
Abstract
BACKGROUND AND PURPOSE: Our aim was to compare 3D TOF-MRA sequences at 3T and 1.5T in the follow-up of coiled aneurysms. The follow-up of coiled intracranial aneurysms is mandatory to depict potential recanalization. 3D-TOF MRA is an appropriate tool for this purpose.
MATERIALS AND METHODS: DSA and 3D TOF-MRA at 1.5T and 3T were performed in a prospective series of 126 aneurysms in 96 patients (58 women, 38 men; age, 25–75 years; mean, 51.3 ± 11.3 years). DSA was the reference standard to which the accuracy of 3D TOF-MRA was compared. The quality of aneurysm occlusion was assessed independently and anonymously by a core lab by using a 3-grade scale (total occlusion, neck remnant, and aneurysm remnant). Adequate occlusion was defined as total occlusion or neck remnant and used in a 2-grade scale: adequate occlusion/aneurysm remnant.
RESULTS: With DSA, total occlusion was depicted in 58 aneurysms (46.0%); neck remnant, in 33 aneurysms (26.2%); and aneurysm remnant, in 35 aneurysms (27.8%). Adequate occlusion was seen in 91 cases (72.2%). A remnant (aneurysm or neck) was depicted in 68 cases (54.0%). For the 3 imaging techniques and regardless of scale used, the interobserver agreement was always greater at 3T than at 1.5T. SE and NPV for the prediction of aneurysm remnant versus adequate occlusion were higher at 3T than at 1.5T (SE 3T, 0.74; SE 1.5T, 0.54; NPV 3T, 0.90; NPV 1.5T, 0.85).
CONCLUSIONS: In this large prospective series of patients, 3D TOF-MRA was superior at 3T to 1.5T for the evaluation of coiled intracranial aneurysms.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- AcomA
- anterior communicating artery
- CE
- contrast-enhanced
- CI
- confidence interval
- MIP
- maximum intensity projection
- NPV
- negative predictive value
- PPV
- positive predictive value
- SE
- sensitivity
- TOF
- time-of-flight
- VA
- vertebral artery
- VB
- vertebrobasilar system
Endovascular treatment with coils is now considered the first-line treatment in the management of most intracranial aneurysms, ruptured or unruptured.1,2 A disadvantage of aneurysm coiling is the potential risk of aneurysm recanalization reported in approximately 20% of cases, with repeat treatment in approximately 10% of cases.3 Therefore, as a complement to the usual clinical follow-up, a regular anatomic follow-up is needed to evaluate aneurysm occlusion in mid- and long-term. Intra-arterial DSA has been, for a long time, the standard follow-up technique, but this technique is invasive, is associated in a small number of patients with clinical complications, and exposes patients to ionizing radiation.4
The use of MRA at 1.5T has been widely evaluated, showing a moderate-to-high diagnostic performance for both TOF- MRA and CE-MRA.5⇓–7 Both 3D TOF-MRA and CE-MRA have also been evaluated at 3T, also showing good diagnostic performance.7⇓⇓–10 Direct comparison of MRA performed at 3T and 1.5T is relatively scarce, has been conducted in small series of patients, and is associated with contradictory results.11⇓–13
To compare the value of 3D-TOF at 1.5T and 3T, a prospective consecutive monocentric study was conducted in patients having follow-up examinations including DSA for coiled intracranial aneurysms. In this group of patients, 3D TOF-MRA was performed at both 3T and 1.5T. With a strong methodology and DSA as the criterion standard, the diagnostic accuracy at 3T and 1.5T was compared.
Materials and Methods
Study Population
Approval of the institutional review board of Reims hospital was obtained for this study, and written informed consent was obtained for all patients.
All patients harboring ruptured or unruptured intracranial aneurysms treated with coils in our center are followed by using MRA and DSA. Usually MRA is performed 3 months after the endovascular treatment. At 1 year, the quality of aneurysm occlusion is evaluated by both MRA and DSA. Further follow-up is tailored according to the specific situation of each patient, mostly based on MRA. DSA is performed if a retreatment has to be discussed or if a neck or aneurysm remnant is changing with the time.
