a chronic progressive diffuse inflammatory fibrosis of the dura mater.1–4 This rare disorder is usually found intracranially and is a diagnosis of exclusion because meningioma, lymphoma, tuberculosis, sarcoidosis and other diseases may present in a very similar fashion.1–5 It has been proposed that Tolosa-Hunt syndrome may represent a focal manifestation of IHP.6
The spinal form is extremely rare, with few described cases, though the first report by Charcot dates back to 1869.7–13 It presents as a chronic progressive disease with manifestations of radiculopathy, myelopathy, or a combination of both, attributable to the compression of neural structures or vascular compromise. It occurs alone, usually involving the cervical and thoracic dura or as a craniospinal form.1,8–13 Corticosteroids have been considered the mainstay of conservative treatment; however, relapses are common, and azathioprine and cyclophosphamide have been tried with some success.1 Decompression provides relief, and early surgical intervention can successfully alleviate neurologic sequelae.8–12
On MR imaging, IHSP has been described as a dural-based mass of low T2 signal intensity extending over multiple levels with strong enhancement; the linear enhancement pattern appears to show better therapeutic response than the nodular form, possibly related to less fibrosis and more vascularity.8–12 Friedman and Flanders13 described the peripheral enhancement that was present in all 3 patients as highly suggestive of hypertrophic pachymeningitis, which was also noted in another report.14 This pattern is presumably caused by a peripheral zone of active inflammation along the lesion periphery, in contrast to attenuated fibrosis throughout the central portions.13, 14 In addition to fibrosis of the meninges, histology shows inflammatory cell infiltration, which is composed mainly of lymphocytes and plasma cells, especially at the surface of the dura mater.2, 3 We reviewed the MR images of published cases and noted that this peripheral enhancement was present in 12 of 14 patients.8–18 The characteristics of reported cases are summarized in the Table. We propose that a long extramedullary mass of low T2 signal intensity with peripheral enhancement represents a specific MR imaging finding that is highly suggestive of IHSP. The specific features of the cases we presented are spontaneous temporary resolution of symptoms and disease recurrence after surgery.
Characteristics of reported cases of idiopathic hypertrophic spinal pachymeningitis (IHSP) that included MR imaging findings
References
- Received February 23, 2006.
- Accepted after revision April 12, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}