
Abstract
BACKGROUND AND PURPOSE: Ischemic stroke is the leading cause of long-term disability in adults, but our ability to prognosticate from baseline imaging data is limited. The ASPECTS measures ischemic change in the middle cerebral artery territory on noncontrast CT based on 10 anatomic regions. Here, we investigated whether infarction in particular regions was associated with worse long-term outcome.
MATERIALS AND METHODS: We identified consecutive patients receiving mechanical thrombectomy for ICA/MCA occlusion at 2 comprehensive stroke centers. Pretreatment ASPECTS was assessed by 2 blinded reviewers. Clinical data including demographics, baseline NIHSS score, and 90-day mRS were collected. The relationship between individual ASPECTS regions and the mRS score (0–2 versus 3–6) was assessed using multivariable logistic regression.
RESULTS: Three hundred fifty-three patients were included (mean age, 70 years; 46% men), of whom 214 had poor outcome (mRS = 3–6). Caudate (OR = 3.26; 95% CI, 1.33–8.82), M4 region (OR = 2.94; 95% CI, 1.09–9.46), and insula (OR = 1.75; 95% CI, 1.08–2.85) infarcts were associated with significantly greater odds of poor outcome, whereas M1 region infarction reduced the odds of poor outcome (OR = 0.38; 95% CI, 0.14–0.99). This finding remained unchanged when restricted to only patients with good recanalization. No significant associations were found by laterality. Similarly, no region was predictive of neurologic improvement during the first 24 hours or of symptomatic intracerebral hemorrhage.
CONCLUSIONS: Our results indicate that ASPECTS regions are not equal in their contribution to functional outcome. This finding suggests that patient selection based on total ASPECTS alone might be insufficient, and infarct topography should be considered when deciding eligibility for thrombectomy.
ABBREVIATION:
- sICH
- symptomatic intracranial hemorrhage
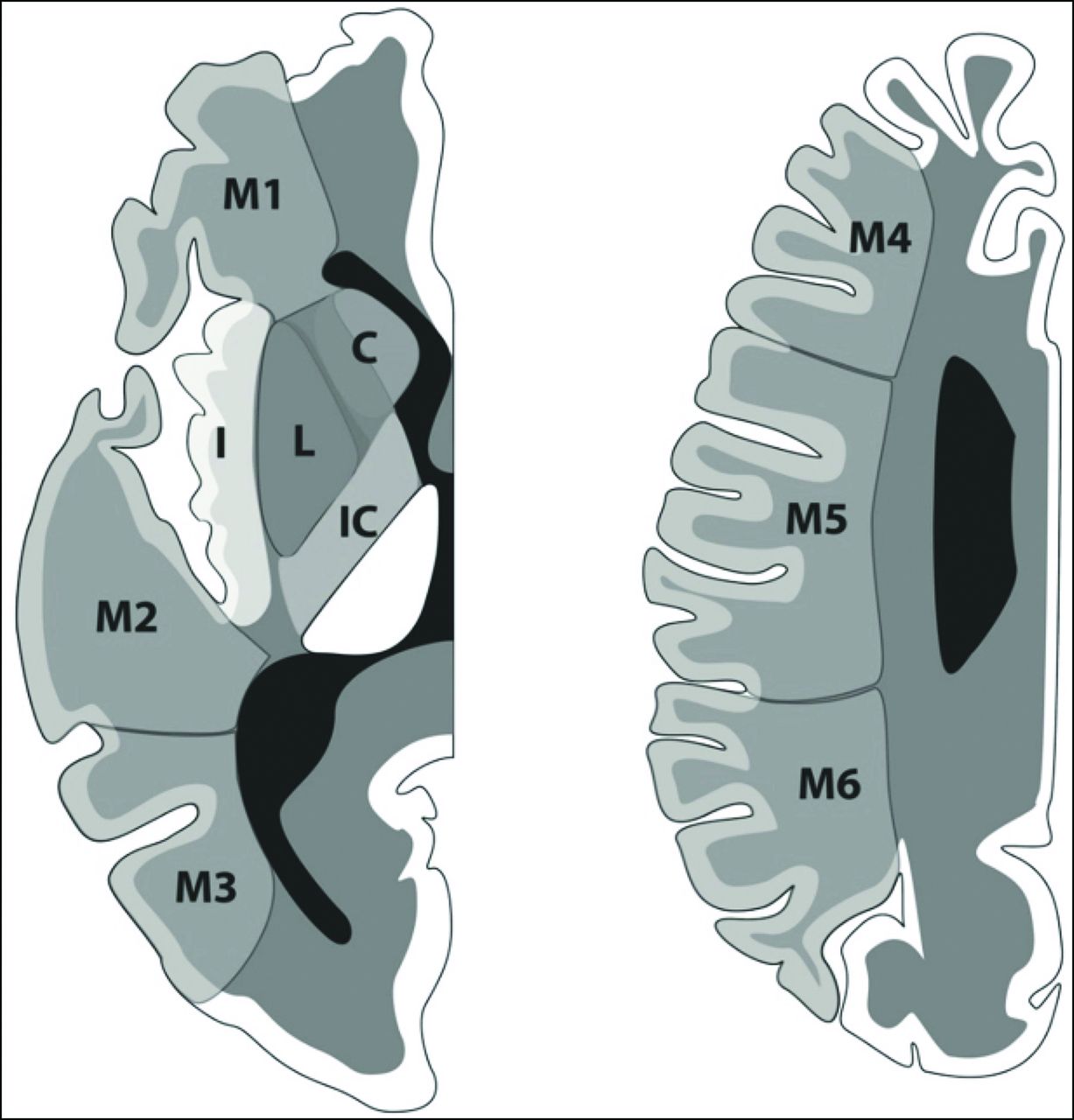
Recent advances in the field of endovascular thrombectomy have led to a sea change in the management of large-vessel-occlusion acute ischemic stroke, with several initial trials showing benefit with new-generation endovascular approaches.1⇓⇓⇓⇓-6 The time window for thrombectomy has subsequently expanded to up to 24 hours from onset.7,8 In all these trials, imaging was crucial to identify patients likely to benefit. Most trials in 2015 used lesion size on CT as part of their selection criteria, quantified as the ASPECTS. ASPECTS was first described in 2000 and separates the middle