From April 2006 to September 2008, all patients eligible for follow-up DSA were prospectively included unless they had a contraindication for MR imaging, were claustrophobic, or refused. Patients younger than 18 years were not included. Because the goal was to compare 3D TOF at 1.5T and 3T in patients having coiled aneurysms, aneurysms treated by parent vessel occlusion or with stent placement were excluded from the series. In patients with multiple aneurysms, aneurysms treated with clips or stent placement were also excluded from the series. Within the inclusion period, some patients were evaluated twice after undergoing repeat coiling or coiling of another aneurysm or if repeat DSA was judged useful to evaluate an evolution of a remnant.
DSA, 1.5T MRA, and 3T MRA were performed during a short hospitalization of <24 hours with a similar order of examinations for all patients (1.5T MRA, DSA, and 3T MRA). No endovascular treatment was performed during DSA.
Imaging Technique for Intra-Arterial DSA
Intra-arterial DSA was performed with a biplane angiographic system (Axiom Artis; Siemens, Erlangen, Germany). Using transfemoral catheterization, we performed selective injections of the ICA or VA, according to aneurysm location. We obtained the following standard projections: anteroposterior view, lateral view, and working view (optimal projection used at coil embolization). For ICA, 8 mL of nonionic contrast agent (iodixanol, Visipaque; GE Healthcare, Oslo, Norway) was injected with a velocity of 4 mL/s. For the VA, 8–10 mL was injected with a velocity of 4–5 mL/s.
Imaging Technique for MRA
MRA examinations were performed on 1.5T (Signa; GE Healthcare, Milwaukee, Wisconsin) and 3T (Achieva; Philips Healthcare, Best, the Netherlands) scanners. For both 1.5T and 3T MRA, examinations were performed with the optimized parameters for each platform and parallel imaging was used with an acceleration factor of 2. At 1.5T, the parameters were the following: TE, 6.9 ms; TR, 38 ms; flip angle, 20°; total acquisition time, 6:09 minutes; number of sections, 110; section thickness, 0.7 mm; FOV, 220 mm; rectangular field of view, 70%; acquisition matrix, 320; reconstruction matrix, 512; reconstructed voxel size, 0.43 × 0.43 × 0.7 mm. At 3T, parameters were the following: TE, 3.45 ms; TR, 18 ms; flip angle, 20°; total acquisition time, 4:59 minutes; number of sections, 140; section thickness, 0.55 mm; FOV, 210 mm; rectangular field of view, 90%; acquisition matrix, 464; reconstruction matrix, 512; reconstructed voxel size, 0.41 × 0.41 × 0.55 mm.
Data Collection
Clinical and anatomic data regarding patient (sex, age), aneurysm (number, location, size of aneurysm), and technique of treatment (standard coiling technique, remodeling technique, stent placement, or parent artery occlusion) were collected. The time interval between aneurysm treatment and anatomic evaluation was also collected (in months).
Aneurysm location was classified into 4 groups: ACA/AcomA, ICA, MCA, and VB. Aneurysm size was classified into 3 groups: ≤5 mm, >5 and <10 mm, and ≥10 mm.
Data Analysis
All examinations (DSA, 1.5T MRA, and 3T MRA) were made anonymous with a different-number random assignment by series. All images were independently evaluated in random order by 2 experienced interventional neuroradiologists (A.B. and J.Y.G.), and in case of disagreement, a third analysis was conducted by another interventional neuroradiologist (L.P.) with knowledge of the 2 previous evaluations. The judgment of the third radiologist acted as a tie-breaker.
We evaluated 1.5T MRA, 3T MRA, and DSA separately without knowledge of the other MRA or DSA examinations. The pretreatment DSA was not available, but the location of the aneurysms to be evaluated was provided to the readers. For both 1.5T and 3T MRA, source images and MIP reconstructions were analyzed.
Aneurysm occlusion was evaluated by using the 3-grade scale: total occlusion, neck remnant, aneurysm remnant.14 Two 2-grade scales derived from the 3-grade scale were used for statistical analysis: adequate occlusion (total occlusion or neck remnant)/aneurysm remnant; and total occlusion/remnant (neck or aneurysm). Artifacts produced by the coils were evaluated by using a 2-grade scale: 0 = no artifacts or moderate artifacts with feasible evaluation of aneurysm occlusion, 1 = important artifacts making the evaluation of aneurysm occlusion difficult. The visibility of the coils was also evaluated by using a 2-grade scale: 0 = not visible, 1 = visible.
