
Abstract
BACKGROUND: The overall safety and efficacy of mechanical thrombectomy for anterior cerebral artery strokes remain unclear.
PURPOSE: Our aim was to summarize procedural and clinical outcomes in patients who underwent mechanical thrombectomy for treatment of anterior cerebral artery ischemic stroke.
DATA SOURCES: A systematic literature review was performed using PubMed, Ovid MEDLINE, and the Web of Science from inception until March 4, 2022.
STUDY SELECTION: We identified 9 studies with a total of 168 patients with mechanical thrombectomy–treated anterior cerebral artery occlusions.
DATA ANALYSIS: Recanalization, procedural data, and clinical outcome at last follow-up were collected and summarized. Categoric variables were reported as proportions. The χ2 test of independence or the Kruskal-Wallis test was performed to assess the relationship between selected variables and the anterior cerebral artery embolus type (ie, primary isolated anterior cerebral artery, primary combined anterior cerebral artery, and secondary anterior cerebral artery occlusion) or the mechanical thrombectomy technique.
DATA SYNTHESIS: For mechanical thrombectomy–treated anterior cerebral artery occlusions, recanalization modified TICI 2b/3 was achieved in 80%, postprocedural complications occurred in 17% of patients, and the 90-day mortality rate was 19%. The rate of symptomatic intracranial hemorrhage varied depending on the anterior cerebral artery embolus type (χ2 = 8.45, P = .01).
LIMITATIONS: This analysis did not consider factors such as small-study effects that affect reliability and limit interpretation.
CONCLUSIONS: Mechanical thrombectomy for the treatment of anterior cerebral artery occlusions is safe and efficacious, offering a favorable rate of recanalization and procedural complications. Mechanical thrombectomy–treated anterior cerebral artery occlusions appear to have lower rates of short-term good functional outcomes and an increased risk of symptomatic intracerebral hemorrhage compared with mechanical thrombectomy–treated MCA/ICA occlusions. Single and multicenter studies are needed to further examine the safety and efficacy of mechanical thrombectomy–treated anterior cerebral artery occlusions.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- ICH
- intracerebral hemorrhage
- MT
- mechanical thrombectomy
- mTICI
- modified TICI
Strokes of the anterior cerebral artery (ACA) and its branches account for up to 4.4% of ischemic strokes.1 Although patients presenting with acute occlusion of the ACA can have varied presentations, in up to 90% of patients, motor deficits typically involving the lower extremity contralateral to infarct location are present.1,2 ACA strokes have been associated with disability after discharge due to the resultant motor, cognitive, and behavioral impairments.1,3 In-hospital mortality from isolated ACA territory infarct has been reported to be 8%.1,2 Additionally, emboli in the ACA territory may occur secondary to endovascular treatment involving other territories, leading to increased risk of hemorrhagic complications and mortality, despite successful reperfusion.1,2
While mechanical thrombectomy (MT) has been established as safe and highly effective in the treatment of thromboembolic occlusion of the MCA, ICA, and basilar artery, the safety and efficiency of MT for the treatment of acute ACA occlusions have not been clearly delineated to date.4 Recent single and multicenter studies have provided additional data to examine the complication profile and outcomes related to MT for ACA occlusion.5⇓⇓⇓⇓⇓⇓⇓-13 This systemic review aimed to summarize procedural and clinical outcomes in patients who underwent MT for the treatment of ACA occlusion.
