
Abstract
BACKGROUND AND PURPOSE: EmboTrap II is a novel stent retriever with a dual-layer design and distal mesh designed for acute ischemic stroke emergent large-vessel occlusions. We present the first postmarket prospective multicenter experience with the EmboTrap II stent retriever.
MATERIALS AND METHODS: A prospective registry of patients treated with EmboTrap II at 7 centers following FDA approval was maintained with baseline patient characteristics, treatment details, and clinical/radiographic follow-up.
RESULTS: Seventy patients were treated with EmboTrap II (mean age, 69.9 years; 48.6% women). Intravenous thrombolysis was given in 34.3%, and emergent large-vessel occlusions were located in the ICA (n = 18), M1 (n = 38), M2 or M3 (n = 13), and basilar artery (n = 1). The 5 × 33 mm device was used in 88% of cases. TICI ≥ 2b recanalization was achieved in 95.7% (82.3% in EmboTrap II–only cases), and first-pass efficacy was achieved in 35.7%. The NIHSS score improved from a preoperative average of 16.3 to 12.1 postprocedure and to 10.5 at discharge. An average of 2.5 [SD, 1.8] passes was recorded per treatment, including non-EmboTrap attempts. Definitive treatment was performed with an alternative device (aspiration or stent retriever) in 9 cases (12.9%). Some hemorrhagic conversion was noted in 22.9% of cases, of which 4.3% were symptomatic. There were no device-related complications.
CONCLUSIONS: Initial postmarket results with the EmboTrap II stent retriever are favorable and comparable with those of other commercially available stent retrievers. Compared with EmboTrap II, the first-generation EmboTrap may have a higher first-pass efficacy; however, data are limited by retrospective case analysis, incomplete clinical follow-up, and small sample size, necessitating future trials.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- BGC
- balloon-guide catheter
- FPE
- first-pass efficacy
- LKN
- last known healthy
- sICH
- symptomatic intracerebral hemorrhage
Several landmark trials in 2015 established mechanical thrombectomy with stent retriever devices as the treatment of choice for emergent large-vessel occlusion acute ischemic stroke (AIS) in the anterior circulation. The thrombectomy window was further expanded in certain cases on the basis of the recent Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3 (DEFUSE 3) and Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN) studies.1⇓⇓⇓⇓⇓-7 Various stent retrievers are available in the United States, such as the Solitaire (Medtronic) and Trevo (Stryker), each with different configurations, mechanisms, and clinical outcome profiles.
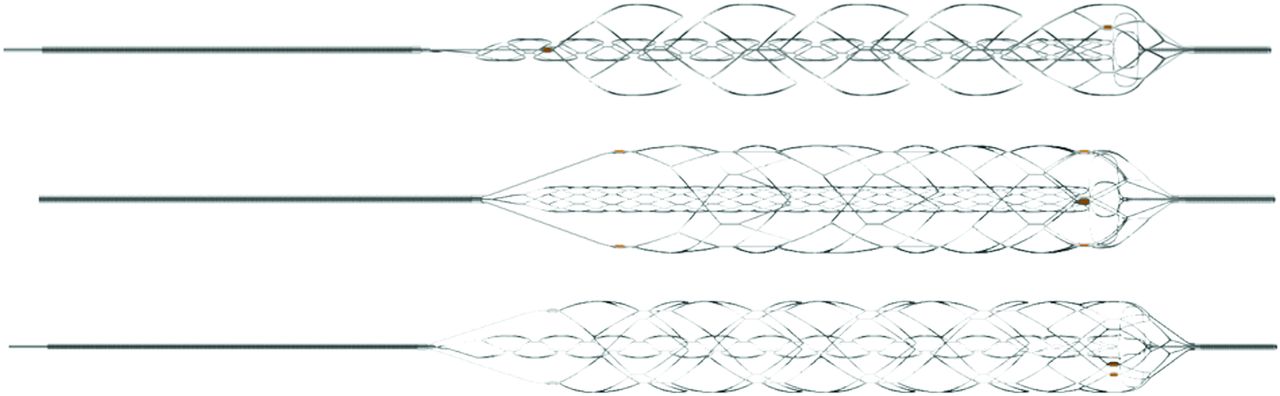
The EmboTrap device (Neuravi/Cerenovus) received FDA approval in May 2018 and is indicated for neurovascular reperfusion within 8 hours of symptom onset in patients experiencing AIS.8 The EmboTrap device has a novel dual-layer construct designed to improve clot engagement and a distal mesh designed to reduce distal emboli. The Analysis of Revascularization in Ischemic Stroke with EmboTrap (ARISE II) was an open-label, single-arm, multicenter, prospective clinical study that evaluated the safety and efficacy of EmboTrap, the first-generation EmboTrap device.8 The EmboTrap II stent retriever is a recent iteration that incorporates a few changes, including the following: 1) a double proximal marker to allow a more precise stent placement, and 2) an increase of outer cages from 3 to 5 to potentially improve the ability of the device to capture clots during device retraction (Fig 1).9

