
Abstract
BACKGROUND AND PURPOSE: Accurate assessment of thyroid cartilage invasion on preoperative imaging influences management in patients with laryngeal and hypopharyngeal cancers. We evaluated the clinical usefulness of contrast-enhanced 3D T1-weighted radial gradient recalled-echo for preoperative assessment of thyroid cartilage invasion in patients with laryngohypopharyngeal squamous cell carcinoma, compared with 2D spin-echo T1WI.
MATERIALS AND METHODS: Preoperative MR images of 52 consecutive patients who were diagnosed with laryngeal or hypopharyngeal cancer and underwent partial or total laryngectomy were analyzed. Pathologic specimens served as reference standards. Two independent head and neck radiologists evaluated the presence of thyroid cartilage invasion in both contrast-enhanced 2D spin-echo T1WI and 3D gradient recalled-echo sequences. The sensitivity, specificity, and accuracy of the 2 modalities were compared. The area under the curve was a measure of diagnostic performance.
RESULTS: Pathologic neoplastic thyroid cartilage invasion was identified in 24 (46.2%) of the 52 patients. The sensitivity (75.0%), specificity (96.4%), and accuracy (86.5%) of contrast-enhanced 3D gradient recalled-echo were significantly higher than those of 2D spin-echo T1WI (58.3%, 89.3%, and 75.0%; P = .017, .003, and .002, respectively). 3D gradient recalled-echo had significantly better diagnostic performance (area under the curve = 0.963) than 2D spin-echo T1WI (area under the curve = 0.862; P = .010).
CONCLUSIONS: Contrast-enhanced 3D gradient recalled-echo was diagnostically superior in identifying neoplastic thyroid cartilage invasion compared with 2D spin-echo T1WI in patients with laryngohypopharyngeal cancer, and therefore, may provide more accurate preoperative staging.
ABBREVIATIONS:
- AUC
- area under the curve
- GRE
- gradient recalled-echo
- SE
- spin-echo
- THRIVE
- T1-weighted high-resolution isotropic volume examination
Accurate preoperative staging is crucial for deciding appropriate treatment strategies and predicting prognosis in patients with head and neck cancers. Specifically, in laryngeal and hypopharyngeal cancers, treatment strategies vary with the presence of thyroid cartilage invasion.1 If the tumor is localized without extension to the thyroid cartilage, larynx-preserving treatment can be performed. On the contrary, if the tumor extends through the thyroid cartilage, more invasive treatment such as total laryngectomy is considered.2⇓⇓⇓⇓-7 Thus, accurate assessment of thyroid cartilage invasion preoperatively is highly desirable in patients with laryngeal and hypopharyngeal cancers.
MR imaging has been shown to be superior to CT in the assessment of cartilage invasion because of its excellent soft-tissue contrast.8⇓-10 Becker et al9 proposed new diagnostic criteria based on MR imaging to improve the distinction between tumor tissue and peritumoral inflammation involving the laryngeal cartilage in patients with laryngeal and hypopharyngeal cancers. Although MR imaging in head and neck cancer is most widely performed with a conventional 2D spin-echo (SE) sequence, 3D volumetric imaging has emerged as an alternative because it allows isotropic data acquisition with multiplanar image reconstruction, within an acceptable acquisition time. In addition, T1-weighted high-resolution isotropic volume examination (THRIVE), a 3D ultrafast spoiled gradient MR imaging sequence that incorporates a frequency-selective fat-saturation pulse, was recently shown to be clinically superior for preoperative evaluation of head and neck cancer, providing more accurate measurement of tumor size and higher sensitivity to detect the primary tumor in patients with cervical lymph node metastases of unknown primary tumors, compared with 2D SE T1WI.11,12
We hypothesized that contrast-enhanced 3D gradient recalled-echo (GRE) might allow more accurate identification of neoplastic thyroid cartilage invasion compared with 2D SE T1WI in patients with laryngohypopharyngeal cancer. The aim of the present study was to investigate the potential of GRE for the preoperative assessment of thyroid cartilage invasion in patients with laryngohypopharyngeal cancer by comparing it with 2D SE T1WI.