Statistical Analysis
Quantitative variables are reported as mean ± SD; qualitative variables, as number and percentage. Artifacts and visibility of coils observed between 1.5T and 3T MRA were compared by using Wilcoxon signed rank tests. P values <.05 were considered statistically significant.
Because the degree of aneurysm occlusion was defined by using the Raymond14 simplified 3-point classification scale (complete occlusion, neck remnant, and aneurysm remnant), weighted κ statistics were used to obtain interobserver and intermodality agreement for each technique. According to Landis and Koch,15 the interpretation of κ was as follows: κ < 0 indicated no agreement; κ = 0–0.19, poor agreement; κ = 0.20–0.39, fair agreement; κ = 0.40–0.59, moderate agreement; κ = 0.60–0.79, substantial agreement; and κ = 0.80–1.00, almost perfect agreement. Using the consensus evaluation of intra-arterial DSA as a reference test to evaluate the degree of aneurysm occlusion, we calculated the sensitivity, specificity, NPV, and PPV for MR angiography with corresponding 95% CIs and also 2-point classification scales: adequate occlusion (complete occlusion or neck remnant) and aneurysm remnant or complete occlusion versus remnant. All analyses were performed by using the Statistical Package for the Social Sciences software (Version 17.0; SPSS, Chicago, Illinois).
Results
Study Population
During the follow-up period, 100 patients with coiled aneurysms were evaluated by DSA, 1.5T MRA, and 3T MRA. We excluded 4 patients: One was treated by parent vessel occlusion, and 2 were treated with coiling and stent placement. For 1 patient, 1.5T MRA was performed but images were not retrievable.
The final population was 96 patients (age, 25–75 years; mean, 51.3 ± 11.3 years; median, 52 years), including 58 women (60.4%) and 38 men (39.6%). Seventy-three patients had 1 aneurysm, 17 patients had 2 aneurysms, and 6 patients had 3 aneurysms. Eight patients were evaluated twice (5 having 1 aneurysm and 3 having 2 aneurysms). The number of aneurysms to be evaluated was 136. In 10 patients with multiple aneurysms, 1 aneurysm was treated with clips (9 patients) or a stent (1 patient). These 10 aneurysms were excluded from the final population.
Finally 126 aneurysms were evaluated in 96 patients. Eighty-two aneurysms were ruptured (65.1%), and 44, unruptured (34.9%). Aneurysm location was the ACA/AcomA in 47 aneurysms (37.3%), ICA in 40 aneurysms (31.7%), MCA in 19 aneurysms (15.1%), and VB in 20 cases (15.9%). Pretreatment aneurysm size was between 2 and 24 mm (mean, 6.8 ± 3.5 mm). Fifty-one aneurysms were ≤5 mm (40.5%); 55, between 5 and 10 mm (43.7%); and 20, ≥10 mm (15.9%).
The interval time between aneurysm treatment and follow-up examinations was 3–215 months (mean, 22.7 ± 32.6 months; median, 12 months). Interval time was <11 months in 9 aneurysms (7.1%), between 11 and 13 months in 63 aneurysms (50.0%), and >13 months in 54 aneurysms (42.9%).
Interobserver Agreement
When we evaluated aneurysm occlusion by using the 3-grade scale, weighted κ was 0.50 for DSA, 0.59 for 3T MRA, and 0.55 for 1.5T MRA. With the 2-grade scale (adequate occlusion/aneurysm remnant), κ was 0.61 for DSA, 0.77 for 3T MRA, and 0.63 for 1.5T MRA. Finally with the 2-grade scale (total occlusion/remnant), κ was 0.62 for DSA, 0.59 for 3T MRA, and 0.58 for 1.5T MRA.