Structure of the EmboTrap II device. Three different angles of the EmboTrap II device (the second is rotated 90° and third is rotated 45° further). Courtesy of Cerenovus, part of DePuy Synthes Products, Inc.
To date, only 1 single-center study has evaluated EmboTrap II, with a relatively small sample size.9 In this study, we present the first prospective multicenter experience with the EmboTrap II stent retriever.
MATERIALS AND METHODS
Study Design
The study was a prospective registry of all patients treated with EmboTrap II at 7 academic neurointerventional centers from May 2018 to October 2019 following FDA approval of the device. These patients were not enrolled in any other studies (eg, the ARISE II trial). All patients older than 18 years of age with emergent large-vessel occlusion AIS who underwent endovascular therapy with at least 1 EmboTrap II deployment (when Embotrap II was used as the initial device) were included in the study. For each patient, demographic, baseline clinical, procedural, and clinical and radiologic outcome data were collected. Institutional review board approval was obtained for the collection and review of patient data for this study (H-33379).
Procedural Technique
All patients were first evaluated with baseline noncontrast CT of the head and CTA. CTP was performed at the discretion of the treating physicians. Experienced neurologists performed all NIHSS and mRS assessments. Mechanical thrombectomy was performed with the patient under conscious sedation or general anesthesia by experienced fellowship-trained neurointerventionalists. Patients underwent endovascular treatment if they had an ASPECTS of 6–10, moderate-to-good collaterals on CTA, and an ischemic penumbra of >50% of the total hypoperfused area identified by CTP. Each case was evaluated on the basis of clinical history and radiologic imaging. Informed consent was obtained for mechanical thrombectomy for all patients except those whose legally authorized representatives were not available (2-physician consent was used in those cases). Thrombectomy techniques used included a stent retriever with a balloon guide catheter (BGC), Solumbra, Embotrap pinning catheter (EPIC), and A Direct Aspiration First Pass Technique (ADAPT) as described below (determined by the individual neurointerventionalist). Balloon-guide catheter use varied depending on the interventionalist's preference. There was no limit to the number of passes attempted with the EmboTrap II stent retriever; however, in case of clot-retrieval failure, each interventionalist could independently choose an alternate device for treatment continuation. ADAPT was only used as a rescue technique after failure of the EmboTrap II stent retriever.
ADAPT
In ADAPT, a large-bore aspiration catheter is advanced to the proximal aspect of the thrombus and connected to a source of continuous aspiration, and the thrombus is suctioned.
Stent Retriever with Balloon Guide
In stent retriever with balloon guide, a large-bore BGC is first placed in the cervical ICA. Next, a microcatheter is navigated over a microwire across the clot. A stent retriever is then deployed across the occlusion. During the removal of the stent retriever with thrombus, the balloon guide catheter is inflated to occlude the proximal vessel and achieve proximal flow arrest. The balloon-guide catheter is also placed under suction to achieve flow reversal.
