
Abstract
BACKGROUND AND PURPOSE: Many authors have reported the increase in vertebral body height after vertebroplasty. However, McKiernan et al demonstrated dynamic mobility in patients who underwent vertebroplasty and concluded that any article that claims vertebral height restoration must control for the dynamic mobility of fractured vertebrae. The purpose of this study was to compare prevertebroplasty (supine cross-table with a bolster beneath) with postvertebroplasty vertebral body height to find out whether vertebroplasty itself really increases the vertebral height.
MATERIALS AND METHODS: From July 2005 to July 2010, 102 consecutive patients with 132 VCFs underwent vertebroplasty at our institution. The indications for vertebroplasty were severe pain that was not responsive to medical treatment, and MR imaging−confirmed edematous lesions. Prevertebroplasty (supine cross-table with bolster beneath) lateral radiographs were compared with postvertebroplasty radiographs to evaluate the height change in vertebroplasty. Kyphotic angle and anterior vertebral body height were measured.
RESULTS: The patients ranged in age from 62 to 90 years. There were 16 men and 86 women. The difference in the kyphotic angle between supine cross-table with bolster and postvertebroplasty was −0.49 ± 3.59° (range, −9°–16°), which was not statistically significant (P = 0.124). The difference in the anterior vertebral body height between supine cross-table with bolster and postvertebroplasty was 0.84 ± 3.01 mm (range, −7.91–8.81 mm), which was statistically significant (P = .002).
CONCLUSIONS: The restoration of vertebral body height in vertebroplasty seems to be mostly due to the dynamic mobility of fractured vertebrae; vertebroplasty itself does not contribute much to the restoration of vertebral height.
Abbreviations:
- VAS
- visual analog scale
- VCF
- vertebral compression fracture
Hiwatashi et al1 found increases in vertebral body height after vertebroplasty and published their results in 2003. Since then, there have been several articles related to height increase after vertebroplasty or kyphoplasty.2–5 These articles all concluded that vertebroplasty or kyphoplasty can increase the height of fractured vertebrae. They proposed that the mechanism of increase in vertebral body height is probably related to padding beneath the upper chest and pelvic region, injection of the high viscosity bone cement under pressure, or balloon tamps. However, McKiernan et al6 demonstrated dynamic mobility in 44% of 41 patients (35% of treated vertebrae) who underwent vertebroplasty. They concluded that any article that claims vertebral height restoration must control for the dynamic mobility of fractured vertebrae. A recent study, which used sitting and supine cross-table (with a bolster beneath) lateral radiographs, demonstrated that dynamic mobility occurred in 87.5% of the treated vertebrae.7 The authors found that 87.5% of 144 MR imaging−proved edematous VCFs were demonstrated to be mobile. The average vertebral body height increase from sitting position to supine with bolster was 8.48 ± 5.36 mm. Because a high percentages of fractured vertebrae are mobile, we must answer the following question: What is the real reason for vertebral body height increase in vertebroplasty?
The objective of this study was to compare prevertebroplasty (supine cross-table with a bolster beneath) with postvertebroplasty vertebral body height to evaluate factors that may correlate with these changes in height (including the occurrence and degree of mobility of the fractured vertebral endplates).
Materials and Methods
From July 2005 to July 2010, one hundred two consecutive patients with 132 osteoporotic VCFs underwent vertebroplasty at our institution. The institutional review board approved this radiographic analysis. The indications for vertebroplasty were severe pain that was not responsive to medical treatment and MR imaging−confirmed edematous lesions (hyperintense signal intensity on a short-tau inversion recovery sequence and/or contrast enhancement on fat-suppressed gadolinium-enhanced T1-weighted imaging). Pre- and postvertebroplasty anteroposterior and lateral radiographs were obtained. In addition, a preprocedural sitting lateral radiograph centered on the fractured vertebra and a supine cross-table lateral radiograph centered on the index vertebra with a bolster (10 cm in height) placed beneath were obtained for each patient.
The kyphotic angles of the VCFs were measured from the superior and inferior endplates of the fractured vertebra. Measurement of the anterior vertebral body height of the fractured vertebra was based on the techniques used by McKiernan et al.8 To eliminate the inter-radiographic magnification error, we matched each index VCF to the referent vertebra on the sitting lateral radiograph. Each index-referent vertebral pair remained constant throughout the analysis. For supine cross-table with bolster and postvertebroplasty lateral radiographs, dimensions of the index vertebra were expressed as a percentage of the analogous dimension of the referent vertebra and then were scaled to the absolute dimensions of the original sitting lateral radiograph. This process cancelled out any residual inter-radiographic magnification error and allowed direct radiographic comparisons. For outcome measurement, a VAS with 10 divisions was used.