Aneurysm Occlusion
Using DSA, total occlusion was depicted in 58 aneurysms (46.0%); neck remnant, in 33 aneurysms (26.2%); and aneurysm remnant, in 35 aneurysms (27.8%). Adequate occlusion was seen in 91 cases (72.2%). A remnant (aneurysm or neck) was depicted in 68 cases (54.0%) (Fig 1). Using 3T MRA, total occlusion was depicted in 65 aneurysms (51.6%); neck remnant, in 29 aneurysms (23.0%); and aneurysm remnant, in 32 aneurysms (25.4%). Adequate occlusion was seen in 94 cases (74.6%). A remnant (aneurysm or neck) was depicted in 61 cases (48.4%). With 1.5T MRA, total occlusion was depicted in 75 aneurysms (60.0%); neck remnant, in 29 aneurysms (23.2%); and aneurysm remnant, in 21 aneurysms (16.8%). Adequate occlusion was seen in 104 cases (83.2%). A remnant (aneurysm or neck) was depicted in 50 cases (40.0%).

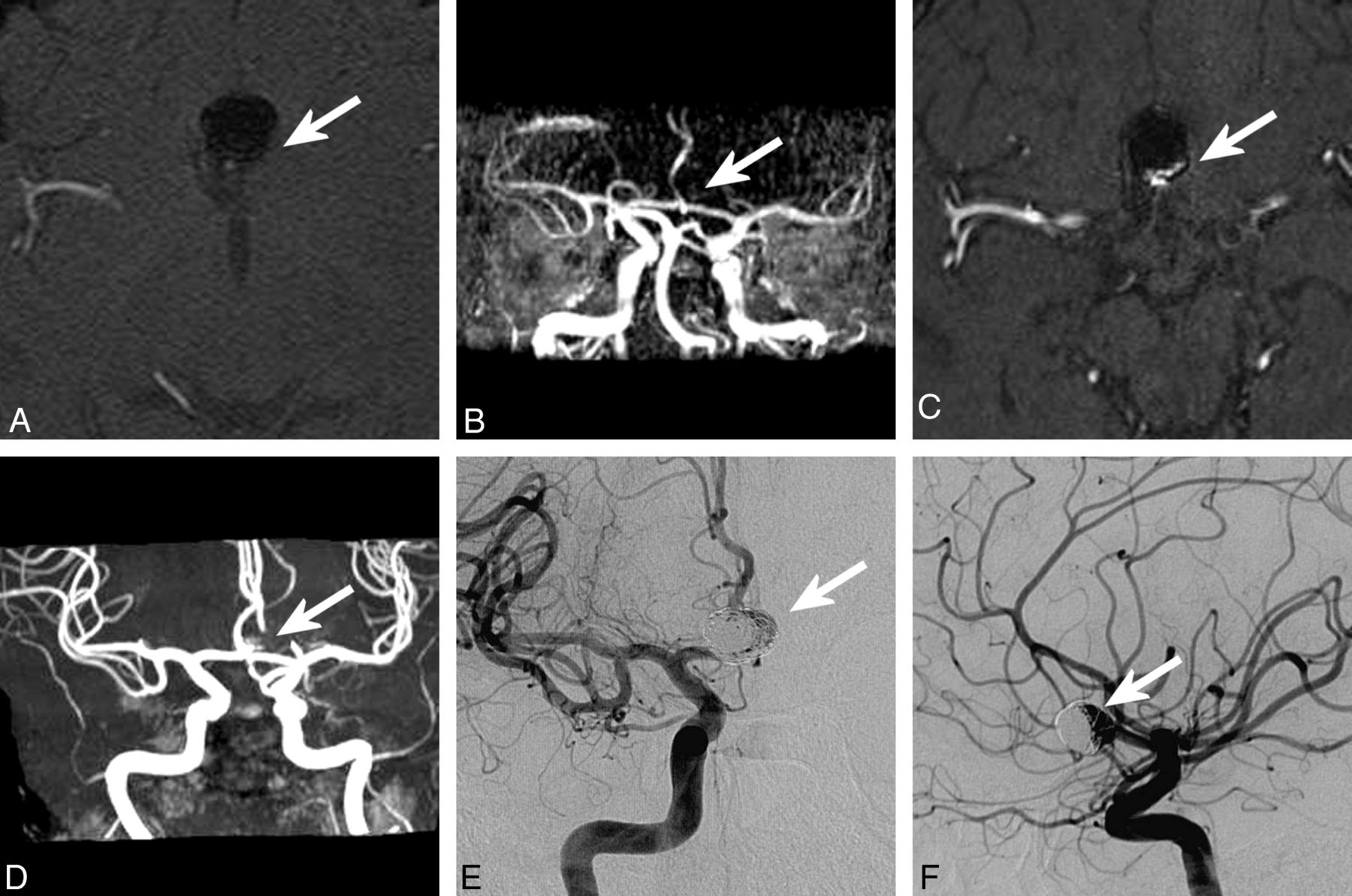
Anterior communicating artery aneurysm treated with coils. MRA at 1.5T (source images, A; MIP reconstruction, B) shows total occlusion of the aneurysm (white arrow). MRA at 3T (source images, C; MIP reconstruction, D) shows an aneurysm remnant (white arrow). DSA (anteroposterior view, E; lateral view, F shows the aneurysm remnant (white arrow).