Solumbra
In the Solumbra technique, a guide catheter is first placed in the cervical ICA. Next, a large-bore aspiration catheter is then advanced to the proximal portion of the thrombus over a microcatheter. A stent retriever is then deployed across the occlusion. During removal of the stent retriever into the aspiration catheter, the aspiration catheter is connected to a continuous aspiration source.
EPIC
In EPIC, a large-bore BGC is first placed in the cervical ICA. An aspiration catheter is then advanced to the proximal portion of the thrombus over a microcatheter. A stent retriever is deployed across the occlusion. During removal of the stent retriever and the aspiration catheter as a unit, the balloon-guide catheter is inflated, with negative suction applied to achieve proximal occlusion and flow reversal. The aspiration catheter is simultaneously connected to a continuous source of aspiration during its removal with the stent retriever.
Outcomes
The TICI score was used to evaluate immediate angiographic results, and TICI ≥ 2b was defined as successful reperfusion. The NIHSS score was assessed after the procedure, at hospital discharge, and at 90 days after the procedure. MR spectroscopy was assessed at hospital discharge and 90 days after the procedure. Both evaluations were performed by experienced neurologists not involved in the procedure. Device-related complications, procedural complications, and instances of hemorrhagic conversion were recorded. Mean and [SD] were used to express continuous variables, while categoric variables were described through frequency distributions. All data analysis was conducted using STATA, Version 15.1 (StataCorp).
RESULTS
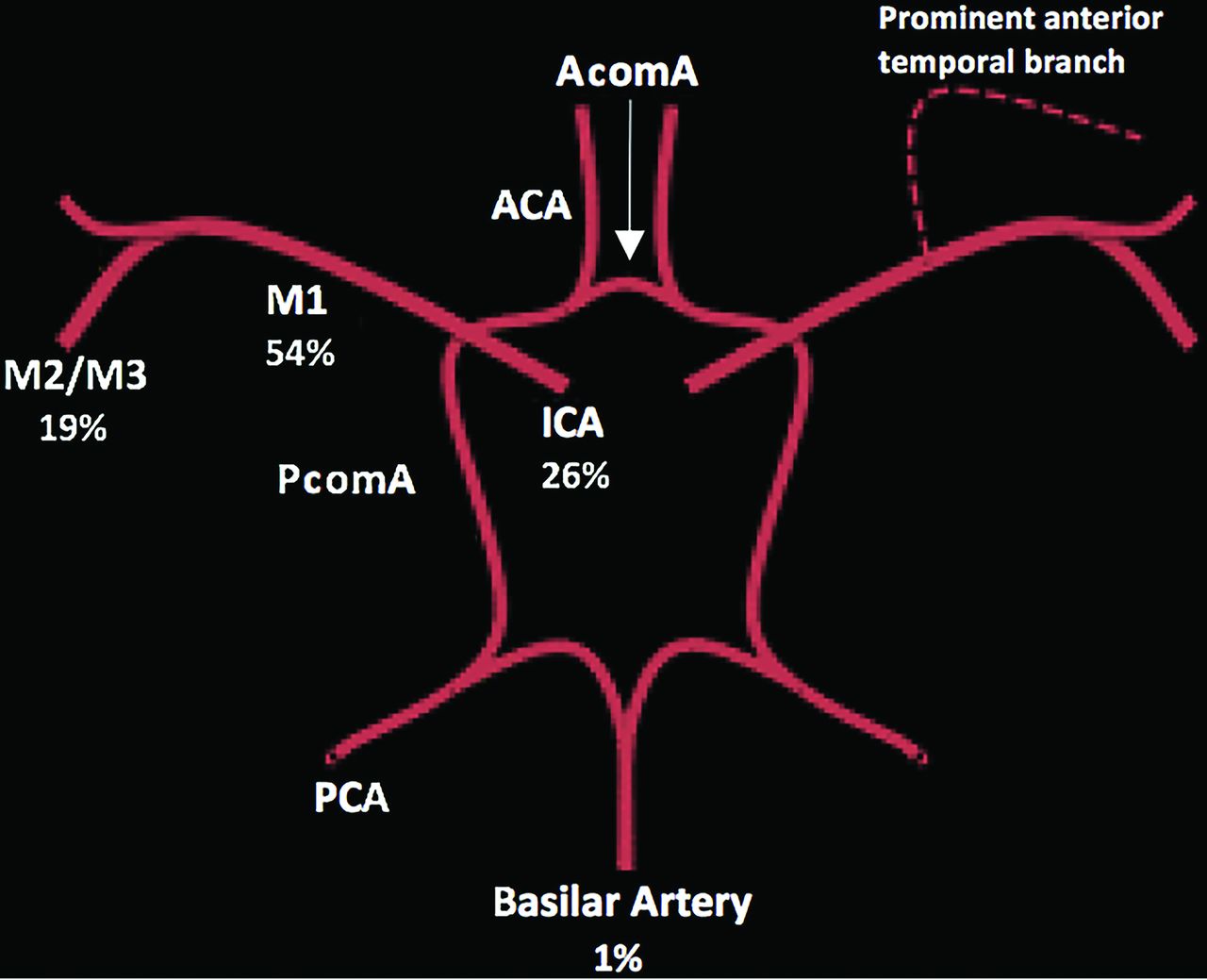
A total of 70 patients were treated with the EmboTrap II device, with a mean age of 69.9 years; 48.6% of patients were women. Hypertension was the most common comorbidity (80.3%), followed by atrial fibrillation, hyperlipidemia, diabetes, and prior strokes. The mean preoperative NIHSS score on admission was 16.3 [SD, 