
Abstract
BACKGROUND AND PURPOSE: A performance of forced arterial suction thrombectomy was not reported for the treatment of acute basilar artery occlusion. This study compared revascularization performance between intra-arterial fibrinolytic treatment and forced arterial suction thrombectomy with a Penumbra reperfusion catheter in patients with acute basilar artery occlusion.
MATERIALS AND METHODS: Fifty-seven patients with acute basilar artery occlusion were treated with intra-arterial fibrinolysis (n = 25) or forced arterial suction thrombectomy (n = 32). Baseline characteristics, successful revascularization rate, and clinical outcomes were compared between the groups.
RESULTS: Baseline characteristics, the frequency of patients receiving intravenous recombinant tissue plasminogen activator, and mean time interval between symptom onset and femoral puncture did not differ between groups. The forced arterial suction thrombectomy group had a shorter procedure duration (75.5 minutes versus 113.3 minutes, P = .016) and higher successful revascularization rate (88% versus 60%, P = .017) than the fibrinolysis group. Fair outcome, indicated by a modified Rankin Scale 0–3, at 3 months was achieved in 34% of patients undergoing forced arterial suction thrombectomy and 8% of patients undergoing fibrinolysis (P = .019), and the mortality rate was significantly higher in the fibrinolysis group (25% versus 68%, P = .001). Multiple logistic regression analysis identified the forced arterial suction thrombectomy method as an independent predictor of fair outcome with adjustment for age, sex, initial NIHSS score, and the use of intravenous recombinant tissue plasminogen activator (odds ratio, 7.768; 95% CI, 1.246–48.416; P = .028).
CONCLUSIONS: In acute basilar artery occlusion, forced arterial suction thrombectomy demonstrated a higher revascularization rate and improved clinical outcome compared with traditional intra-arterial fibrinolysis. Further clinical trials with the newer Penumbra catheter are warranted.
ABBREVIATIONS:
- BAO
- basilar artery occlusion
- IA
- intra-arterial
- FAST
- forced arterial suction thrombectomy
The prognosis for acute basilar artery occlusion (BAO) is dismal.1,2 Early recanalization is one of the most important prognostic factors for an improved outcome in BAO.3,4 Intravenous infusion of recombinant tissue plasminogen activator is, however, not fully effective for the recanalization of acute BAO.5,6
Endovascular treatment is an emerging therapeutic option for acute BAO. Previously, local infusion of fibrinolytic agents was the only available therapy.2,7,8 Although intra-arterial fibrinolysis achieved a much higher recanalization rate than intravenous rtPA, clinical outcome did not differ between the treatments.9 Recently, several mechanical thrombectomy devices have been developed and applied in clinical studies.10⇓⇓–13 However, thus far, no device has been proved to improve clinical outcomes, and the optimal strategy for acute BAO treatment has not yet been established.
The Penumbra System (Penumbra, Alameda, California) is an endovascular device designed to reduce clot burden in acute ischemic stroke due to large cerebral artery occlusion. Although many clinical trials have been conducted using the device, data concerning the use of the Penumbra System in acute BAO are still scarce.10 Forced arterial suction thrombectomy (FAST), which is a modification of the standard Penumbra System, is used as a mechanical recanalization method for ischemic stroke.14,15 Unlike the standard Penumbra System, the FAST method involves only a reperfusion catheter. Negative pressure via forceful pulling of a syringe can keep an embolus aspirated at the catheter tip. This method has been reported to be simpler and faster than the standard Penumbra System and has been applied clinically.14,16,17
We postulated that the FAST method may improve the clinical outcome of acute BAO compared with the traditional endovascular treatment method of local fibrinolysis. In the present study, we evaluated the revascularization performance and clinical outcomes between intra-arterial (IA) fibrinolytic treatment and the FAST method and compared them with the Penumbra reperfusion catheter in patients with acute BAO.