Anatomic results (adequate occlusion/aneurysm remnant) evaluated by 1.5T and 3T MRA are compared with DSA results in Table 1.
Anatomic results (adequate occlusion/aneurysm remnant) with 1.5T and 3T MRA versus DSA
Intermodality Agreement
When we evaluated aneurysm occlusion by using the 3-grade scale, the agreement of 3T MRA with DSA was 0.51 compared with 0.47 for the agreement of 1.5T MRA with DSA. With the 2-grade scale (adequate occlusion/aneurysm remnant), the agreement of 3T MRA with DSA was 0.70 compared with 0.59 for the agreement of 1.5T MRA with DSA. With the 2-grade scale (total occlusion/remnant), the agreement of 3T MRA with DSA was 0.54 compared with 0.52 for the agreement of 1.5T MRA with DSA.
Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value
The dichotomization of adequate occlusion/aneurysm occlusion is shown in Table 2, and the dichotomization of total occlusion/neck or aneurysm remnants is shown in Table 3.
Sensitivity, specificity, positive predictive value, and negative predictive value for 3T MRA and 1.5T MRA (DSA as the criterion standard): adequate occlusion/aneurysm remnant
Sensitivity, specificity, positive predictive value, and negative predictive value for 3T MRA and 1.5T MRA (DSA as the criterion standard): total occlusion/neck or aneurysm remnants
Artifacts: Visibility of the Coils
At 3T, no or moderate artifacts were observed in 121 aneurysms (96.0%) and important artifacts were observed in 5 cases (4.0%). At 1.5T, no or moderate artifacts were observed in 116 aneurysms (92.1%) and important artifacts were observed in 10 cases (7.9%). The difference between 1.5T and 3T was not statistically significant (P = .096).
At 3T, coils were visible in 120 cases (95.2%) and not visible in 6 cases (4.8%). In 5/6 cases, aneurysms were <5 mm. In the 6 cases, aneurysms were located close to areas with artifacts. At 1.5T, coils were visible in 125 cases (99.2%) and not visible in 1 case (0.8%). The difference was statistically significant (P = .025).
Discussion
In the literature, the comparison between 3T MRA and 1.5T MRA for the follow-up of coiled aneurysms yielded heterogeneous results. In a small 20-aneurysms series, no advantage of 3T MRA versus 1.5T MRA was seen.11 A large prospective trial showed similar sensitivity and NPV with both 1.5T and 3T, but direct comparison was not available because a group of patients was evaluated at 1.5T and another at 3T.10 Another small series showed that 3T MRA had better agreement with DSA than 1.5T MRA and that coil artifacts were smaller at 3T than at 1.5T.12
In our large series of 126 coiled intracranial aneurysms, 3D TOF-MRA at 3T was superior to 3D TOF-MRA at 1.5T to evaluate the quality of aneurysm occlusion. Regardless of the scale used to analyze aneurysm occlusion, the interobserver agreement was always greater with 3T compared with 1.5T. Also the sensitivity of 3T was greater than 1.5T to distinguish adequate occlusion and aneurysm remnant or total occlusion and neck or aneurysm remnants.