6.6] (range, 3–27), the mean preoperative baseline mRS score was 0.4 [SD, 0.9] (range, 0–4), and 94.0% of patients had mRS ≤ 2 at admission. All except 1 case (basilar artery occlusion) were in the anterior circulation, with most occlusions in M1 (54.3%), followed by the ICA (25.7%), M2 (15.7%), and M3 (2.9%) as shown in Fig 2. There were 3 tandem occlusions, and one of the ICA occlusions was in the petrocavernous segment. Intravenous thrombolysis was administered in 34.3% of cases. Baseline patient characteristics are detailed in Table 1.

Distribution of sites of vessel occlusion treated. Most occlusions were in M1 (54.3%), followed by the ICA (25.7%), followed by M2 (15.7%) and M3 (2.9%). AcomA indicates anterior communicating artery; PcomA, posterior communicating artery; PCA, posterior cerebral artery; ACA, anterior cerebral artery.
Baseline characteristics and demographics
Most patients had conscious sedation (63.2%), while 36.8% underwent general anesthesia. Last-known healthy (LKN) to puncture time was 444.7 [SD, 310.4] minutes, and the mean procedure time (puncture to reperfusion) was 54.2 [SD, 36.0] minutes. The 5 × 33 mm device was used in 88% of cases, while the 5 × 21 mm device was used in the other 12%. A mean of 2.5 [SD, 1.8] (range, 1–7) passes was made per treatment, including non-EmboTrap II attempts, and a mean of 2.2 [SD, 1.6] (range, 1–7) passes was made per treatment when the EmboTrap II was the definitive treatment. Definitive treatment with an alternative device (aspiration, another stent retriever, intra-arterial tPA, and stent placement) was required in 12.9% of cases. Procedural variables are detailed in Table 2. A balloon-guide catheter was used in 38.6% of cases. As overviewed in Table 3, TICI ≥ 2b recanalization was achieved in 95.7% of patients. TICI ≥ 2b recanalization was achieved in 82.3% of patients for whom the EmboTrap II was used as the definitive device. First-pass efficacy (FPE), defined as TICI ≥ 2b recanalization after a first pass with the device, was achieved in 35.7% of patients.