cerebral artery territory into 10 regions (6 superficial, 4 deep; Figure). These are then assigned a value of 0 if there are early ischemic changes—parenchymal hypoattenuation, loss of gray-white differentiation, and focal swelling—and a value of 2 if the region is normal in appearance.9 Correspondingly, lower scores imply more extensive ischemia and intuitively suggest that the outcome is more likely to be poor; indeed, the ASPECTS is known to have value in long-term prognostication after stroke,10 and has previously been shown to correlate with functional independence in intra-arterial thrombolysis.11 Thus, low ASPECTS values continue to be used as an exclusion criterion for thrombectomy because these patients are assumed to have a low likelihood of meaningful improvement.

Illustration of ASPECTS, showing 10 regions in 1 hemisphere. C indicates caudate; IC, internal capsule; L, lentiform; I, insula. Reproduced from Neuhaus et al25 with permission from BMJ Publishing Group Ltd.
However, there are a number of disadvantages in using ASPECTS. First, although it significantly correlates with long-term function on a group level, individual outcomes are discriminated less accurately, particularly when the ASPECTS is moderate to high (eg, 6–10, implying limited ischemic change).12 Second, it is known that involvement of specific regions leads to particular functional deficits, eg, the angular gyrus in language13 and multiple cortical and subcortical areas in motor function.14 The ASPECTS treats all 10 areas equally; therefore, a composite ASPECTS of 7 may reflect very different lesion patterns, and there is no a priori reason to think these would be equivalent in terms of functional consequences. Third, the volumes of ASPECTS regions are not equal, and the loss of a single point can reflect a wide range of ischemic volumes, depending on which areas are affected. Indeed, it has been previously reported that some regions confer a greater risk of poor long-term outcome.15 Variation in outcome based on the affected area has also been described with ASPECTS regions from baseline CT,15⇓⇓-18 though with inconsistent findings.
The implication of this finding is that a significant number of patients with a poor composite ASPECTS might, in fact, have a greater likelihood of good outcome than the total score would suggest, which may influence treatment decisions. In this study, we sought to estimate regional contributions to long-term function using pretreatment ASPECTS data in a thrombectomy cohort.