MATERIALS AND METHODS
Study Population
This retrospective study was approved by the institutional review board of our institution, Severance hospital, and the requirement for informed consent was waived on the basis of its retrospective nature. Between July 2012 and June 2019, one hundred twenty-four consecutive patients with laryngeal and hypopharyngeal squamous cell carcinoma who underwent partial or total laryngectomy for curative intent at our institution were initially included. Exclusion criteria were as follows: no preoperative MR imaging (n = 8), unavailability of either 2D SE T1WI or 3D GRE scans (n = 20), and patients who underwent neoadjuvant chemotherapy or radiation therapy (n = 44). Therefore, after accounting for the exclusion criteria, a total of 52 patients (48 men and 4 women; mean age, 66.4 years; range, 33–79 years) were included in this study.
MR Imaging Acquisition
All patients underwent MR imaging with a 3T system (Intera Achieva or Achieva TX; Philips Healthcare) and a head and neck coil. Conventional MR imaging consisting of axial SE T1-weighted (TR = 560 ms, TE = 10 ms, matrix = 256 × 256, 4-mm section thickness, 1-mm intersection gap, and 2 signal averages) and fat-saturated axial fast SE T2-weighted imaging (TR = 6480 ms, TE = 70 ms, matrix = 256 × 256, 4-mm section thickness, 1-mm intersection gap, and 2 signal averages) were performed according to the routine protocol for the head and neck, respectively, before injecting the contrast material. All images were obtained with a 22- to 25-cm FOV, which was adjusted for each patient. Subsequently, gadopentetate dimeglumine (Magnevist; Bayer HealthCare Pharmaceuticals) was administered intravenously at a dose of 0.2 mL/kg body weight at a rate of 2 mL/s. Forty seconds after administering the contrast material, fat-saturated axial GRE scans were acquired, followed by fat-saturated axial and coronal 2D SE T1WI scans sequentially. The axial GRE images were then reformatted into the coronal and sagittal planes.
The sequence parameters for the contrast-enhanced 2D SE T1WI were as follows: TR = 400–550 ms, TE = 10 ms , flip angle = 90°, bandwidth = 75.3 Hz/pixel, matrix = 256 × 256, 4-mm section thickness, 1-mm intersection gap, 2 signal averages, and acquisition time = 303 seconds for axial images and 175 seconds for coronal images. The parameters for the contrast-enhanced 3D GRE were as follows: TR = 4.5 ms, TE = 2.2 ms, flip angle = 10°, bandwidth = 434 Hz/pixel, matrix = 256 × 256, 1-mm section thickness, 2 signal averages, and acquisition time = 223 seconds.
Image Analysis
Two experienced head and neck radiologists (with 17 and 3 years of experience, respectively, in head and neck radiology) who were blinded to preoperative clinical findings, patient history, and final pathologic results retrospectively reviewed the MR images of enrolled patients independently. The contrast-enhanced 2D SE T1WI and 3D GRE images were presented to the 2 radiologists in a random fashion, with at least a 2-week interval between the 2 sequences. Each reviewer assessed the presence of thyroid cartilage invasion on the contrast-enhanced 2D SE T1WI and 3D GRE images, using the precontrast SE T1-weighted and fat-saturated fast SE T2-weighted images as references. The presence of thyroid cartilage invasion was determined by comparing the signal intensity of cartilage with that of the adjacent tumor mass visually on fat-saturated SE T2-weighted and contrast-enhanced images, according to MR imaging criteria proposed in 2008.9 If the cartilage presented a signal intensity or enhancement degree similar to that of the adjacent tumor, neoplastic thyroid cartilage invasion was suspected. On the contrary, if the cartilage had a higher signal intensity or stronger enhancement than the adjacent tumor, the cartilage was regarded as having peritumoral inflammation. Subsequently, each reviewer determined the invasion of the thyroid cartilage using the following 4-point scoring system: 1, definitely negative; 2, tumor abutting the thyroid cartilage without invasion (probably negative); 3, tumor invading the inner cortex of the thyroid cartilage and confined to the thyroid cartilage (probably positive); and 4, transmural extralaryngeal spread through the cartilage (definitely positive). Disagreements between the 2 radiologists were resolved by consensus for the final evaluation.