Procedural variables
Clinical and radiographic outcomes
The NIHSS score improved from a preoperative mean of 16.3 [SD, 6.6] to 12.1 [SD, 7.6] postprocedure, and to 10.5 [SD, 11.2] at discharge (deceased patients were given an NIHSS score of 42). The mean mRS at discharge was 3.2 [SD, 1.7] (range, 0–6), with 43.1% of patients having mRS ≤ 2, and the mean mRS at 90 days was 2.7 [SD, 2.2] (range, 0–6), with 52.9% of patients having mRS ≤ 2. Embolization to distal or a new territory was found in 15.7% of patients, and hemorrhagic conversion of any type was noted in 22.9% of cases, of which 4.3% were symptomatic (Table 4). Mortality at 90 days was 11.4%. There were no device-related complications.
Adverse events
Sample Case
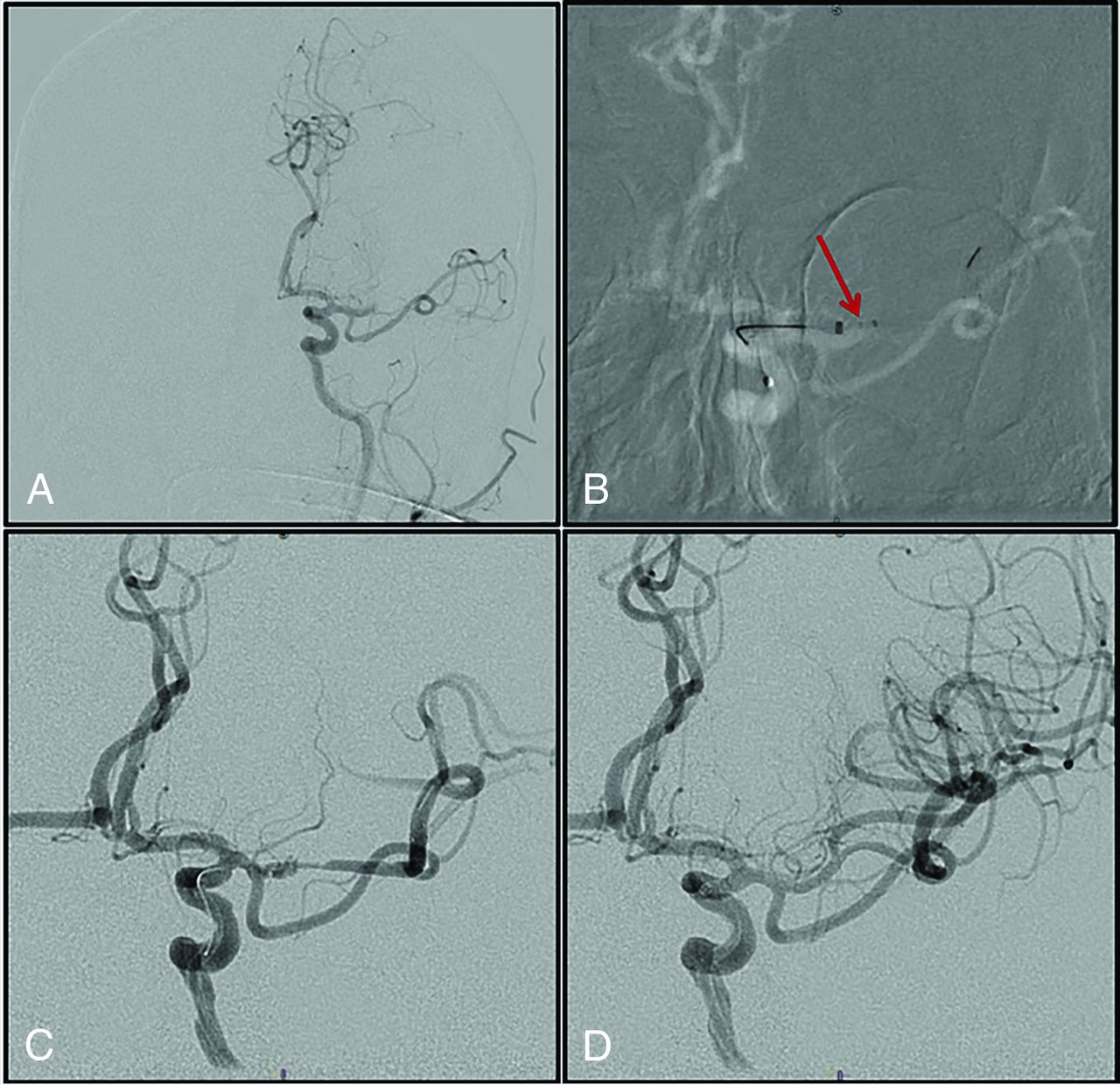
A 72-year-old man with a history of diabetes, hypertension, and hyperlipidemia presented with acute onset of expressive aphasia and right-sided weakness. His LKN was at 9:30 pm before he went to bed, and at 2:30 am, the patient was found on the floor of the restroom, unable to talk and with weakness in his right upper extremity. On initial examination, the patient had an NIHSS score of 17. CTA and angiography showed left M2 occlusion (Fig 3). Mechanical thrombectomy was performed with a 5 × 33 EmboTrap II and a distal-access catheter using the Solumbra technique. TICI 3 revascularization was achieved after a single pass. On postoperative day 1, the patient was found to have marked improvement on examination with an NIHSS score of 2. The patient was discharged home on postoperative day 5.