Materials and Methods
Study Population
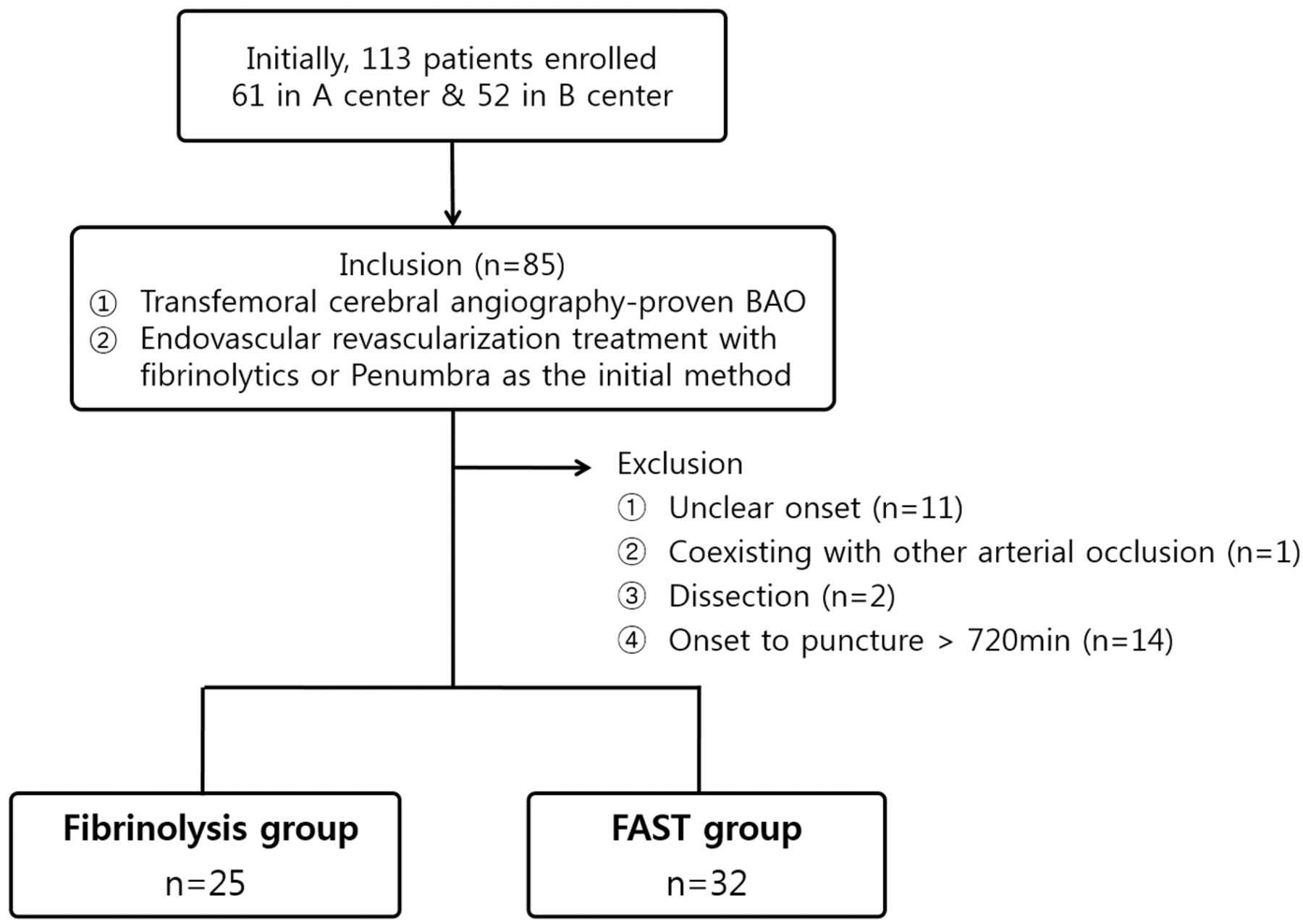
This retrospective study involved registry data bases and additional imaging analyses. All patients or their caregivers gave informed consent for each endovascular treatment. From registries of 2 university hospitals in Korea, 113 consecutive patients who had BAO with or without continuous vertebral artery occlusion and underwent revascularization treatments between March 2006 and June 2013 were enrolled (Fig 1). Among them, those who had transfemoral cerebral angiography–proved BAO and underwent IA revascularization with either fibrinolysis or mechanical thrombectomy by using FAST as the initial IA treatment method for acute BAO were included. Patients were excluded under the following conditions: 1) their onset of symptoms was unclear, 2) another cerebral artery was occluded, 3) onset-to-puncture time exceeded 720 minutes, or 4) their stroke etiology was dissection. We grouped patients into a fibrinolysis group and a FAST group, depending on the initial method of endovascular treatment. Other endovascular methods for rescue therapy were permitted.