A pathologist with 12 years of experience who was blind to the preoperative imaging findings evaluated the surgical specimens. The final histopathologic results after surgery were used as the reference standard.
Statistical Analysis
The contrast-enhanced 2D SE T1WI and 3D GRE image interpretation results were compared with the histopathologic results. Tumors with scores of ≥3 were considered to have neoplastic thyroid cartilage invasion, to facilitate calculation of the diagnostic performance. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 2D SE and 3D GRE for detecting pathologic thyroid cartilage invasion were calculated with 95% CIs. The McNemar test was performed to compare the sensitivity, specificity, and accuracy between the 2 sequences. Receiver operating characteristic curves were generated to compare the diagnostic performance of the 2 sequences, and the area under the curve (AUC) was calculated. Pair-wise comparisons of the AUCs were performed using the DeLong method. All statistical analyses were performed using R statistical software, Version 3.4.2 (http://www.r-project.org/). P values < .05 indicated a statistically significant difference.
RESULTS
Of the 52 patients, 36 had laryngeal cancer and 16 had hypopharyngeal cancer. Primary tumors were found in the glottis (n = 24), pyriform sinus (n = 12), supraglottis (n = 11), posterior pharyngeal wall (n = 3), subglottis (n = 1), and postcricoid region (n = 1). The final histopathologic examinations after the operation revealed that thyroid cartilage invasion was present in 24 (46.2%) of the 52 patients. Tumor invasion occurred through the outer cortex of thyroid cartilage in 13 patients (54.2%), whereas the tumor invaded only the inner cortex of the thyroid cartilage in the remaining 11 patients (45.8%).
The Online Supplemental Data summarize the diagnostic performances of contrast-enhanced 2D SE T1WI and 3D GRE in assessing the presence of neoplastic thyroid cartilage invasion. In 24 patients with neoplastic thyroid cartilage invasion diagnosed histopathologically, 3D GRE enabled us to identify thyroid cartilage invasion accurately in 18 patients (75.0%), while 2D SE T1WI enabled us to identify the same in 14 patients (58.3%). The sensitivity of 3D GRE was significantly superior to that of 2D SE T1WI (75.0%; 95% CI, 53.3%–90.2%) versus 58.3% (95% CI, 36.6%–77.9%) (P = .017). In 28 patients without neoplastic thyroid cartilage invasion, 3D GRE and 2D SE T1WI enabled us to report the absence of thyroid cartilage invasion accurately in 27 (96.4%) and 25 (89.3%) patients, respectively. The specificity of 3D GRE was significantly superior to that of 2D SE T1WI (96.4%; 95% CI, 81.7%–99.9% versus 89.3%; 95% CI, 71.8%–97.7%) (P = .003). The diagnostic accuracy of 3D GRE (86.5%) was significantly higher than that of 2D SE T1WI (75.0%; P = .002). False-positive and false-negative results were observed in 10 and 3 patients, respectively, on 2D SE T1WI. In contrast, false-positive and false-negative results were observed in 6 and 1 patient, respectively, on 3D GRE. Representative cases for comparison of contrast-enhanced 3D GRE and 2D SE T1WI are shown in Figs 1 and 2.