Angiographic runs of a patient case. A, Preoperative angiogram shows M2 occlusion. B, EmboTrap II deployed across the occlusion. C, Angiogram run after EmboTrap II deployment. D, Angiographic run after EmboTrap II removal.
DISCUSSION
The results of our study support the safety and efficacy of EmboTrap II, and its procedural success and safety metrics are comparable with those of other commercially available stent retrievers. Table 5 presents a comparison of our study with that of Valente et al,9 ARISE II,8 Solitaire With the Intention for Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME),4 and Thrombectomy Revascularization of Large Vessel Occlusions in Acute Ischemic Stroke (TREVO 2).10 Valente et al studied EmboTrap II, ARISE II studied the first-generation EmboTrap device, and SWIFT PRIME and TREVO 2 studied the Solitaire and Trevo stent retrievers, respectively, the 2 most commonly used stent retrievers in the United States. Overall, the final reperfusion rate in EmboTrap II–only cases in our study was 82%, similar to the results in Valente et al. Most interesting, although our FPE was similar to that of Valente et al (36% versus 34%), both our study and Valente et al's had a lower FPE than was reported in ARISE II (52%), in which the original EmboTrap device was used. This finding suggests that the original design may have a higher FPE, especially because the use of the BGC was similar between ARISE II and Valente et al. The rate of good functional outcome (mRS 0–2) at 90 days in this study was similar to that of Valente et al (53% versus 55%), but both our study and that of Valente et al's had worse outcome than reported in ARISE II (67%). This finding may be related to our lower FPE. In addition, ARISE II evaluated only patients treated within 8 hours, whereas our real-world study had many cases beyond the ones with a mean time from LKW to puncture of 7.4 [SD, 5.2] hours. This finding may also explain the slightly worsened results in our study.
Comparison with prior studies
The mean procedure time in our study (54.2 minutes) is on the longer side; however, it is likely related to the difficulty of the cases rather than an inherent problem with the stent retriever. Our rate of symptomatic intracerebral hemorrhage (sICH) was similar to that of ARISE II, lower than that of TREVO 2, and higher than that of Valente et al and SWIFT PRIME, which both reported no sICH.
Of note, our rate of distal embolization (15.7%) was higher than that of the other studies. Valente et al9 also studied the EmboTrap II device and reported no cases with distal embolization. The mechanical design of the EmboTrap stent retriever with the distal mesh has been shown to reduce distal embolization, thus making our results surprising,11 especially in comparison with the results of Valente et al. A study by Chueh et al12 examined distal embolization and found that BGC use during thrombectomy led to a lower rate of distal embolization. Our rate of BGC use (39%) is substantially lower than that of Valente et al and ARISE II (79% and 74%). Furthermore, our mean number of passes when EmboTrap II was used as the definitive treatment was slightly higher than that of Valente et al. These 2 reasons in combination could potentially explain the high rate of distal embolization in our study.