Digital files of the patients' radiographs were retrieved for analysis from the PACS. Two of the authors (D.-F.L. and Y.-J.C.) performed the measurements. Intraobserver and interobserver reproducibility of these measurements was evaluated by using intraclass correlation coefficients.
Statistical Analysis
The results are expressed as the mean ± SD. The statistical significance of changes in vertebral body height and the kyphotic angle was evaluated with the paired t test. A P value < .05 was considered statistically significant. All statistical analyses were carried out by using the Statistical Package for the Social Science, Version 12.0 (SPSS, Chicago, Illinois), Windows version.
Results
One hundred two patients underwent vertebroplasty to treat 132 MR imaging−proved edematous VCFs. The patients ranged in age from 62 to 90 years (mean, 76.97 years). There were 16 men and 86 women. Seventy-four patients (72.5%) had 1-level fractures, 26 patients had 2-level fractures, and 2 patients had 3-level fractures. L1 was the most common level affected (n = 32), followed in order by T12 (n = 31) and L2 (n = 17).
Pain assessed by the VAS was significantly decreased (P < .001) from a mean of 8.91 ± 0.74 (range, 7–10) before the procedure to 1.90 ± 1.48 (range, 0–9) after 1-month follow-up. Ninety-one patients (89%) were satisfied with the results. Only 1 patient described having no improvement in pain after vertebroplasty.
Intraobserver (Y.-J.C.) reproducibility was 0.93 for the height of the vertebral body and 0.96 for the kyphotic angle. Interobserver reproducibility was 0.94 for height and 0.93 for the kyphotic angle. The mean kyphotic angle on sitting lateral radiographs was 17.96 ± 8.45° (range, 0°–40°). It changed to 7.22 ± 7.24° (range, −15°–26°) on supine cross-table with bolster radiographs and 7.71 ± 6.83° (range, −9°–29°) on postvertebroplasty radiographs. The average anterior vertebral height on sitting lateral radiographs was 13.83 ± 7.01 mm (range, 1.12–29.87 mm). It changed to 22.01 ± 6.28 mm (range, 6.09–38.53 mm) on supine cross-table with bolster lateral radiographs and 21.24 ± 5.59 mm (range, 6.11–37.51 mm) on postvertebroplasty radiographs (Table). The prevertebroplasty (supine with bolster) anterior vertebral body height was higher than the postvertebroplasty anterior vertebral body height in 87 vertebrae (65.9%). The difference in the kyphotic angle between supine cross-table with bolster radiographs and postvertebroplasty radiographs was −0.49 ± 3.59° (range, −9°–16°), which was not statistically significant (P = .124). The difference in anterior vertebral body height between supine cross-table with bolster radiographs and postvertebroplasty radiographs was 0.84 ± 3.01 mm (range, −7.91–8.81 mm), which was statistically significant (P = .002).
The average kyphotic angle and vertebral body height in preprocedural and postprocedural lateral radiographsa
Eighty-one percent (107/132) of vertebrae had a height increase >3 mm (10.3 ± 5.1 mm) from sitting to supine cross-table with bolster radiographs; 19% (25/132) of vertebrae had a height increase ≦3 mm. Seventy-nine percent (104/132) of vertebrae had improvement in the degree of kyphosis of >5° (−12.9 ± 5.7°) from sitting to supine cross-table with bolster radiographs. Of those 25 vertebrae with fixed height (height increase, ≦3 mm) from sitting to supine cross-table with bolster radiographs, only 4 (16%) had a height increase of >3 mm (mean, 4.7 mm; range, 3.1–6.9 mm) after vertebroplasty.
Discussion
A large part of the success of vertebroplasty depends on correct patient selection, and MR imaging plays a vital role in this process.9 Many authors9–11 recommended using MR imaging as a preprocedural examination. Brown et al12 stated that 100% of patients with bone marrow edema had clinical benefit. We followed this rule, and vertebroplasty was performed in vertebrae with bone marrow edema on MR imaging. If the patient had contraindications for MR imaging, we used dynamic radiographs (sitting and supine with bolster) to find out which vertebra was symptomatic (dynamic mobility) after we ruled out the possibility of infection. If a patient had severe back pain without an edematous lesion on MR imaging, we would also use dynamic radiographs to check the mobility. Usually, if the pain was severe, there was always some dynamic mobility at the fractured vertebrae.
