
Abstract
BACKGROUND AND PURPOSE: Spread of thrombus material in previously unaffected vessels is a potential hazard of mechanical thrombectomy, but it has not yet been investigated in detail, to our knowledge. Our purpose was to evaluate the frequency and relevance of these events in mTE of M1 occlusions.
MATERIALS AND METHODS: We retrospectively reviewed all patients treated for isolated M1 occlusion between January 2008 and July 2012. Angiographic images were analyzed to assess emboli in anterior cerebral artery branches induced by mTE and associated devices. Recanalization attempts in the ACA were reported as well as technical success and adverse events of rescue therapies. ACA infarcts on follow-up imaging served as a surrogate for clinical relevance. ACA infarcts were quantified volumetrically and assessed visually for involvement of motor or supplementary motor areas.
RESULTS: New ACA emboli occurred in 12 of 105 (11.4%) M1 recanalization procedures and were caused by a stent-retriever in 11 intances. Attempts to recanalize the ACA were made in 6 patients and were deemed technically successful in 5 with no adverse events. We detected 6 (5.7%) new infarcts on follow-up imaging with an average volume of 26.9 cm3. Involvement of motor or supplementary motor areas was seen in 4 (3.8%) cases. Three patients developed ACA infarcts despite successful endovascular ACA recanalization.
CONCLUSIONS: The frequency of ACA emboli in mTE of M1 occlusions is relevant, causing ACA infarcts in 5.7% of patients; 3.8% of emboli were likely to hamper motor-function recovery. Endovascular recanalization of major ACA branches reduced the incidence of infarcts with no adverse events.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- IVT
- intravenous thrombolysis
- mTE
- mechanical thrombectomy
- RECOST
- Rescue, Combined, and Stand-Alone Thrombectomy
- TICI
- Thrombolysis in Cerebral Infarction
Mechanical thrombectomy is an effective tool for recanalization of occluded cerebral vessels in acute stroke treatment. This is especially true because stentlike retrievers were added to the already-existing armamentarium of devices, allowing even higher success rates.1 Recently this observation was proved in a randomized trial comparing the Solitaire FR stent-retriever (Covidien Neurovascular, Irvine, California) and the Merci thrombectomy device (Merci retriever; Concentric Medical, Mountain View, California).2 The improved morphologic results translated into a significantly better clinical outcome 3 months after the ischemic event. Similar results were shown in the Thrombectomy Revascularization of Large Vessel Occlusions in Acute Ischemic Stroke Trial comparing the Trevo Pro Retriever (Stryker, Kalamazoo, Michigan) and the Merci thrombectomy device.3
Even though angiographic and, in part, clinical results of mTE are promising, adverse events might occur. The main interest is in intracranial hemorrhage, but embolism to previously unaffected vessels is another adverse event of catheter-directed treatment that might hamper patient recovery. Although this also happens in IVT when thrombus material resolves and fragments are carried into peripheral vessels, the phenomenon of thrombus loss can be observed directly in endovascular treatment and therefore attracts attention. Due to improper embedding of the thrombus into the device, fragments may embolize not only into the downstream arterial territory but also into side branches proximal to the primary occlusion site. The aim of our study was to determine the frequency of thrombus loss into proximal vessels and to assess the relevance of this phenomenon in mTE of middle cerebral artery occlusion.
Materials and Methods
Ethical Adherence
The local ethics committee approved this retrospective data analysis.
Patient Selection
From a comprehensive data base of all acute stroke treatments performed in our institution since 2008, we selected patients with an embolic occlusion of the M1 segment without pre-existing emboli in the ACA territory. All treatments were performed between January 2008 and July 2012. Cases were excluded if the ipsilateral A1 segment was severely hypoplastic or absent, the posttreatment angiographic run did not allow assessment of the peripheral MCA and ACA branches, or posttreatment imaging was not available.