Flow diagram of the current study.
Protocol
Brain parenchyma and cervicocerebral arteries were evaluated by CT or MR imaging as early as possible before IA treatment. The BAO as a treatment target was confirmed by selective cerebral intra-arterial digital subtraction angiography. Patients received either endovascular revascularization treatment following intravenous thrombolysis or endovascular treatment alone. Local intra-arterial fibrinolysis was performed by using an infusion microcatheter inserted into the middle of the clots. Fibrinolytic agents included rtPA, urokinase, abciximab, and tirofiban. All FAST methods were performed by using the Penumbra aspiration catheter (first-generation). Using a transfemoral approach, we placed the guide catheter into the dominant or most navigable vertebral artery. After we placed the reperfusion catheter immediately proximal to the clot, we applied negative pressure at the distal tip by continuous suctioning with a 50-mL syringe. The catheter was then smoothly pulled back. The interventional procedure was terminated when recanalization was achieved or according to a consensus between neurologists and neurointerventionists.
Outcome Measurements
Baseline patient data, including vascular risk factors, stroke etiology, laboratory and imaging variables, and initial neurologic severity scales, were retrieved from each stroke registry data base and electronic health records. Imaging data were collected from the PACS of each hospital. Procedural duration was defined as the time between the placement of a guide catheter proximal to the target artery and final angiography of the target artery. Revascularization was measured by the Thrombolysis in Cerebral Infarction score. Successful revascularization was defined as a TICI score of 2b (perfusion ≥ 50%) or 3. Functional outcomes were measured by using the modified Rankin Scale and mortality at 3 months. Fair outcome at 3 months was defined as an mRS score of 0–3.
Statistical Analysis
Univariate analyses were performed by using the t test for continuous variables and the χ2 test for nonparametric variables. Logistic regression analysis was used to evaluate whether the FAST method was an independent predictor of fair outcomes at 3 months. Two-sided P values < .05 were considered significant. Statistical analyses were performed by using a commercially available software package (SPSS, Version 17.0 for Windows; IBM, Armonk, New York).
Results
Ultimately, 57 patients were included in the study: 25 in the fibrinolysis group and 32 in the FAST group. Baseline characteristics were similar between groups (Table 1). Mean age, the frequency of males, and the mean initial National Institutes of Health Stroke Scale score did not differ significantly between groups. The frequency of patients who underwent intravenous rtPA and the mean time interval between symptom onset and femoral puncture also did not differ between groups.