False-positive findings on a 2D SE T1WI and true-negative findings on a 3D GRE image in a 68-year-old man with supraglottic cancer. Axial fat-saturated fast SE T2WI (A) shows a left-sided laryngeal tumor occupying the paraglottic space and iso-signal intensity of the adjacent left thyroid lamina. Axial precontrast (B) and contrast-enhanced 2D SE T1WIs (C) show similar enhancement of the left thyroid lamina (arrow) compared with the adjacent tumor, regarded as tumor invasion of the thyroid cartilage. Axial contrast-enhanced 3D GRE image (D) shows no definite enhancement of the adjacent left thyroid lamina (arrow), suggesting that the tumor was confined to the paraglottic space without thyroid cartilage invasion. Photomicrograph (E) confirms that tumor cells (arrowheads) do not invade thyroid cartilage (arrows) (hematoxylin-eosin stain; original magnification, ×1.25).

False-negative findings on a 2D SE T1WI and true-positive findings on a 3D GRE image in a 61-year-old man with glottic cancer. Axial fat-saturated fast SE T2WI (A) shows a tumor arising from the right glottis and higher signal intensity of the right thyroid lamina than of the adjacent tumor. Axial precontrast (B) and contrast-enhanced 2D SE T1WIs (C) show strong enhancement of the right thyroid lamina (arrow), regarded as inflammatory changes rather than neoplastic cartilage invasion. Axial contrast-enhanced 3D GRE image (D) shows contrast enhancement of the right thyroid lamina (arrow), similar to that of the adjacent tumor, suggesting neoplastic thyroid cartilage invasion. Photomicrograph (E) confirms that the inner cortex of thyroid cartilage (arrows) is invaded by tumor (arrowheads) (hematoxylin-eosin stain; original magnification, ×1.25).
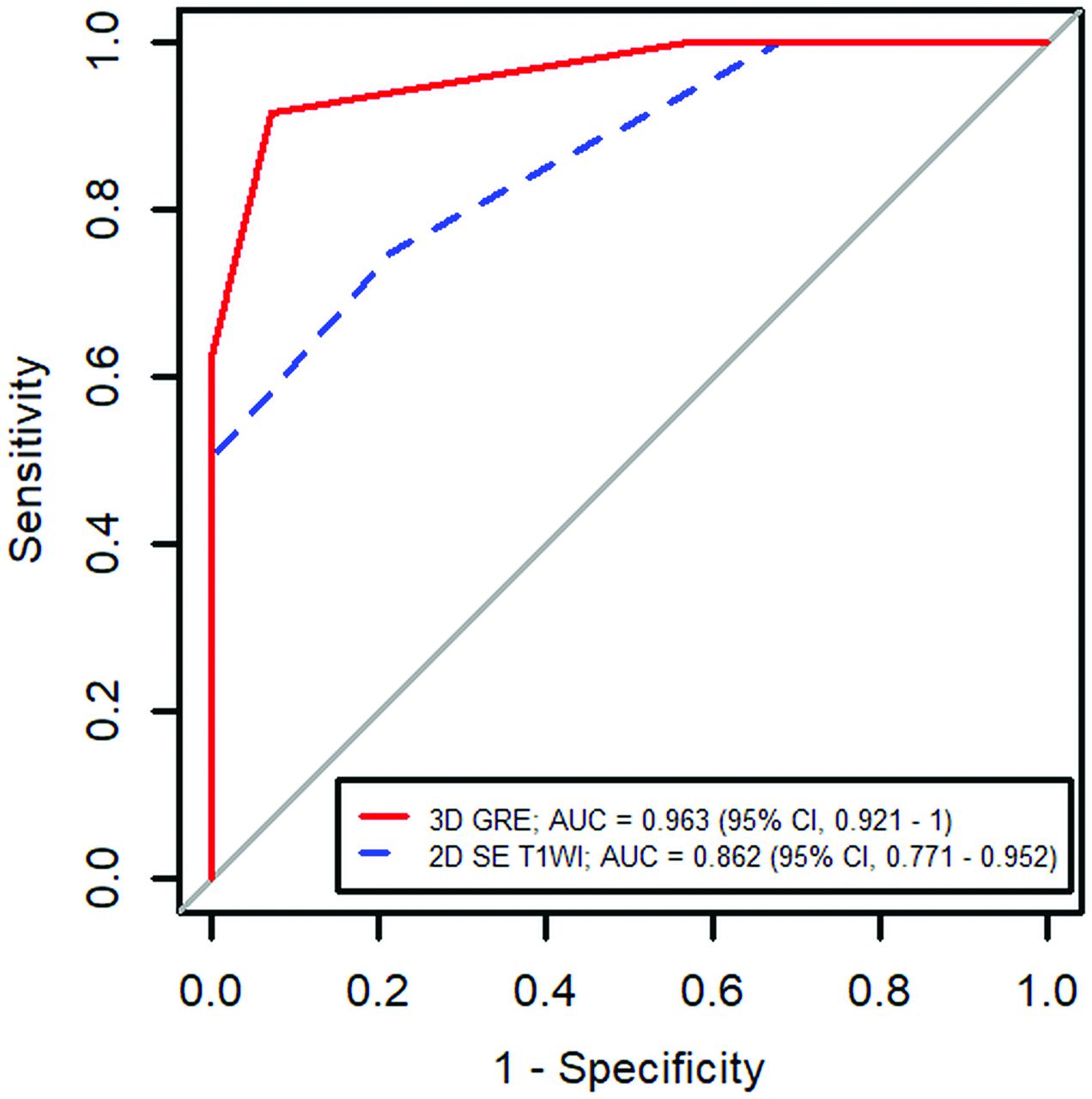
The receiver operating characteristic curve analysis revealed that the diagnostic performance of 3D GRE (AUC = 0.963; 95% CI, 0.921–1.000) was significantly better than that of 2D SE T1WI (AUC = 0.862; 95% CI, 0.771–0.952) (P = .010, Fig 3).

Receiver operating characteristic curve analysis shows the diagnostic performance of 3D GRE and 2D SE T1WI. The AUC was significantly higher with 3D GRE (0.963) than with 2D SE T1WI (0.862, P = .010).
The clinical and pathologic T-stages of the tumors are summarized in the Table. The 36 laryngeal tumors were classified as pT2 (n = 3), pT3 (n = 20), and pT4a (n = 13), and the 16 hypopharyngeal tumors were classified as pT2 (n = 3), pT3 (n = 6), and pT4 (n = 7). Among the 26 patients with pT3, 22 and 25 patients were assessed accurately with cT3 based on 2D SE T1WI and 3D GRE, respectively. Among the 20 patients with pT4, sixteen and 17 patients were assessed accurately with cT4 based on 2D SE T1WI and 3D GRE, respectively.