Treatment Protocol
Patients referred for mechanical recanalization had an acute onset of clinical symptoms caused by cerebral ischemia and a relevant neurologic deficit (NIHSS score ≥ 4). In case of fluctuating or progressive neurologic deficits, we also treated patients with minor symptoms (NIHSS score < 4). Patients with minor stroke and large-vessel occlusion were included because this subgroup is known to be at a significant risk of secondary deterioration and poor outcome despite minor symptoms at presentation.4,5 Patient selection did not include a strict age limit. In elderly patients, the decision about interventional treatment was made on an individual basis, considering the prestroke quality of life, comorbidities, and the assumed will of the patient. Patients were treated within a time window of 8 hours. Exceptions were made for patients beyond this time window in case of small infarct size and severe stroke symptoms suggesting a relevant proportion of salvageable brain tissue and good collaterals.6,7 Intracranial hemorrhage was ruled out by using CT or MR imaging, and large-vessel occlusion was confirmed by CTA or MRA. Because patients were referred from several hospitals, there was no uniform imaging protocol.
Intravenous rtPA was given before the procedure in a small subset of patients on the basis of generally accepted inclusion and exclusion criteria for IVT. The referring neurologist was the decision-maker regarding the use of systemic fibrinolysis. Patients in whom stent placement was likely to be necessary were pretreated with a loading dose of 500 mg acetylsalicylic acid and 600 mg clopidogrel and did not receive IVT to reduce the risk of hemorrhage. If a patient did not receive a loading dose but stent placement had to be performed, 500 mg acetylsalicylic acid was applied intravenously followed by 600 mg clopidogrel via a nasogastric tube.
Procedures were routinely performed with the patient under general anesthesia by 6 experienced interventional neuroradiologists. An 8F guide catheter was used mainly in combination with an intermediate catheter. We rarely used a balloon-guide catheter. The occluded vessel segment was catheterized with a 0.021-inch inner diameter microcatheter by using a 0.014-inch microguidewire. A device for mTE was chosen at the discretion of the operator. Under fluoroscopy, the mTE device was inserted starting beyond the assumed level of vessel occlusion and deployed by withdrawal of the microcatheter. After a minimum device incubation time of 3 minutes, a DSA run was performed. Two milligrams of glycerol trinitrat was slowly injected intra-arterially through the guide catheter to avoid vasospasm during device withdrawal. Arterial hypotension was pharmacologically compensated for by intravenous injection of cafedrine hydrochloride/theodrenalinhydrochlorid. Under fluoroscopy, the microcatheter and the deployed thrombectomy device were withdrawn with simultaneous aspirtion of the guide or extension catheter, occasionally under proximal balloon occlusion.
In January 2012, we introduced “distal aspiration” into our treatment concept. The intermediate catheter was positioned in the M1 segment before device removal to reduce the distance of unprotected device retraction and allow aspiration in the proximity of the thrombus. After removal of the device and careful purging of the guide or extension catheter, the result of mTE was assessed angiographically. In case of persistent occlusion or incomplete recanalization, mTE was repeated with the same or another device. If recanalization could not be achieved after several mTE maneuvers, the procedure was either aborted or continued by using angioplasty and/or stents. In case of an intraprocedural ACA occlusion, endovascular recanalization was attempted if a significant proportion of the ACA territory was affected and collateral flow was deemed insufficient. Recanalization of the ACA was achieved by either permanent implantation of a self-expanding stent or mTE, depending on the vessel course and site of occlusion.
After mTE, the patient was kept sedated and ventilated until the next day to allow precise management of blood pressure, tolerating a maximum peak systolic value of 130–150 mm Hg.
Imaging was performed within the following 24–48 hours by using either CT or MR imaging.
Data Evaluation
Baseline clinical data included age, sex, NIHSS score, time from symptom onset to treatment, and etiology of the embolic cerebral vessel occlusion. Clinical outcome was measured by using the modified Rankin Scale score at 90 days. The overall incidence of parenchymal hemorrhage types I and II according to the European Cooperative Acute Stroke Study definition was assessed.8 We also reported on isolated SAH distinguishing focal SAH located around the site of infarction and diffuse SAH spreading to the contralateral hemisphere or infratentorially.
For the purpose of this study, we evaluated all treatments for the arterial access system, the type of thrombectomy devices, the number of passes performed, and the final recanalization result applying the TICI score.9 TICI 2b and 3 were defined as successful recanalization. We recorded all treatment-induced ACA branch occlusions, the time point of occurrence, and the device used during the same thrombectomy maneuver. Rescue strategies to recanalize the ACA territory were described as well as their results by using the TICI score.