Baseline demographics, neurologic deficits, and hyperacute treatment status
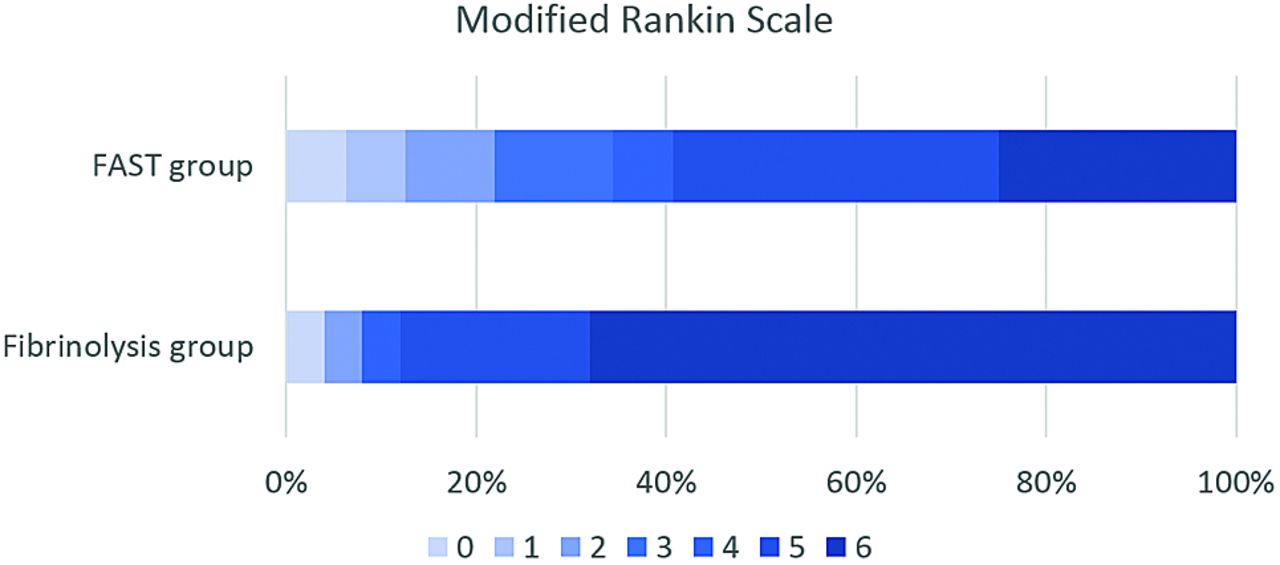
Procedural and clinical outcomes are presented in Table 2. Urokinase was most frequently used for primary IA fibrinolysis (88%; mean, 240,000 U). Tirofiban and rtPA were used in a small number of patients who underwent primary IA fibrinolysis. In patients who underwent the primary FAST procedure, the Penumbra reperfusion catheter 041 was most frequently used (29 cases), followed by the Penumbra reperfusion catheter 032 (3 cases). Furthermore, the Penumbra reperfusion catheter 026 (2 cases) was used only for rescue therapy in the fibrinolysis group. A separator was not used in any of the cases in both the hospitals. The median number of passes performed with the Penumbra reperfusion catheter was 2 (interquartile range, 1–3). The mean procedural duration was significantly shorter in the FAST group than in the fibrinolysis group (76 minutes versus 113 minutes, P = .016). Successful revascularization was achieved at a higher rate in the FAST group than in the fibrinolysis group (88% versus 60%, P = .017). The rate of fair outcome at 3 months was significantly higher in the FAST group than in the fibrinolysis group (36% versus 8%, P = .015), while the mortality rate was significantly higher in the fibrinolysis group (23% versus 68%, P = .001; Fig 2). A multiple logistic regression model revealed that the FAST method was an independent predictor of fair outcome with adjustment for age, sex, initial NIHSS score, and the infusion of intravenous rtPA (odds ratio, 7.768; 95% CI, 1.246–48.416; P = .028; Table 3).
Procedural and clinical outcomes

Modified Rankin Scale of each group. Mortality was significantly reduced when patients underwent endovascular treatment with the FAST method compared with local fibrinolysis.
Multiple logistic regression model for fair outcome at 3 months
Notably, our cohort demonstrated unique characteristics concerning etiology, with atherosclerosis accounting for 50% of patients. Specifically, intracranial stent placement was performed in 19% and 28% of patients in the FAST and fibrinolysis groups, respectively.
Discussion
In this series, we have demonstrated that the FAST method with the Penumbra aspiration catheter can rapidly and effectively restore blood flow in acute BAO and can improve patient outcome in comparison with the traditional IA fibrinolysis method. Better clinical outcome was attributed to higher performance in terms of the revascularization rate and shorter procedural duration. This study is the first to report the efficacy of FAST with the Penumbra reperfusion catheter for the treatment of acute BAO in comparison with IA fibrinolysis.