With the addition of our multicenter study to the prior single-center series of 29 patients of Valente et al,9 we bring the total number of EmboTrap II cases in the literature to 99. Combining both datasets yields the following cumulative literature rates for EmboTrap II: final reperfusion rate (80%), FPE (35%), sICH (3%), 90-day mRS ≤2 (54%), mean procedure time (55.6 minutes), and distal embolization (11%). These results are comparable with those in studies of other stent retrievers depicted in Table 5.
Limitations
Our study has several limitations. First, as a multicenter series, there were variations in thrombectomy techniques among different interventionalists, which could affect the results. Second, our study was a single-arm study with no comparison group, making a definitive comparison with other stent retrievers difficult. Third, the results of our study may have low generalizability because most emergent large-vessel occlusions were treated with alternative devices per center (Online Supplemental Data). Fourth, the angiographic results were self-adjudicated, and the analysis was performed in a retrospective manner, thus introducing bias. In contrast, the clinical follow-up was performed by experienced neurologists unrelated to the study. Last, 90-day follow-up mRS data were limited and were only available in 49% of patients.
CONCLUSIONS
We present the first prospective multicenter experience with the novel EmboTrap II stent retriever. The procedural efficacy and safety profile of the device in our study are favorable and comparable with those of other commercially available stent retrievers. Compared with EmboTrap II, the first generation EmboTrap may have a higher FPE, but this possibility needs to be further examined in future studies comparing the 2 devices. Data on this new device are still limited by retrospective case analysis, incomplete clinical follow-up, and low sample size, necessitating further future trials.
Footnotes
Disclosures: Robert M. Starke—UNRELATED: Consultancy: Medtronic, Penumbra, Cerenovus, Abbott Laboratories Ineurico; Grants/Grants Pending: National Institutes of Health, Bee, Braf, Joe Niekro, Poseydon, and The Aneurysm and AVM Foundation*. Ameer E. Hassan—RELATED: Consulting Fee or Honorarium: Medtronic, Stryker, MicroVention, Cerenovus, Penumbra, Genentech, Balt, Viz.ai, Scientia Vascular, GE Healthcare, Comments: consulting; Support for Travel to Meetings for the Study or Other Purposes: Medtronic, Stryker, MicroVention, Cerenovus, Penumbra, Genentech, Viz.ai, GE Healthcare; Fees for Participation in Review Activities such as Data Monitoring Boards, Statistical Analysis, Endpoint Committees, and the Like: Medtronic, Penumbra; UNRELATED: Patents (Planned, Pending or Issued): I have device patents that are not part of this work. Peter Kan—UNRELATED: Consultancy: Consultant for Cerenovus. Reade A. de Leacy—UNRELATED: Consultancy: Cerenovus, Comments: Scientific Advisory Board member. Dileep R. Yavagal—RELATED: Grant: Cerenovus, Comments: Cerenovus funded the EXCELLENCE registry and my institution, University of Miami, was a site for the EXCELLENCE registers*; Consulting Fee or Honorarium: I am a consultant to Cerenovus. I have not had any projects or payments from Cerenovus in the last 18 months; UNRELATED: Consultancy: Medtronic, Cerenovus, Rapid Medical, Neural Analytics, Poseydon; Stock/Stock Options: Rapid medical and Poseydon. None issued to date; OTHER RELATIONSHIPS: Global Chair of Mission Thrombectomy 2020+, a nonprofit public health campaign and alliance. This is a campaign run by the Society of Vascular and Interventional Neurology l, a nonprofit medical society. Alejandro M. Spiotta—UNRELATED: Consultancy: Penumbra, Stryker, Terumo, Siemens, Cerenovus; Grants/Grants Pending: Penumbra, Stryker, Medtronic.* *Money paid to the institution.
Paper previously presented at: Annual Meeting of the Congress of Neurological Surgeons, October 19–23, 2019; San Francisco, California.
References
- Received August 21, 2020.
- Accepted after revision November 23, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}