
Abstract
SUMMARY: One case report of a schwannoma involving the sympathetic plexus in the carotid canal has been reported previously. This article presents 2 additional cases of this rare entity with associated clinical and unique radiographic findings. All patients presented with diplopia among other symptoms, and they had enhancing masses that smoothly expanded the carotid canal on cross-sectional imaging. Comparison with the index case and differential diagnosis of more common pathologies in this area are discussed.
Abbreviations
- ICA
- internal carotid artery
The most common nerve sheath tumor is the schwannoma. It may arise from any peripheral, cranial, or autonomic nerve. Nearly 45% of schwannomas occur in the head and neck, and comprise 9% of skull base tumors.1 The most common intracranial schwannomas arise from the vestibular nerve and less commonly from the trigeminal nerve or the nerves of the jugular foramen. Less than 75 cases of sympathetic plexus schwannoma have been reported in the cervical region,2,3 and it has only been reported once to occur in the carotid canal at the skull base and cavernous sinus.4,5 The most common schwannoma in the cavernous sinus is the trigeminal, with rare reports of schwannomas arising from the occulomotor, trochlear, and abducens nerves.5
Schwannomas are slow-growing tumors that arise from the perineural or Schwann cells within the perineural sheath eccentric to the nerve root, as originally described by Verocay.6,7 Most of these tumors are benign and solitary, though malignant cases have been reported previously.8 Neurofibromatosis type II patients have an increased rate of schwannoma formation as well as meningiomas and ependymomas9 and involve a deletion of the long arm of chromosome 22. They are also at increased risk for malignant degenerations but less so than the peripheral nerve sheath tumors of neurofibromatosis type I.9
An important part of understanding schwannomas is knowledge of the anatomic pathways of the nerves that they follow and distort. The carotid canal encompasses the petrous and cavernous portion of the internal carotid artery. The petrous portion of the carotid canal has a relatively simple differential diagnosis for pathology because it only has bone, sympathetic nerves, and blood vessels in the region. The cavernous portion can have numerous pathologies due to the proximity of many varying tissues, including blood vessels, nerves, dura, bone, the pituitary gland, and additional tissues that could be incorporated during embryologic formation. The most common mass of the cavernous region is a meningioma, followed by pituitary adenoma and trigeminal schwannoma. Rare cases of epidermoid tumors, plasmacytomas, and bone and blood vessel tumors have been reported previously.5 Other considerations include vascular lesions such as aneurysms and extension of other skull-based tumors such as metastasis and lymphoma.
The sympathetic chain surrounding the ICA is composed of postganglionic fibers derived from sympathetic fibers primarily from the superior cervical ganglion. It has 2 parts: the internal carotid plexus and the cavernous plexus. The internal carotid plexus is lateral to the ICA and has branches to cranial nerves V and VI and the wall of the ICA. In addition, there are branches to the tympanic branch of the glossopharyngeal nerve, known as the caroticotympanic nerve, that project to the cochlear promontory and branches of the deep petrosal nerve that contribute fibers to form the pterygoid (Vidian) nerve. The cavernous plexus is medial to the ICA and has branches to cranial nerves II, III, IV, and VI, including the ciliary ganglion, and it is involved in pupillary response as well as the vasomotor rami to the pituitary gland.4,10
To date, there has only been 1 case report of a schwannoma involving the sympathetic plexus in the carotid canal at the skull base.4 This article presents 2 additional cases of this rare entity and discusses the more common differential diagnosis.
Case Presentations
Patient 1
A 27-year-old Hispanic woman presented with 2 weeks of hearing loss secondary to a middle ear effusion. The patient had relief of her symptoms after placement of a tympanostomy tube. The patient subsequently developed 4 months of headache and 2 weeks of diplopia. There was no relevant personal or pertinent family history. On physical examination, the patient was found to have a left abducens palsy with an otherwise intact extraocular muscle movement and facial sensation.