Posttreatment imaging was assessed for new infarcts in the territory of the ipsilateral ACA and eventual involvement of the primary or supplementary motor cortex area. Infarct volume was measured after manual segmentation by using OsiriX 4.1 Imaging Software (http://www.osirix-viewer.com).
Statistical Analysis
We compared the influence of different mTE devices and the impact of distal aspiration on the frequency of ACA emboli by using the Fisher exact test. The same test was applied to evaluate the influence of additional rtPA on intracranial hemorrhage. A P value ≤ .05 was defined as statistically significant. All analyses were performed with STATA/IC 11.2 for Windows software (StataCorp, College Station, Texas).
Results
Our hospital is a large tertiary referral center for neurointerventions, providing service for 13 regional stroke units on a 24/7 basis. In the defined period, we performed 682 endovascular recanalization procedures. This number represents 3% of all patients treated for ischemic stroke in the referring hospitals. Of 122 patients, 17 had to be excluded because of insufficient imaging material or an ipsilateral hypoplastic A1 segment. Of the remaining 105 patients, baseline clinical data are summarized in Table 1. Overall successful recanalization of the M1 territory was achieved in 97 patients with a median number of 2 passes (range, 1–8). In 29 (27.6%) patients, an additional intracranial balloon angioplasty with or without stent placement was necessary to achieve a sufficient recanalization result. Table 2 summarizes types of thrombectomy devices and the number of passes performed per device.
Summary of clinical data
Summary of the types of devices used for mTE and the number of passes performed per device
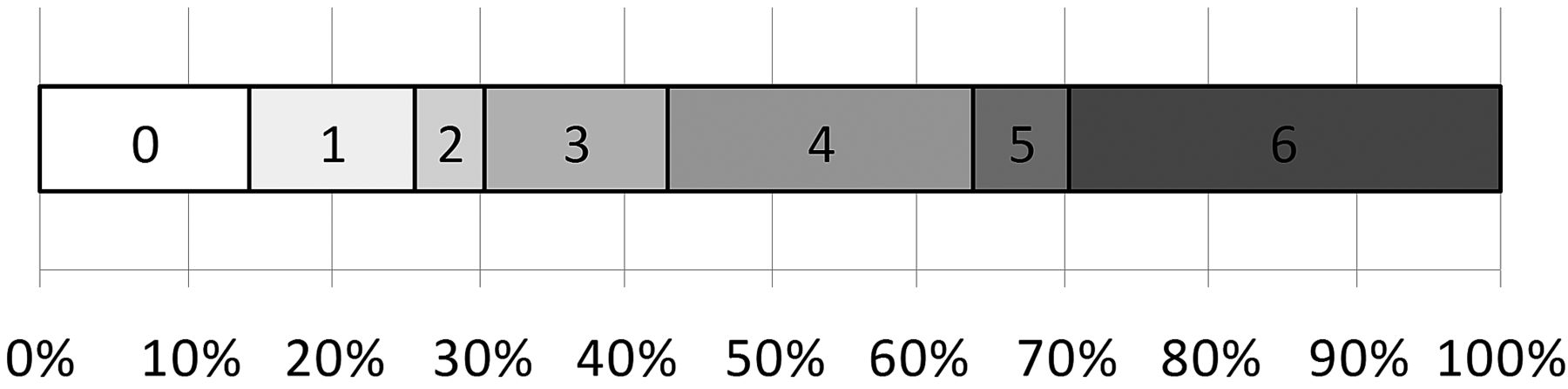
Parenchymal hemorrhage occurred in 14 (13.3%) patients, with 3 (2.9%) type I and 11 (10.4%) type II hemorrhages. An additional 17 (16.2%) patients experienced isolated SAH with 15 (14.2%) focal and 2 (1.9%) diffuse distributions. The rate of any intracranial hemorrhage on imaging was not significantly increased with additional rtPA treatment (P = .720). Clinical outcome at 3 months is shown in Fig 1.

Distribution of modified Rankin Scale scores at 90 days.