As previously reported, the methodologic quality of the studies dealing with MRA for evaluation of coiled aneurysm occlusion is often moderate.7 Our study was designed by using the criteria of Kwee and Kwee7 to obtain a high methodologic quality. It was conducted from April 2006 to September 2008. During this period, the use of stents in our department was very limited and flow diverters were not available. Because the performance of MRA is probably not the same in aneurysms treated only with coils and with coiling and stent placement, the decision was made to exclude the 3 aneurysms treated with stents to compare the efficacy of MRA at 3T and 1.5T in a homogeneous population of coiled aneurysms.16
The most popular scale to evaluate aneurysm occlusion after coiling is the 3-grade scale: total occlusion, neck remnant, and aneurysms.14 This scale was used in the present study, but it is not easy to manipulate and its clinical significance is unknown.17 Using this scale, previous publications have shown that the independent evaluation of postoperative aneurysm occlusion by a core lab is different and less optimistic than the evaluation of the physician doing the treatment.18 In the present series, the interobserver agreement was relatively low, regardless of the technique used, and it is probably partially explained by the fact that it is not so easy and partly subjective to differentiate neck and aneurysm remnants and it is sometimes difficult to differentiate total occlusion and neck remnants. Also, with DSA as the criterion standard, intermodality agreement was relatively low but slightly higher with 3T (κ = 0.51 versus 0.47 for 1.5T).
The clinical significance of a neck remnant is also unknown. The Cerebral Aneurysm Rerupture After Treatment study showed that the risk of early rebleeding after coiling of ruptured aneurysms was directly related to the quality of aneurysm occlusion.19 The risk of rerupture was 1.1% for aneurysms completely occluded, 2.9% for 91%–99%, 5.9% for 70%–90%, and 17.6% for <70%. Little information is available regarding the quality of aneurysm occlusion in case of late rebleeding or rupture of an unruptured coiled aneurysm. In the large International Subarachnoid Aneurysm Trial cohort in the long-term follow-up (range, 6–14 years; mean, 9 years), only 10 late (>1 year) rebleedings were observed, but the quality of aneurysm occlusion was not reported.20 In a series of 393 patients treated by coiling for ruptured aneurysms between 1995 and 2003, late rebleeding was observed in 5 patients with a delay of, respectively, 4, 8, 12, 30, and 40 months.21 In all patients evaluated by DSA at the time of rebleeding, aneurysm remnants were depicted. Finally, the risk of rupture or rerupture is probably higher in aneurysm remnants than in neck remnants, and depicting the aneurysm remnant seems critical in the follow-up of coiled aneurysms.
Accordingly, the use of a 2-grade scale derived from the 3-grade scale and combining total occlusion and neck remnant into 1 grade called appropriate is probably effective from a clinical point of view. With this scale, the interobserver agreement was higher at 3T than at 1.5T (respectively, κ = 0.77 and κ = 0.63). Also intermodality agreement (by using DSA as the criterion standard) was higher with 3T compared with 1.5T (respectively, κ = 0.70 and κ = 0.59).
Because the most crucial aspect of MRA is to correctly depict the aneurysm remnant, the NPV is quite important. MRA at 3T has a higher negative predictive value than at 1.5T (respectively, 0.90 and 0.85): Sixteen aneurysms with remnants were depicted as having adequate occlusion by 1.5T MRA, but only 9, by 3T MRA. Also the sensitivity of 3T MRA is much higher than that of 1.5T MRA (respectively, 0.74 and 0.54) with a higher number of aneurysm remnants detected by 3T MRA compared with 1.5T (respectively, 26 and 19 of 35 detected by DSA). When we compared 3T MRA and 1.5T MRA for the detection of any remnant (neck or aneurysm), similar results were obtained but are probably clinically less relevant. Important artifacts were more frequent at 1.5T (7.9%) than at 3T (4.0%), but the visibility of the coils was better at 1.5T.
Our study has some limitations. First, only 3D TOF sequences were compared at 3T and 1.5T. Comparison of CE-MRA at 3T and 1.5T was technically difficult because it was not really feasible to have 2 injected MRA examinations in a very short period of time. The next step of this evaluation will be to compare 3D TOF- and CE-MRA at 3T. Second, because the appearance of 1.5T and 3T images was slightly different, the readers were not totally blind to the sequences they were reading (1.5T or 3T); this feature created some bias. Third, other factors than magnetic field strength (vendors, platforms, MRA parameters, and so forth) can play a role in the difference of efficacy between both sequences. However, because the goal was to compare the use of 3D TOF sequences at 1.5T and 3T in the current practice, optimized parameters were used for both sequences. Certainly platforms from different vendors (and also from the same vendor) will not have the same performances, but these are quite difficult to evaluate. Fourth, another potential limitation was that some aneurysms were evaluated twice, which can result in a decrease of the effective number of aneurysms and in the statistical power. However, in most cases, a long period of time elapsed between the 2 evaluations and the second evaluation was related to the treatment of another aneurysm (in the case of multiple aneurysms) or to a change of the quality of aneurysm occlusion. Fifth, aneurysms treated with stents or flow diverters were not included in the present series. However, preliminary series have shown that evaluation of aneurysm occlusion with MRA in aneurysms treated with coils and stents was difficult due to stent artifacts.16 Therefore, it was logical to compare 3T and 1.5T MRA in a homogeneous population treated only with coiling.