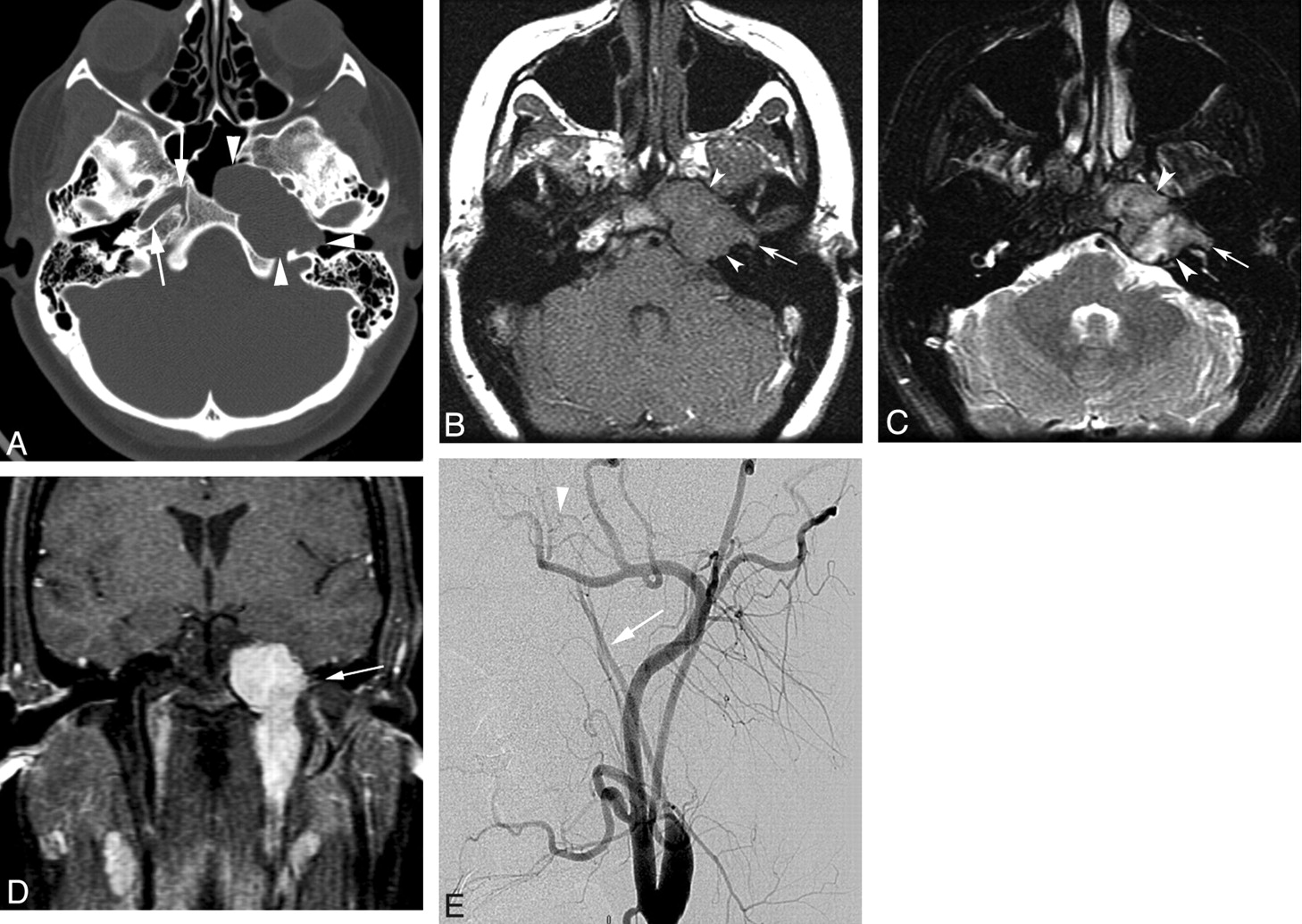
Work-up included a contrast-enhanced CT examination (Fig 1A), contrast-enhanced MR imaging (Fig 1B–D), and subsequently a conventional cerebral angiogram (Fig 1E). The examinations revealed a large, homogeneous avidly enhancing mass with heterogeneous high T2 signal intensity that smoothly expanded the left carotid canal. There was a small projection toward the cochlear promontory and the mass resulted in displacement of the ICA with occlusion near the cavernous segment. The effect on the Eustachian tube explained the patient's presenting complaint of unilateral ear effusion. The patient underwent surgical resection and histology confirmed the suspected diagnosis, carotid sympathetic plexus schwannoma.

Patient 1 is a 27-year-old woman presenting with left ear effusion, headache, and diplopia. A, Axial noncontrast CT image in bone window shows a mass that smoothly enlarges and remodels the left petrous portion of the carotid canal (arrowheads). The normal right petrous portion of the carotid canal is annotated (arrows). B and C, Axial precontrast T1 (B) and T2 MR (C) images, respectively, reveal an essentially isointense T1 and heterogeneously hyperintense T2 mass (arrowheads). D, Coronal postcontrast fat-saturated T1 MR image shows relatively homogeneous avid enhancement of the mass and extension from the neck through skull base to the cavernous sinus. Posterior lateral triangular projection toward the middle ear (arrow, B–D) may represent the caroticotympanic nerve of the internal carotid sympathetic plexus. E, Left common carotid artery injection from digital subtraction conventional angiogram in left anterior oblique projection reveals severe narrowing of the left ICA above the bifurcation (arrow) with occlusion near the cavernous portion (arrowhead).
Patient 2
A 68-year-old man presented with intermittent right-sided headache, diplopia, right-sided nasal obstruction, and tinnitus in the right ear. There was no personal or pertinent family history. On physical examination, the patient was found to have a right abducens palsy. He had a lateral gaze diplopia upon rightward gaze. Otherwise, the patient had intact extraocular muscle movement and facial sensation. No other relevant clinical findings were noted.