Overall we detected 12 (11.4%) new ACA branch occlusions. ACA embolism occurred during the first 2 thrombectomy passes on 9 occasions. In 11 patients, this was caused by a stent retriever. One subcortical branch occlusion was only visible on the final overview run and could not be assigned to a specific device. On-line Table 1 summarizes the procedures resulting in an embolic ACA occlusion. Statistical analysis of the frequency of thrombus loss per pass did not reveal significant differences among devices (P = .212). The rate of ACA emboli was 3.3% (1 of 30) with distal aspiration compared with 14.6% (11 of 75) without distal aspiration. The observed difference was not statistically significant (P = .172).
ACA territory recanalization was attempted in 6 patients either by stent angioplasty, stent-retriever thrombectomy, or a combination of both. The procedure was technically successful in 5 and uneventful in all intances. One patient with an ACA recanalization procedure developed SAH predominantly in the Sylvian fissure and along the MCA cistern. This was attributed to the M1 thrombectomy rather than ACA recanalization.
Follow-up imaging was performed by CT in 78 and MR imaging in 27 cases. It revealed 6 (5.7%) new infarcts in the ACA territory. Involvement of the primary and/or supplementary motor cortex area was seen in 4 (3.8%) patients. Three patients with new infarcts deteriorated clinically by >4 points on the NIHSS (2.8%). Three of 5 patients with successful ACA recanalization did not develop new infarcts. On-line Table 2 provides an overview of the ACA territory embolic occlusions, rescue therapy, and imaging and clinical outcome.
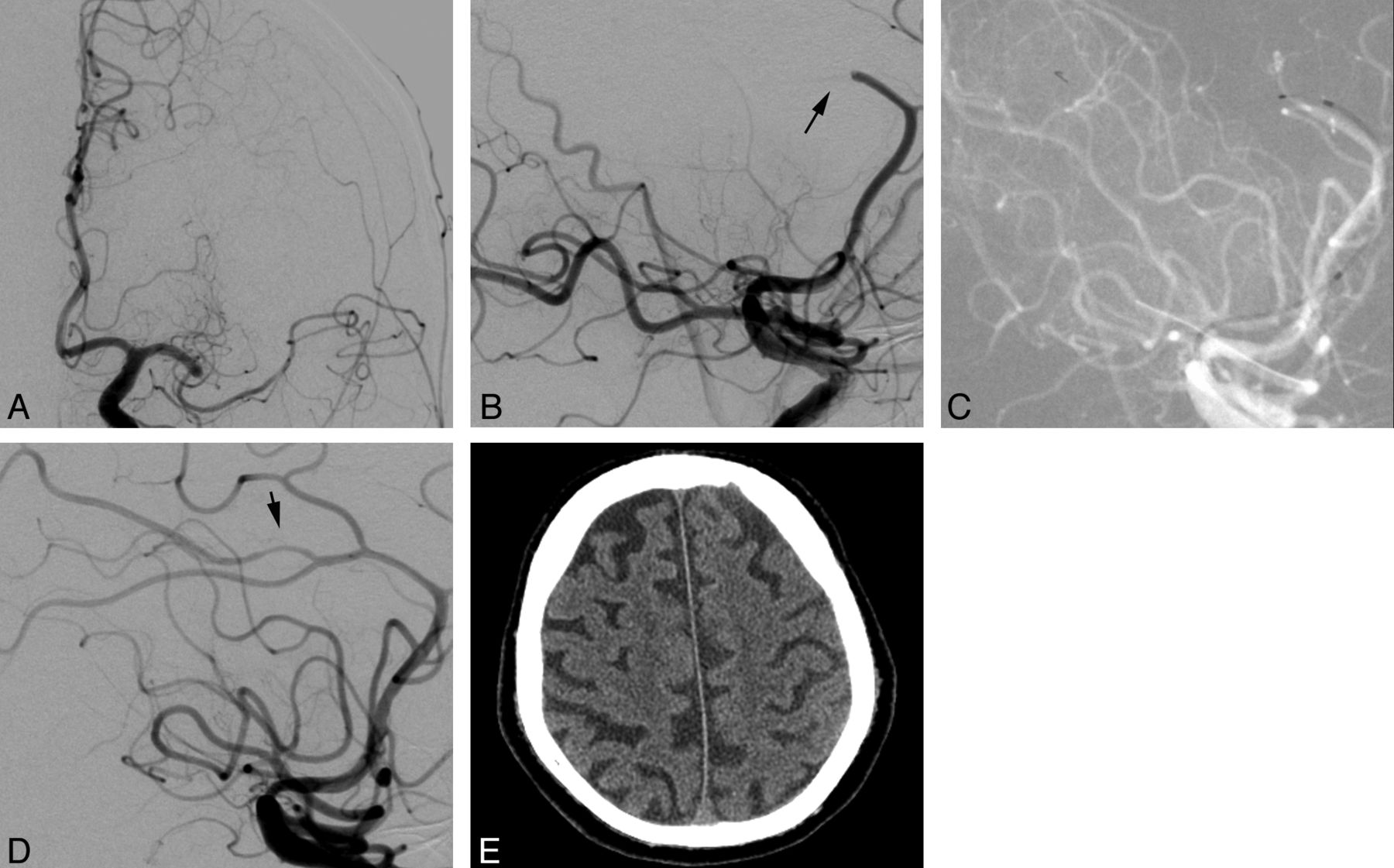
Figure 2 shows an illustrative case of embolic ACA occlusion and recanalization.