Acute BAO is a devastating disease, which has been associated with a poor clinical outcome and a high mortality rate.1,2 Treatment with intravenous thrombolysis has been shown to be ineffective for the recanalization of BAO or carotid T occlusion.18,19 On the basis of these limitations, IA injection of fibrinolytic agents has been adopted in standard protocols to treat BAO by many stroke centers, and several randomized trials and numerous case series have demonstrated the benefits of this therapy.2,7,20⇓–22 However, despite the high recanalization rate of intra-arterial fibrinolysis therapy, clinical outcome has not improved.23⇓–25 In the past several years, the introduction of mechanical thrombectomy devices has offered a new option for the treatment of large-vessel occlusion, achieving higher recanalization rates and favorable clinical outcomes.5,10,12,13,26,27
At the start of the endovascular treatment era for BAO, Hacke et al2 published findings in 1988 demonstrating better outcomes and higher survival rates in patients who underwent IA fibrinolysis compared with those who received conventional treatment. On the basis of that report, IA fibrinolysis has been considered an additional treatment option for patients with acute BAO. Recently, several studies have described the performance and efficacy of new mechanical thrombectomy devices for the treatment of BAO. The Merci retrieval system (Concentric Medical, Mountain View, California) was reported as a feasible option for the revascularization of acute BAO, with a recanalization rate of 68%.13 Several studies using the Solitaire retrieval stent (Covidien, Irvine, California) in acute BAO have also been reported.11,12,26⇓⇓–29 The latest studies have achieved revascularization rates of 74%–94% and mortality rates of 22%–32% by using stent-retrieval systems.27,28 Previous studies of endovascular treatment for BAO are summarized in Table 4.10,13,28,30,31
List of revascularization treatment studies for acute basilar artery occlusion
Limited literature is available on use of the Penumbra system for acute BAO. In one study, 12 patients with acute BAO were treated with the standard Penumbra System, with a recanalization rate of 75% and a mortality rate of 33%.10 In the present study, a successful revascularization rate of 79% and a 21% mortality rate were observed with the FAST method. Compared with traditional IA fibrinolysis, which had a successful revascularization rate of 36% and a mortality rate of 68%, outcomes of the FAST method were substantially better. Compared with the standard Penumbra System,10 outcomes appeared to be slightly better, particularly with respect to mortality.
The interpretation of clinical outcomes in our cohort should be cautious. In contrast to cohorts in Western countries, the rate of atherosclerosis among stroke etiologies in our patients was relatively high, up to 50%. After patients were treated with the first endovascular method, intractable severe stenosis still caused the blood flow to be stagnated, necessitating secondary angioplasty and/or stent placement, in approximately 20% of our patients. These additional procedures may delay the final revascularization time and worsen clinical outcomes. On this basis, investigators should consider that intracranial stenosis may be observed often when Asian patients are studied in clinical trials of endovascular treatment. Furthermore, a specific strategy of endovascular treatment should be established for Asian patients.
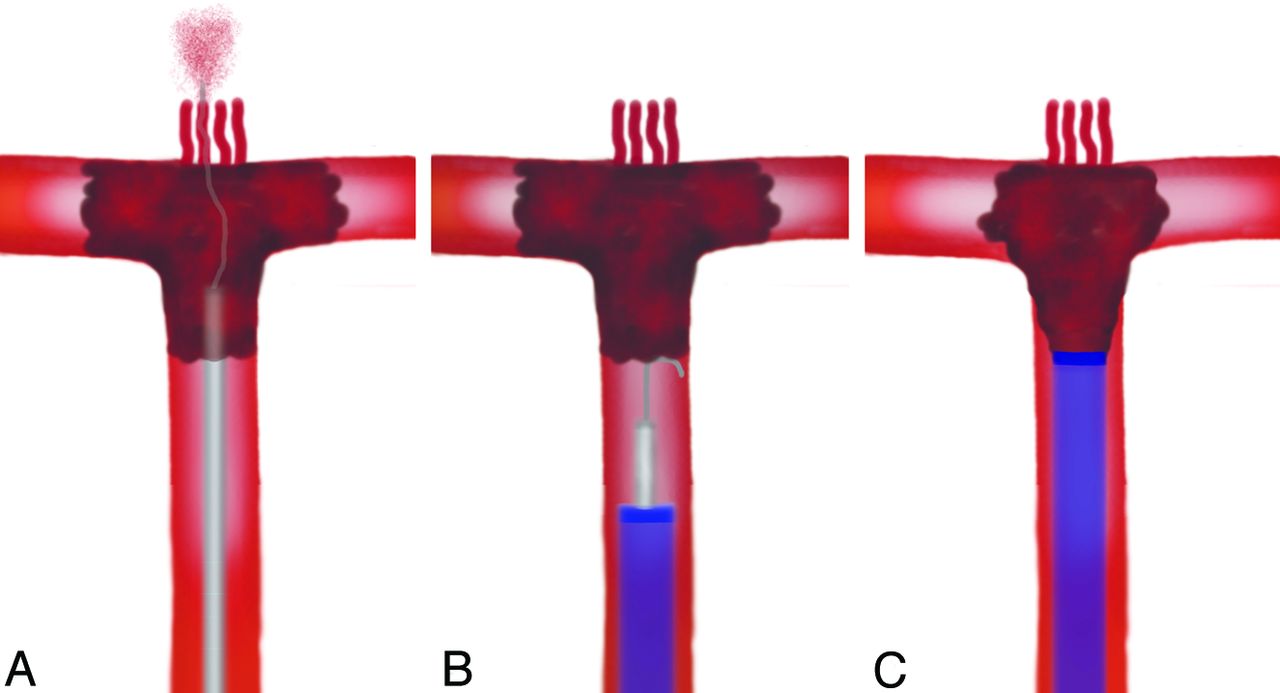