Work-up included an MR imaging (Fig 2A–C) and a CT (Fig 2D) of the head and skull base that demonstrated a homogeneous hyperintense T2, well-defined avidly enhancing mass smoothly expanding the right carotid canal. A similar smaller mass was seen in the left cavernous sinus. Six-month follow-up examination revealed no significant change in the appearance of the bilateral lesions. The patient noted spontaneous improvement in his diplopia, and no surgical procedure was performed. The diagnosis was presumptive, but the imaging findings were compelling for schwannoma.

Patient 2 is a 68-year-old man presenting with headache, diplopia, tinnitus, and nasal stuffiness. Precontrast T1 (A), T2 (B), and fat-suppressed postcontrast T1(C) axial images reveal hyperintense T2, isointense T1, avidly homogeneously enhancing mass in the right carotid canal surrounding the petrous and cavernous segments of the ICA (arrowhead). There is also a smaller mass along the anterior wall of the left ICA within the cavernous sinus (arrow) D, Axial contrast-enhanced CT in bone windows demonstrates right (arrowhead) greater than left (arrow) smooth expansion of the carotid canals by the masses.
Discussion
Schwannomas may present at any age but most commonly occur between the fourth and sixth decades.11 Our first patient was younger than the average age of reporting for head and neck schwannomas, but the patient had no additional findings to suggest neurofibromatosis type II, which more commonly presents in the second decade.9
Diplopia was experienced by all patients with this type of schwannoma. Ture et al4 reported a 23-year-old man who also presented with diplopia and was found to have the only other reported case of a carotid canal sympathetic plexus schwannoma. The abducens nerve (cranial nerve VI) is in proximity to the ICA, more medially located than the other cranial nerves12 in the center of the cavernous sinus. This anatomy may place the abducens nerve at particular risk for injury with cavernous sinus pathologies and result in the presenting complaint of diplopia experienced by these patients from unrestrained medial rectus muscle activity.
On surgical investigation of the index case by Ture et al,4 the schwannoma was inferomedial to the ICA and thus probably involving the cavernous sympathetic plexus. In patient 2, the mass was anterior medial to the right carotid artery and therefore also probably arose from the cavernous sympathetic plexus. However, in patient 1 the lateral projection to the cochlear promontory was likely the tympanic branch of the caroticotympanic nerve. These findings are suggestive of the first schwannoma in the literature to arise from the internal carotid sympathetic plexus. Because this is also the first case of internal carotid occlusion secondary to a carotid canal sympathetic plexus schwannoma, the position of the tumor lateral to the ICA cannot be confirmed. Although not histologically confirmed in patient 2, the second mass surrounding the left ICA is suggestive of the first reported case of bilateral carotid canal sympathetic plexus schwannoma.
The imaging characteristics of a carotid canal sympathetic plexus schwannoma are much like those of schwannomas in other portions of the body. They are well circumscribed, slow-growing masses that smoothly expand canals and foramina. It is these classic imaging features that make the authors confident in the diagnosis of patient 2. Hyperintense T2 signal intensity is noted in schwannomas, predominately from the Antoni type B myxoid material with areas of lower signal intensity collagen and cellular components (Antoni type A).9 Schwannomas are often homogeneous on T1 and noncontrast CT but may undergo cystic degeneration, calcification, hemorrhage, or fibrosis that gives a heterogeneous appearance.9 There is usually avid enhancement, which is more commonly homogeneous than heterogeneous. In the rare case of malignant degeneration, the mass may become less defined and exhibit rapid growth, with bony or brain invasion, rather than remodeling.
As discussed, the most common mass in the cavernous sinus is a meningioma, and it could have similar signal intensity characteristics to a schwannoma. It would be unusual for a meningioma to have an elongated course that smoothly expands the carotid canal. There was neither reactive hyperostosis nor dural tail. Other schwannomas also could be considered but would not be expected to course along the petrous carotid canal. The signal intensity and enhancement characteristics of a schwannoma are different from those expected for an epidermoid, aneurysm, or a blood vessel neoplasm. Lastly, the benign-appearing expansion of the canal and no history of primary malignancy make more aggressive neoplasms unlikely.
Conclusions
Although a very rare tumor by location, the carotid canal sympathetic plexus schwannoma is similar in imaging characteristics to schwannomas found elsewhere. In the total of 3 cases now reported in the literature, all patients presented with diplopia probably due to mass effect on the abducens nerve within the cavernous sinus.
Footnotes
-
Previously presented in part as an excerpta extrordinaire at: Annual Meeting of the American Society of Neuroradiology, May 15–20, 2010, Boston, Massachusetts.
-
Disclosures: J.D.H., research support (including provision of equipment and materials): Levin Family Chairman Fund, M.D. Anderson Cancer Center. Details: Salary support from charitable contribution for research in brain tumor imaging. F.D., speaker bureau: Medtronic, Details: Teaching faculty for yearly skullbase course.
References
- Received November 5, 2010.
- Accepted after revision November 13, 2010.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}