Hiwatashi et al1 measured the height of 85 vertebral bodies in 37 patients before and after vertebroplasty. The average increase in vertebral body height was 2.5 mm; 13 of 85 treated vertebrae remained unchanged. They concluded that vertebral body height often increases during vertebroplasty. Teng et al2 reviewed digital radiographs of 73 vertebral bodies in 53 patients before and after vertebroplasty and found that the restoration percentage for the height of the vertebral body was 29% for the anterior border. They, therefore, also concluded that vertebroplasty increases the height of a fractured vertebra. Many other authors have also reported increased vertebral body height from vertebroplasty (with or without any reduction maneuver) or kyphoplasty.3–5,13–15
However, McKiernan et al6 demonstrated dynamic fracture mobility in 44% of their patients (35% of treated vertebrae) who underwent vertebroplasty. They concluded that in any article in which vertebral height restoration is claimed, there must be control for the occurrence of dynamic mobility of the fractured vertebrae. In a study by Chen et al,7 87.5% of 144 MR imaging−proved edematous VCFs were demonstrated to be mobile. The average vertebral body height increase from sitting to supine with bolster lateral radiographs was 8.48 ± 5.36 mm (range, −1.17–24.04 mm), which was statistically significant (P < .001). On the basis of these findings, we propose that dynamic mobility of a fractured vertebra may contribute to height restoration in vertebroplasty.
As McKiernan et al6 mentioned, because any article that claims vertebral height restoration must control for the occurrence of dynamic mobility of the fractured vertebrae, we compared the vertebral body height between supine with bolster lateral radiographs and postvertebroplasty radiographs to decide whether the height increase came from the dynamic mobility of fractured vertebra or from the vertebroplasty itself. In this study, the difference in the kyphotic angle between supine cross-table with bolster radiographs and postvertebroplasty radiographs was −0.49 ± 3.59° (range, −9°–16°), which was not statistically significant (P = 0.124). That means that there was no significant difference between the kyphotic angle on supine with bolster and postvertebroplasty radiographs; the correction of the kyphotic angle was due to the dynamic mobility of the fractured vertebrae, not due to vertebroplasty itself. Vertebroplasty itself did not contribute to the correction of the kyphotic angle.
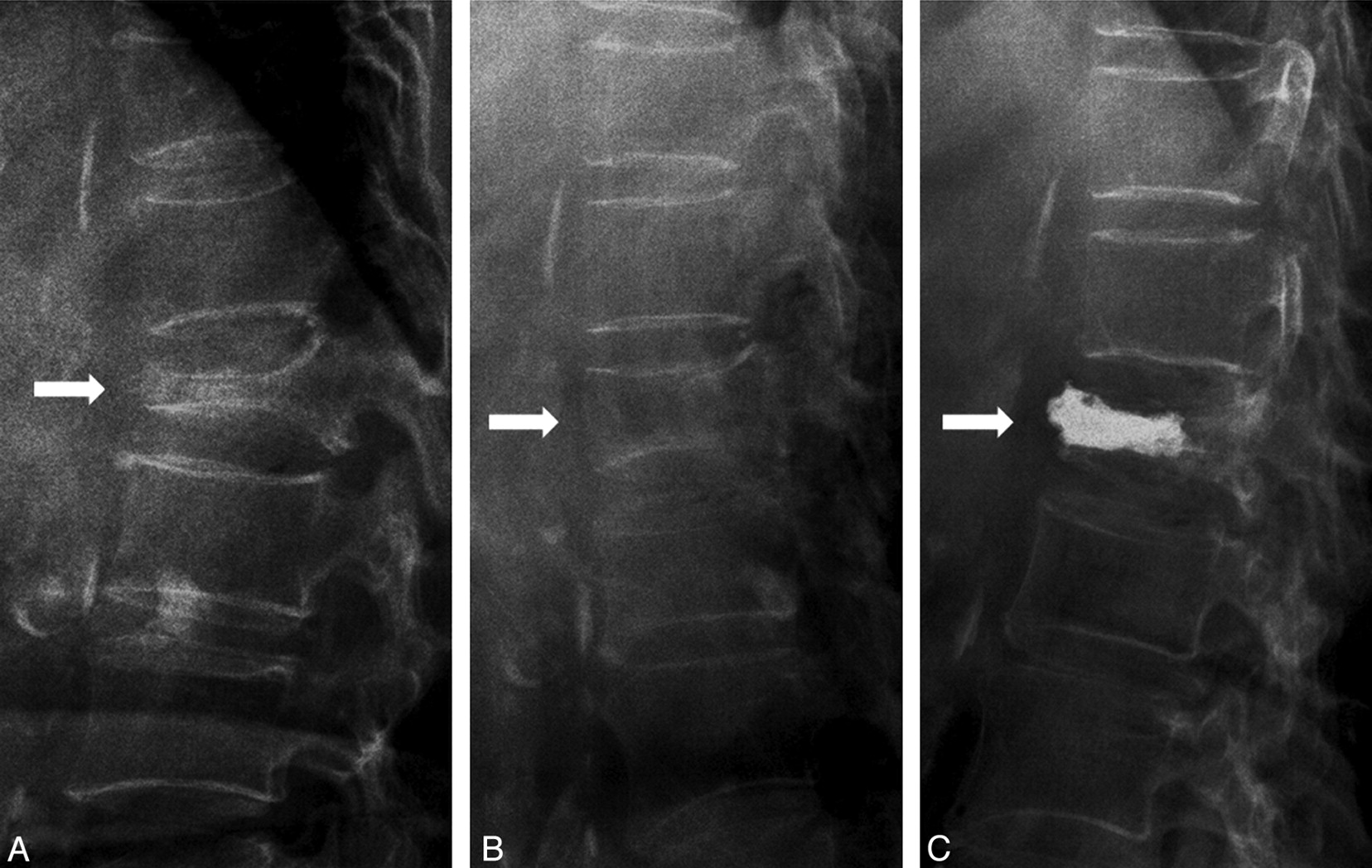