Conclusions
In this large prospective series of patients, 3D TOF at 3T was superior to 3D TOF at 1.5T for the evaluation of coiled intracranial aneurysms. The next steps are to compare 3D TOF- and CE-MRA at 3T to determine the most appropriate sequence for the follow-up of coiled aneurysms and to determine the appropriate imaging technique for the follow-up of aneurysms treated with stents and flow diverters.
Footnotes
-
The authors declare that they have no conflict of interest with the topic of the manuscript.
-
Disclosures: Laurent Pierot—RELATED: Grant: Health Ministry (France);* UNRELATED: Consultancy: Codman, ev3, MicroVention, Penumbra, Sequent. Christophe Portefaix—RELATED: Grant: Health Ministry (France).* *Money paid to the institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 7, 2012.
- Accepted after revision February 14, 2012.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- The sensitivity and specificity of TOF-MRA compared with DSA in the follow-up of treated intracranial aneurysms
- MRA versus DSA for the follow-up imaging of intracranial aneurysms treated using endovascular techniques: a meta-analysis
- Visualization of Aneurysmal Neck and Dome after Coiling with 3D Multifusion Imaging of Silent MRA and FSE-MR Cisternography
- Impact of the global outflow angle on recanalization after endovascular treatment of middle cerebral artery bifurcation aneurysms
- Balloon-assisted coil embolization and large stent delivery for cerebral aneurysms with a new generation of dual lumen balloons (Copernic 2L)
- Contrast-Enhanced and Time-of-Flight MRA at 3T Compared with DSA for the Follow-Up of Intracranial Aneurysms Treated with the WEB Device
- Detection of aneurysmal subarachnoid hemorrhage 3 months after initial bleeding: evaluation of T2* and FLAIR MR sequences at 3 T in comparison with initial non-enhanced CT as a gold standard
- Follow-up of intracranial aneurysms treated by a WEB flow disrupter: a comparative study of DSA and contrast-enhanced MR angiography
- Inter- and Intrarater Agreement on the Outcome of Endovascular Treatment of Aneurysms Using MRA
- Imaging Follow-Up of Intracranial Aneurysms Treated by Endovascular Means: Why, When, and How?
- Republished: Republished: Rebleeding of a neck remnant in a case of ruptured aneurysm initially treated with coils
- Follow-up of intracranial aneurysms treated by flow diverter: comparison of three-dimensional time-of-flight MR angiography (3D-TOF-MRA) and contrast-enhanced MR angiography (CE-MRA) sequences with digital subtraction angiography as the gold standard
- WEB-DL Endovascular Treatment of Wide-Neck Bifurcation Aneurysms: Long-Term Results in a European Series
- Is Visual Evaluation of Aneurysm Coiling a Reliable Study End Point?: Systematic Review and Meta-Analysis
- Late onset aneurysm development following radiosurgical obliteration of a cerebellopontine angle meningioma
- Is long-term follow-up of adequately coil-occluded ruptured cerebral aneurysms always necessary? A single-center study of recurrences after endovascular treatment
- Rebleeding of a neck remnant in a case of ruptured aneurysm initially treated with coils
- One-Year MR Angiographic and Clinical Follow-Up after Intracranial Mechanical Thrombectomy Using a Stent Retriever Device
- Optimized Angiographic CT Using Intravenous Contrast Injection: A Noninvasive Imaging Option for the Follow-Up of Coiled Aneurysms?
- Late onset aneurysm development following radiosurgical obliteration of a cerebellopontine angle meningioma
- WEB-DL Endovascular Treatment of Wide-Neck Bifurcation Aneurysms: Short- and Midterm Results in a European Study
- Endovascular Treatment of Intracranial Aneurysms: Current Status