MATERIALS AND METHODS
Study Subjects
We conducted a retrospective analysis of 353 consecutively treated patients with a diagnosis of acute ischemic stroke related to an emergent large-vessel occlusion from January 2015 to December 2018. One hundred seventy-eight patients were treated at the first participating center, and 175 patients, at the second (Mayo Clinic and Toronto Western Hospital). ASPECTS ≥6 was a prerequisite for proceeding with thrombectomy at our institutions.
The inclusion criteria were as follows:
Clinical diagnosis of acute stroke in the anterior circulation
Eighteen years of age or older
Availability of NCCT images acquired within 24 hours of onset of symptoms
Patients with intracranial ICA, M1, or M2 occlusion identified on CTA who were treated by endovascular thrombectomy.
Among the exclusion criteria were nonischemic pathology found on baseline imaging (eg, intracerebral hemorrhage), poor quality of baseline scans (eg, excessive artifacts preventing regional ASPECTS estimation), and denial of consent following checking for research authorization.
Baseline clinical characteristics collected from subjects included age, sex, NIHSS score, and time of last known well; posttreatment characteristics included the mRS score at 90 days and recanalization status after thrombectomy. The study was approved by the institutional review boards at both institutions; because this was a retrospective study, informed consent was waived. However, per Minnesota state law, after checking the status of all patients residing in the state of Minnesota, 21 patients who denied access to their medical records for research use were not included in this study.
CT Acquisition and Analysis
Noncontrast CT scans with 5-mm section thickness were obtained at admission, with a maximal delay of <24 hours from stroke onset. ASPECTS was independently determined by 2 neuroradiologists at each site, for a total of 4 raters who were blinded to clinical outcome. In case of any disagreement, a third neuroradiologist in each center reviewed and adjudicated the score. 9,19 In contrast to the original methodology of using 1 supraganglionic and 1 ganglionic section for ASPECTS, assessors had access to the entire NCCT scan. Evidence of early ischemic change was defined as the presence of hypoattenuation and/or loss of gray matter–white matter differentiation, with or without cortical swelling. Assessors were aware of the presumed laterality of the stroke but blinded to other clinical details.
Statistical Analysis
A summary of clinical and imaging characteristics is presented in the Online Supplemental Data as mean (SD) (age, NIHSS) or median with interquartile range (ASPECTS). The relationship between individual ASPECTS regions and the ordinal functional outcome score (mRS) was assessed using multivariable logistic regression. mRS was dichotomized as good (0–2) or poor (3–6). Ten-fold cross-validation was then used to estimate the predictive value of each region, and a multivariable logistic regression with the 10 regions in a single model was fitted. This was also used for subgroup analyses based on laterality (left and right hemispheres separately) and recanalization status based on angiographic findings (dichotomized as TICI 2b/3 for successful recanalization and also examining TICI 3 separately). We also explored the predictive value of regional ASPECTS for symptomatic intracranial hemorrhage following thrombectomy and for NIHSS change within the first day following stroke onset (calculated simply as NIHSS24 hours – NIHSSbaseline) as an indicator of acute neurologic deterioration or improvement. Data were collected in Excel (Microsoft) and analyzed using R statistical and computing software (http://www.r-project.org/).
RESULTS
Baseline Characteristics
The baseline characteristics of the patient population are presented in the Online Supplemental Data. The mean age of patients was 70 years, and 46% were men. Baseline imaging showed a median total ASPECTS of 9; early ischemic changes were most commonly seen in the insula (172 patients, 48.7%) and lentiform nucleus (96 patients, 27.2%) and least frequently in M6 (16 patients, 4.5%).
Primary Outcome
Logistic regression for regional ASPECTS irrespective of laterality (Table 1) showed that the regions significantly associated with poor outcome were the caudate nucleus (ORcaudate = 3.26; 95% CI, 1.33–8.82), M4 (ORM4 = 2.94; 95% CI, 1.09–9.46), and insula (ORinsula = 1.75; 95% CI, 1.08–2.85). Conversely, M1 was associated with reduced odds of poor outcome (ORM1 = 0.38; 95% CI, 0.14–0.99). The remaining 6 areas (M2, M3, M5, M6, lentiform nucleus, and internal capsule) did not reach statistical significance. When we separated them by the side of the stroke, no regions reached statistical significance, though similar trends were observed; on the right, there was an additional trend for M6 in particular (ORM6 = 3.71; 95% CI, 0.72–29.4) and on the left for M5 (ORM5 = 2.80; 95% CI, 0.81–13.2).