The difference in anterior vertebral body height between supine cross-table with bolster and postvertebroplasty radiographs was 0.84 ± 3.01 mm, which was significant (P = .002). That means that the anterior vertebral body height restoration on supine with bolster radiographs was more than that on postvertebroplasty radiographs and was statistically significant. However, the difference was so small that it may not have any clinical significance. Why is the vertebral height on supine with bolster radiographs higher than the height on postvertebroplasty radiographs? It is because of the bolster that causes the fractured vertebrae to be in a hyperextended position (Fig 1B); the degree of hyperextension is less during vertebroplasty (Fig 1C). However, the difference is not much, only 0.84 ± 3.01 mm.

A 62-year-old woman had severe back pain due to a T12 compression fracture. The anterior vertebral body height in the sitting (A) lateral radiograph is 7.23 mm and changed to 21.22 mm in the supine with bolster (B) lateral radiograph and 15.41 mm in the postvertebroplasty radiograph (C).
Theoretically, if the vertebra is fixed, there should be no height increase after vertebroplasty. Why did some fixed vertebrae (height increase, ≦3 mm) have a height increase after vertebroplasty in our study? The reasons may be due to poor positioning of the bolster so that the fractures did not open well, pain-induced muscle spasm during the examination, and some measurement error due to the poor quality of radiographs. This situation only happened in fractures with mild mobility.
The weaknesses of this study are the following: 1) As a retrospective study from a single center, there was potential for several biases (referral bias, patient characteristics, and so forth). 2) The number of patients enrolled was small. 3) Patients were screened by using MR imaging and not other modalities and had to show signs of edema—this group may not be representative of all patients or all fractures undergoing vertebroplasty. 4) Although we tried our best to measure the radiographs correctly, there may be still some measurement error.
Conclusions
The restoration of vertebral body height in vertebroplasty seems to be mostly due to the dynamic mobility of fractured vertebrae; vertebroplasty itself does not contribute much to the restoration of vertebral height.
If height restoration is mainly due to dynamic mobility and can be restored by posture reduction, we should try to get a better height restoration by using towel rolls under the shoulders and hips to hyperextend the back and open the fracture cleft.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received February 21, 2011.
- Accepted after revision May 9, 2011.
- © 2012 by American Journal of Neuroradiology





{kind=link}