The FAST method is theoretically considered safe because it can avoid inadvertent hemorrhagic complications resulting from the perforation of small arteries originating from the top of the basilar artery (Fig 3). These complications may cause further decrease of mental status and new neurologic deficits. In most cases of BAO, the distal portion above the proximal end of the occlusion is obscured. When a microwire and microcatheter must be navigated to select a posterior cerebral artery, those instruments risk perforating small arteries that are located directly beyond the basilar artery. In the FAST method, the reperfusion catheter is placed immediately proximal to the clot, and negative pressure is applied to aspirate the thrombus. Without any procedure through the thrombus, the risk of perforation is decreased (Fig 3). Recent reports on A Direct Aspiration first Pass Technique (ADAPT) have indicated that it is similar to the FAST method32,33; this technique was especially well-illustrated in a previous report.33 However, the microwire and microcatheter should be selectively traversed because this may cause a subarachnoid hemorrhage, particularly through the perforators at the top of the basilar artery.

Schematic drawings of endovascular treatment for acute BAO. A, Arterial branches are obscured above the occlusive site, and inadvertent hemorrhagic complications can occur when a microwire and microcatheter must be navigated distal to the occlusive site. B and C, The FAST method can avoid this risk because the tip of the Penumbra reperfusion catheter is located only at the proximal end of the clot.
The current study has some limitations. First, it was retrospective. A further comparative study in which both groups are randomly assigned should be performed to confirm our results. Second, both methods were not performed in the same time period. The FAST method was introduced more recently; therefore, progress in the systematic treatment for acute ischemic stroke and the development of newer intracranial microwires and microcatheters may have influenced our results. Nonetheless, major baseline characteristics and clinical events that have a substantial influence on outcomes were similar between the groups. Additionally, data were collected from 2 large hospitals and combined so that unforeseen confounding factors were less likely to have significantly affected our results. Finally, additional treatment for intracranial arterial stenosis was not considered in our analyses. Stenosis of the vertebrobasilar artery system is often observed, especially in Asians. The revascularization methods for stenosis should be applied differently. On the basis of our observations, FAST methods are better suited to embolic BAO than to atherosclerosis.
Conclusions
The FAST method by using the Penumbra reperfusion catheter demonstrated superior performance and was associated with better outcomes in patients with acute BAO compared with intra-arterial fibrinolysis. Moreover, the Penumbra system has recently been enhanced. However, additional clinical trials with newer generation devices, such as Penumbra ACE and MAX, are required to confirm the conclusions of this study.
Footnotes
This work was supported by the new faculty research fund of the Ajou University School of Medicine (J.S. Lee).
References
- Received March 28, 2014.
- Accepted after revision May 28, 2014.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Use and Utility of Aspiration Thrombectomy in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis
- Thromboaspiration technique as first approach for endovascular treatment of acute ischemic stroke: initial experience at nine Italian stroke centers
- Effect of Intracranial Atherosclerotic Disease on Endovascular Treatment for Patients with Acute Vertebrobasilar Occlusion