Predictive value of ASPECTS regions for mRS at 90 days
Subgroup Analyses
The average total ASPECTS for patients without insular or caudate infarcts was higher than for those with insula or caudate involvement (P value < .0001) (Table 2).
Comparison of total ASPECTS between patients with caudate or insular infarct with the rest of cohort
Of the studied population, 302 (85.6%) had successful recanalization, defined as TICI 2b/3. When this cohort was analyzed as a subgroup, the results were effectively unchanged from the total population (Table 3), with the caudate nucleus (ORcaudate = 4.02; 95% CI, 1.51–12.2), M4 (ORM4 = 3.54; 95% CI, 1.26–11.9), and insula (ORinsula = 1.69; 95% CI, 1.01–2.85) being associated with poor outcome; again, M1 infarction was associated with lower odds of poor outcome (ORM1 = 0.28; 95% CI, 0.09–0.83). When this cohort was restricted to only TICI 3 (n = 154), suggesting complete reperfusion, only the caudate nucleus (ORcaudate = 14.86; 95% CI, 3.22–114.94) reached statistical significance. The group of patients with unsuccessful recanalization (TICI 0/1/2a, n = 51) was too small to reliably estimate ORs.
Predictive value of ASPECTS regions for mRS at 90 days, stratified by recanalization status
ASPECTS Regions and Short-Term Outcomes
We then repeated the analyses using symptomatic intracranial hemorrhage (sICH) as an outcome. In our sample, 27 patients (7.6%) developed sICH within the first 24 hours following thrombectomy. Due to the small sample size, there was no significant association with any ASPECTS region; because the lowest P value was .299, it was not possible to characterize any trends in the data (Table 4). We also used changes in the NIHSS score during the first 24 hours as the outcome metric to explore the impact of individual regions on short-term neurologic improvement. No individual ASPECTS region showed significant correlation with NIHSS change (Online Supplemental Data), with a slight trend toward the lentiform nucleus (ORlentiform = 6.89; 95% CI, 0.57–83.10).
Predictive value of ASPECTS regions for sICH
DISCUSSION
In this study, we have characterized the long-term functional impact of ischemia in specific regions of the ASPECTS system in patients who underwent thrombectomy after baseline imaging. Our main finding is that infarction in the caudate, M4, and insula areas is significantly associated with poor outcome (mRS = 3–6) following thrombectomy, whereas patients with M1 infarctions have reduced odds of poor outcome. The same observation was made when analyses were restricted to only those patients in whom good recanalization was achieved. Analyses by laterality or looking at neurologic improvement and sICH as outcomes did not reach statistical significance. The implication of these results may be that the use of a composite ASPECTS should be re-evaluated because the total score may be less informative than individual territories, as discussed below.
Previous studies have examined the contribution of individual ASPECTS regions to outcome. However, the results reported in the literature show significant disagreement. For example, Khan et al18 reported that M3 and M6 infarction on either side, M2 on the right, and M5 on the left were associated with poor outcome. Beare et al17 also reported M2 and M5 infarction as a poor prognostic factor, without specifying side. In the largest study looking at admission NCCT, Payabvash et al20 found M5, caudate, lentiform, and insula infarction to be associated with poor outcome in patients treated with intravenous thrombolysis. Phan et al16 only found significant results from interaction terms between age and lentiform, and age and M6. There have also been studies using the ASPECTS template with modalities other than NCCT. Haranhalli et al21 found that insula, M2, and M5 infarcts on CT perfusion were associated with poor outcome. Payabvash et al15 also reported that insula infarction predicted poor outcome, using DWI at admission.