The clinical and pathologic T-stages of the tumor
DISCUSSION
In this study, contrast-enhanced 3D GRE showed superior sensitivity, specificity, and accuracy than contrast-enhanced 2D SE T1WI in detecting thyroid cartilage invasion in patients with laryngohypopharyngeal cancer. In addition, 3D GRE had better diagnostic performance compared with 2D SE T1WI, suggesting that 3D GRE is an acceptable alternative for 2D SE T1WI for accurate preoperative staging in patients with laryngohypopharyngeal cancer.
Accurate preoperative staging is important to determine an adequate surgical resection margin and appropriate treatment options, which may result in improved prognosis and reduced treatment-associated morbidity in patients with head and neck cancer. Specifically, in patients with laryngohypopharyngeal cancer, the presence of thyroid cartilage invasion by the tumor is one of the key factors that determine treatment strategies, ie, total laryngectomy versus larynx-preserving surgery.13,14 Therefore, several previous studies evaluated the diagnostic performance of various imaging modalities for the detection of neoplastic cartilage invasion. CT is a well-established method, and a few studies have reported that dual-energy CT can provide high specificity and acceptable sensitivity for assessing neoplastic thyroid cartilage invasion in patients with laryngohypopharyngeal cancer.15,16 However, CT cannot distinguish between nonossified cartilage and tumor because they show similar CT values.13,17 In contrast, MR imaging has been regarded as providing higher soft-tissue contrast resolution and superior sensitivity and negative predictive values compared with CT in detecting neoplastic cartilage invasion.9,18 However, MR imaging still has limited value with regard to differentiation of neoplastic cartilage invasion and inflammatory changes because edema or inflammatory changes frequently mimic tumor invasion. In addition, motion artifacts with a relatively long scan time are one of the important issues of MR imaging because patients with head and neck cancer often have breathing and swallowing difficulties.16 Therefore, we attempted to find an optimal contrast-enhanced MR imaging sequence for the assessment of neoplastic thyroid cartilage invasion.