A, Patient 5 was referred for endovascular treatment of an acute left M1 occlusion. B, After 4 thrombectomy passes, the inferior trunk of the MCA was recanalized at the expense of an acute embolic occlusion of the pericallosal artery (arrow). C, Recanalization of the pericallosal artery was attempted by mTE after complete recanalization of the MCA territory. D, The final angiographic run confirmed complete recanalization of the pericallosal artery and minor vasospasm (arrow). E, An ACA infarct was excluded on CT imaging.
Discussion
The issue of embolism into the ACA territory in the setting of MCA recanalization is important because this may lead to clinical sequelae, which are clearly treatment-induced. The phenomenon is known to occur in intra-arterial recanalization procedures. A pooled analysis of the Interventional Management of Stroke I and II data proved an incidence of 1.6% for intra-arterial fibrinolysis of MCA occlusions.10 Mechanical thrombus removal increases the chance of successful recanalization at the expense of a higher risk of inadvertently spreading thrombus material. The first FDA-approved device for mechanical embolectomy was the Merci retriever. Within the approval study, 3 new emboli were detected in 141 patients. All were located in the ACA and occurred during recanalization of MCA occlusions.11 A proximal approach to mechanically remove intracranial thrombus material is represented by the Penumbra system (Penumbra, Alameda, California). Animal experiments suggested lower rates of emboli for proximal compared with distal devices but also lower success rates in terms of recanalization.12 The Penumbra Pivotal trial reported only 1 event in 125 anterior and posterior circulation acute stroke treatments.13
Recently the first stent-retriever, Solitaire FR, was FDA-approved after superiority over the Merci device was definitively proved in the Solitaire Flow Restoration Device versus the Merci Retriever in Patients with Acute Ischemic Stroke Trial.2 Data on the frequency of emboli in previously unaffected vessel territories are not yet available, but the European prospective RECOST study provided some information regarding this adverse event.14 Fifty patients with acute embolic vessel occlusion in the anterior and posterior circulation were treated with the Solitaire FR, and 4 (8%) symptomatic occlusions of previously unaffected vessels were observed. The findings of the RECOST study are in line with our observation of 11.4% new ACA emboli. Nearly all events occurred with the use of stent retrievers exhibiting a high capability to mobilize and remove thrombus material. The higher efficacy seems to be associated with a higher probability of thrombus loss. Approximately half of the affected patients developed new infarcts, but only one-third showed involvement of primary or supplementary motor areas, suggesting an impact on motor function recovery. Most patients with successful ACA recanalization did not develop new infarcts. All ACA recanalization treatments were uneventful. From our results, we conclude that recanalization should be attempted if collateralization is insufficient and treatment seems technically feasible. With the introduction of distal aspiration, we observed fewer embolic events in the ACA, but the advantage of this new concept could not be proved yet.