One important difference with the results reported here is the clinical care provided to the patient population. Most patients in the aforementioned studies were either managed conservatively or treated with intravenous thrombolysis. Payabvash et al15,20 and Haranhalli et al21 did include patients with subsequent intra-arterial therapy, but given that data collection occurred before 2015, these likely represented intra-arterial thrombolysis and thrombectomy with first-generation devices, which were notably less effective. In contrast, our study included only patients who underwent stent retriever or aspiration thrombectomy and is, therefore, more reflective of the current criterion standard approach to management of large-vessel-occlusion stroke.
We can only speculate on why the regions identified by our study were associated with worse outcomes. M4 represents the frontal cortex on the supraganglionic section, whereas M1 is more the caudal frontal cortex. In terms of function, infarcts involving M1 might lead to deficits in behavioral planning due to involvement of the operculum and may also lead to nonfluent aphasia if the dominant hemisphere (ie, left in most individuals) is affected. Hemiplegia, in particular, might be expected to have a substantial effect on mRS because the scale is largely based on mobility. M4 might similarly be associated with aphasia and apraxia on the dominant side, though limb weakness is less likely. Similarly, the caudate nucleus is part of the basal ganglia and crucial for motor control, as well as being associated with cognitive changes. The insula is primarily associated with autonomic function, but also with motor control, cognition, and emotion.22,23
Limitations
There are limitations to this study. First, although our total cohort was relatively large, subgroup analyses for sICH, stroke laterality, and outcome in poorly recanalized patients were limited by small sample sizes. In addition, we had relatively few cases with stroke in some of the cortical areas (most notably M6) and the internal capsule. This spectrum bias is probably the consequence of selection bias for endovascular thrombectomy. Second, the median ASPECTS in this study was 9, suggesting only limited ischemic changes. Although this was also the median ASPECTS value in the meta-analysis of the 2015 trials1 and is therefore representative of patients receiving endovascular thrombectomy, it, nonetheless, complicates applying these findings to patients with more extensive ischemic changes and lower total ASPECTS. Third, our analyses currently assume that regional ischemic changes were independent of each other, and we have not adjusted for collinearity; however, preliminary analyses did not show significant collinearity in our dataset. Although in our cohort, patients with infarcts in the insula or caudate nucleus had poorer total ASPECTS, this still warrants further follow-up studies. Fourth, there is potential interobserver variability, as was reported by Nicholson et al24 in their study of 375 patients with acute ischemic stroke, which showed substantial interobserver variability among readers in scoring different ASPECTS regions. They found that readers had the highest agreement in scoring the insula (κ = 0.56; range, 0.48–0.64) and the lowest agreement in scoring M3 (κ = 0.34; range, 0.12–0.56).
CONCLUSIONS
We have characterized outcome based on regional infarction as determined by the ASPECTS template on baseline NCCT. This work is hypothesis-generating and may be of potential use in the development of scoring systems that take infarct topography into account and allow improved patient-selection algorithms for thrombectomy. Therefore, larger datasets are required to validate our findings and provide more definitive quantification of the impact of ischemia in different ASPECTS areas on outcome.
Footnotes
W. Brinjikji and J.D. Schaafsma contributed equally as senior and supervising authors.
This work was supported by an Award from the American Heart Association (19POST34381067) to S.M. Seyedsaadat. A.A. Neuhaus was supported by an award from the Oxford University Clinical Academic Graduate School.
Disclosures: Seyed Mohammad Seyedsaadat—RELATED: Grant: American Heart Association, Comments: 2 years postdoctoral fellowship American Heart Association research grant. Timo Krings—UNRELATED: Consultancy: Stryker, Medtronic, Penumbra; Royalties: Thieme; Stock/Stock Options: Marblehead Medical LLC. Ain A. Neuhaus—RELATED: Grant: Oxford University Clinical Academic Graduate School, Comments: internal grant from the Oxford University Clinical Academic Graduate School to support travel and living expenses for medical elective at the Mayo Clinic. David F. Kallmes—UNRELATED: Stock/Stock Options: Superior Medical Experts LLC, Marblehead Medical LLC.
References
- Received November 14, 2019.
- Accepted after revision December 17, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- Association between ASPECTS region of infarction and clinical outcome in non-acute large vessel occlusion ischaemic stroke after endovascular recanalisation
- Penumbra salvage in extensive stroke: exploring limits for reperfusion therapy
- Factors associated with unfavorable outcome after anterior circulation stroke despite successful reperfusion and early neurological improvement