The major advantage of 3D imaging with isotropic data acquisition is that it does not show partial volume averaging artifacts, which are frequently observed on 2D imaging, providing more detailed anatomic information. In addition, there is the potential to reformat images in any plane without compromising image resolution, simplifying imaging protocols and reducing acquisition time when multiplanar imaging is required.19⇓-21 Furthermore, the shorter scan time makes 3D imaging less sensitive to motion artifacts.
Among the 3D volumetric sequences, 3D gradient-echo MR images with isotropic data acquisition, such as a volumetric interpolated breath-hold examination and THRIVE, may serve as feasible alternatives to 2D SE for the head and neck as well as other parts of the body. A few previous studies have revealed that 3D GRE could provide more accurate tumor size measurement in head and neck cancer and higher sensitivity for detecting primary tumors in patients with cervical lymph node metastasis of unknown primary tumors, compared with 2D SE T1WI.11,12 In particular, because 3D GRE can provide more accurate information of small complex areas (such as the larynx and hypopharynx) and fewer flow-related artifacts, we hypothesized that 3D GRE might perform better diagnostically than 2D SE T1WI in patients with laryngohypopharyngeal cancer.
A previous study devised a new criterion that enabled improved differentiation of neoplastic cartilage invasion from peritumoral inflammation by MR imaging.9 However, it is still challenging to distinguish peritumoral inflammation from neoplastic invasion of thyroid cartilage on MR imaging, and doing so may lead to unsatisfactory specificity and false-positive results.15,22 Furthermore, minimal cortical invasion of tumor on ossified cartilage is also not easily detectable on MR images, resulting in false-negatives.9,15 In our study, we observed 10 false-positive and 3 false-negative cases on 2D SE T1WI, while the number decreased to 6 false-positive and 1 false-negative case on 3D GRE. Therefore, despite the possible disadvantage of a lower signal-to-noise ratio on the 3D sequence, we would expect that 3D GRE with a lesser partial volume averaging effect and higher spatial resolution might enable more accurate differentiation between the inflammatory change and neoplastic invasion of thyroid cartilage as a feasible alternative to ordinary 2D SE T1WI with regard to minimizing false-positive and false-negative cases.
There are several limitations to be addressed. First, radiologists determined the presence of neoplastic thyroid cartilage invasion by visual inspection without measuring the signal intensity of the tissue because these measurements are not usually performed in the clinical setting. Second, during the MR imaging acquisition, 3D GRE was performed first, followed by 2D SE T1WI after contrast injection, without randomizing the order. Nevertheless, scan time delay may not necessarily have affected our study results because the total acquisition time for GRE was approximately 4 minutes. Third, completely blinded interpretations of MR images were not possible because contrast-enhanced 2D SE T1WI and 3D GRE are easily distinguishable by experienced reviewers. Finally, we evaluated the neoplastic invasion of thyroid cartilage only, not the cricoid or arytenoid cartilage in our study. Assessment of tumor extension into the thyroid cartilage was more clinically relevant, and future studies are necessary to validate our study results in the evaluation of cricoid or arytenoid cartilage.
CONCLUSIONS
Contrast-enhanced 3D GRE with 1-mm section thickness and reconstruction had a superior diagnostic performance compared with contrast-enhanced 2D SE T1WI with a 4-mm section thickness in detecting thyroid cartilage invasion in patients with laryngohypopharyngeal cancer. 3D GRE is a clinically relevant and feasible alternative to 2D SE T1WI.
References
- Received December 5, 2020.
- Accepted after revision April 20, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.