Clinical observations are limited to the description of the phenomenon per se and the impact on patient outcome. Experimental animal studies offer the opportunity to gain insight into the whole process of thrombectomy by using stained thrombus material. Animal studies proved that passage of the occluded vessel segment and deployment of the Catch system (Balt, Montmorency, France) and the Merci device were associated with rates of distal emboli as high as 31.8% and 28.6%. Thromboembolic events during retraction occurred in 40% and 10% of attempts, respectively.15 Three years later the same group tested the Solitaire FR in an identical setting and did not observe any distal emboli during passage, deployment, and retraction.16 These results suggest differences between devices and a clear superiority of the stent-retriever approach in terms of embolic events. In our case series as well as in the RECOST study, loss of thrombus material occurred with the use of stent retrievers and we did not find any statistical difference between devices. Several factors may contribute to this divergent finding in a clinical context. First, the number of embolic events per device was low; this feature increased the chance of a type 2 statistical error. Second, the swine animal model has a straight-vessel anatomy. Retraction through the narrow and elastic human carotid siphon curves results in a nonlinear transfer of traction forces, often translating into undesired acceleration of device movement. This increases the probability of thrombus loss. The problem might be overcome by positioning large-lumen intermediate catheters close to the site of occlusion up to the M1 segment with the aim of reducing the distance of unprotected device retraction and allowing a more controlled transfer of traction forces. Third, the animal model benefits from artificial visibility of the thrombus, allowing precise coverage over the whole length.
Angiographic assessment in acute stroke clearly depicts the proximal occlusion site, whereas the distal end of the thrombus usually remains obscured. The only way to visualize thrombus length during angiography is contrast injection after microcatheter passage. We intentionally avoided this because contrast injection distal to the occlusion site might increase the risk of hemorrhage.17 This may lead to—at least in some cases—a less precise positioning of the retriever or suboptimal device selection in terms of length and diameter. Fourth, experimental thrombi differ in their composition compared with human fibrin-rich cardiac emboli. Therefore, they exhibit different mechanical properties that influence their behavior during mTE.
Another animal study testing the Solitaire FR confirmed that no emboli occurred during positioning and retraction but fragmentation of the thrombus at the tip of the guide catheter was observed in some cases.18 The fragments were aspirated successfully on all occasions, but this mechanism might still contribute to undesired embolism. The animal experiment underlines the necessity of careful aspiration and purging of the guide system as well as the advantage of a large-lumen guide catheter. This is especially important in cases with a high thrombus load when thrombus size is large enough to obstruct the guide catheter. In addition, the use of proximal balloon occlusion is widespread in acute stroke treatment. In animal experiments, proximal flow arrest during mTE with distal devices reduced the risk of embolic events.12 So far the superiority was not clearly demonstrated in clinical studies. Higher stiffness and increased expense are the drawbacks of balloon-guide catheters. In our case series, most treatments were performed without proximal occlusion, not allowing valid statistical analysis of the possible impact on the frequency of peripheral emboli.
Limitations of the Study
The main limitation of the study is that embolization to previously unaffected vessel territories represents only a part of the topic. Downstream emboli caused by thrombus fragmentation may also cause new ischemia in tissue that was previously sufficiently supplied by leptomeningeal collaterals. Distal emboli can only be depicted when pretreatment imaging clearly shows contrast filling via collaterals either in CT angiography or DSA images. Because this scenario is rare, it is very likely that assessment of downstream emboli remains arbitrary. Even if embolic occlusion of collaterals is detected, the impact on final infarct size is not clear due to a lack of thresholds allowing a precise discrimination between sufficient and insufficient collaterals.
Posttreatment imaging was mainly CT-based in our study, which is less sensitive for small infarcts compared with MR imaging. Therefore, the incidence of new infarcts might be higher than reported.
Conclusions
New ACA emboli are not a rare event in mTE of MCA occlusions, even with new-generation stent retrievers. This adverse event led to 5.7% new infarcts. Endovascular recanalization of occluded major ACA branches reduced the risk of ischemia with no adverse effects and can be attempted in cases with poor collaterals and good accessibility.
Effective strategies to avoid thrombus loss are warranted. Possible components of the solution are advanced angiographic imaging techniques to improve visualization of the thrombus, low-profile microcatheters to prevent fragmentation during passage, and modified retriever designs for a better encasement of the thrombus. In terms of arterial access, positioning of a large-lumen intermediate catheter in the proximity of the occlusion reduces the distance of device retraction and probably has the potential to reduce the frequency of thrombus loss. In addition, balloon-guided catheters might have a positive impact due to effective flow arrest and sufficient aspiration.
Footnotes
Disclosures: Wiebke Kurre—UNRELATED: Consultancy: Phenox, Payment for Lectures (including service on Speakers Bureaus): Codman, Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Phenox. Marta Aguilar Pérez—UNRELATED: Consultancy: Phenox, Comments: performed preclinical animal experiments to test devices currently under development. Elisabeth Schmid—UNRELATED: Payment for Lectures (including service on Speakers Bureaus): Bayer Vital. Hansjörg Bäzner—UNRELATED: Payment for Lectures (including service on Speakers Bureaus): Biogen Idec, Bayer Vital, UCB Pharma, Boehringer Ingelheim, Comments: Speakers Bureaus. Hans Henkes—UNRELATED: Board Membership: Codman, Comments: modest payment for participation in board meetings and compensation for travel expenses, Consultancy: ev3, Sequent Medical, Comments: occasional consultation and modest payment, Grants/Grants Pending: Codman;* Payment for Lectures (including service on Speakers Bureaus): ev3, Codman, Comments: modest payment for lectures, Patents (planned, pending or issued): Phenox, Comments: submission of intellectual property as coinventor, Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: ev3, Codman, phenox, Other: B. Braun,* Comments: sponsoring of open access for publications, Other Relationships: cofounder of Dendron GmbH, Bochum, Germany, cofounder of Phenox GmbH, Bochum, Germany; proctor (Pipeline) for ev3/Covidien; workshop for Balt Extrusion. *Money paid to the institution.
Previously presented in part at: Annual Meeting of the American Society of Neuroradiology and the Foundation of the ASNR Symposium, April 21–26, 2012; New York, New York.
REFERENCES
- Received August 21, 2012.
- Accepted after revision November 15, 2012.
- © 2013 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison between transradial and transfemoral mechanical thrombectomy for ICA and M1 occlusions: insights from the Stroke Thrombectomy and Aneurysm Registry (STAR)
- Predictors of distal embolization during thrombectomy for anterior circulation large vessel bifurcation occlusion stroke
- Mechanical thrombectomy for the treatment of primary and secondary anterior cerebral artery occlusions: insights from STAR
- Predictors of tissue infarction from distal emboli after mechanical thrombectomy
- Impact of stent-retriever tip design on distal embolization during mechanical thrombectomy: a randomized in vitro evaluation
- Impact of stent-retriever tip design on distal embolization during mechanical thrombectomy: a randomized in vitro evaluation
- Mechanical Thrombectomy for the Treatment of Anterior Cerebral Artery Occlusion: A Systematic Review of the Literature
- A Meta-analysis of Combined Aspiration Catheter and Stent Retriever versus Stent Retriever Alone for Large-Vessel Occlusion Ischemic Stroke
- A review of endovascular treatment for medium vessel occlusion stroke
- Novel Human Acute Ischemic Stroke Blood Clot Analogs for In Vitro Thrombectomy Testing
- Time-to-Maximum of the Tissue Residue Function Improves Diagnostic Performance for Detecting Distal Vessel Occlusions on CT Angiography
- Modelling the impact of clot fragmentation on the microcirculation after thrombectomy
- Anterior cerebral artery embolism during thrombectomy increases disability and mortality
- Beyond Large Vessel Occlusion Strokes: Distal Occlusion Thrombectomy
- Initial clinical experience using the two-stage aspiration technique (TSAT) with proximal flow arrest by a balloon guiding catheter for acute ischemic stroke of the anterior circulation
- Wire escalation in emergent revascularization procedures of internal carotid artery occlusions: the use of high tip stiffness microguidewires
- Combined proximal balloon occlusion and distal aspiration: a new approach to prevent distal embolization during neurothrombectomy
- An in vitro evaluation of distal emboli following Lazarus Cover-assisted stent retriever thrombectomy
- Initial experience with a new distal intermediate and aspiration catheter in the treatment of acute ischemic stroke: clinical safety and efficacy
- Mechanical Thrombectomy of Distal Occlusions in the Anterior Cerebral Artery: Recanalization Rates, Periprocedural Complications, and Clinical Outcome
- Stent retriever thrombectomy with the Cover accessory device versus proximal protection with a balloon guide catheter: in vitro stroke model comparison
- Risk of distal embolization with stent retriever thrombectomy and ADAPT
- Distal aspiration with retrievable stent assisted thrombectomy for the treatment of acute ischemic stroke