MATERIALS AND METHODS
Electronic Literature Search
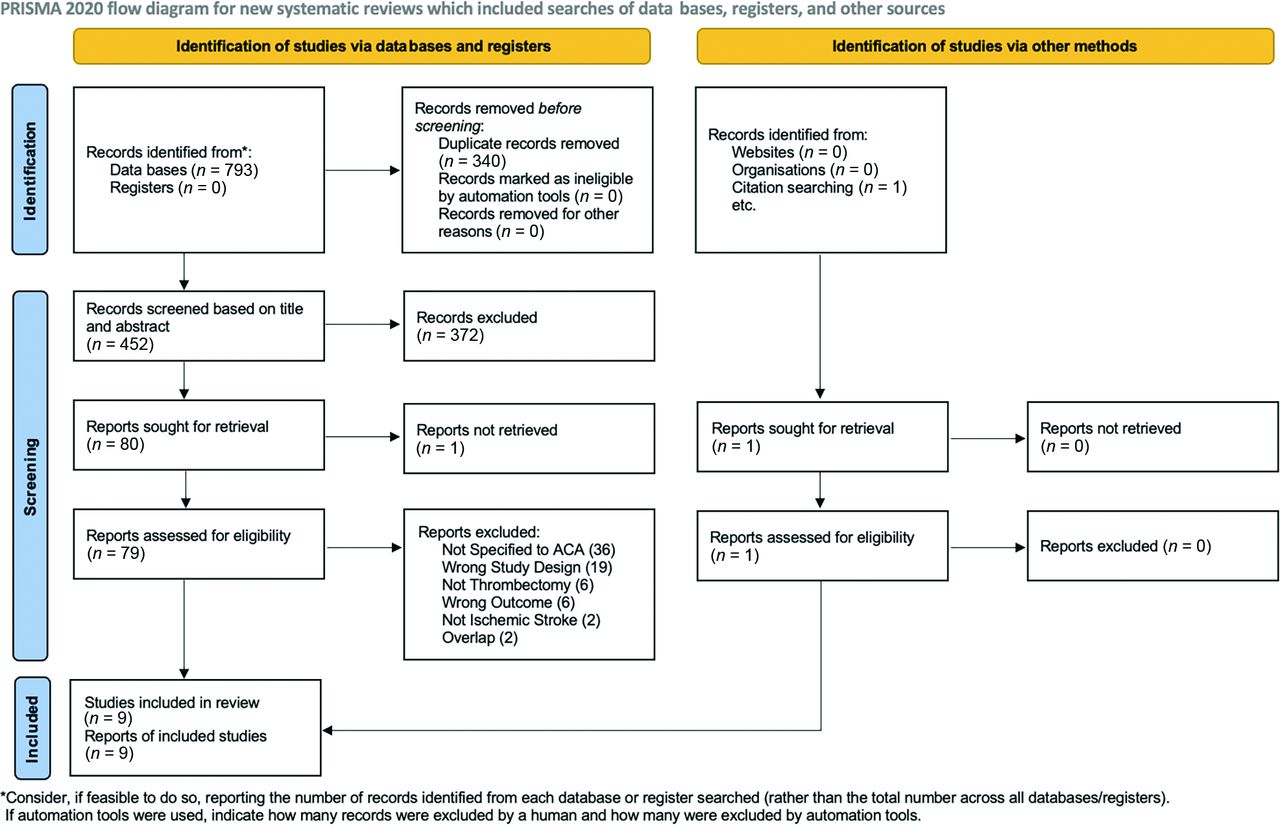
A systematic review of the literature was performed and presented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A PRISMA checklist is provided (Online Supplemental Data). The electronic databases PubMed, Web of Science, and Ovid MEDLINE were searched from inception to March 4, 2022. A keyword search using the Boolean operators OR & AND with terms including “anterior cerebral artery” and “thrombectomy” was conducted (Online Supplemental Data). Duplicates of search results from different databases were identified and removed. A PRISMA 2020 flow diagram is presented in the Figure. The protocol used for this review is provided in the Online Supplemental Data. This protocol was not prospectively registered.

Flow chart showing the study-selection process.
Literature Review
Inclusion and exclusion criteria were determined a priori. Studies that included patients with primary or secondary acute ACA occlusions treated with aspiration or stent-retriever–mediated MT with data related to clinical outcomes were considered. We excluded the following studies: 1) those that were in the form of abstracts, case reports, and editorials; 2) did not include clinical or procedural outcomes related to MT for acute ACA occlusion; or 3) had no English version. Articles that grouped acute ACA occlusions with other territory occlusions in their analysis (ie, did not detail individual characteristics or outcome data of patients with ACA strokes) were also not considered.
All articles were initially screened on the basis of their titles and abstracts. Two authors evaluated full-text articles independently and selected those that fit the inclusion criteria. Reference lists of the selected articles were reviewed to identify articles potentially missed by the electronic literature search.
Data Extraction
One author extracted data from each selected study, which was then verified by an additional author for accuracy. We collected the following baseline data from each included study: age, sex, NIHSS score at admission, ASPECTS, clinical presentation of stroke, stroke etiology (ie, atherosclerotic, cardiogenic), and ACA stroke location (ie, A1–A5). Proximal callosomarginal artery occlusions were grouped with the A4 segment, and distal downstream occlusions of the ACA branches were grouped with A5.
Primary isolated ACA stroke was defined as an acute, isolated ACA occlusion that did not occur due to thrombectomy or thrombolytic therapy. Primary combined ACA occlusion was defined as an ACA occlusion in conjunction with other vessels of the anterior circulation, not resulting from thrombectomy or thrombolytic therapy. Secondary ACA stroke included occlusions of the ACA territory that occurred as a result of the thrombectomy procedure or thrombolytic therapy.
Procedural data collected included the number of patients having undergone thrombolytic therapy, the type of MT technique (ie, stent retriever, aspiration), incidents of procedural failure, time from symptom onset to recanalization, procedural time, number of passes, the modified TICI (mTICI) score, and postprocedural complications. The mTICI score referred to the recanalization score for ACA occlusion. Postprocedural complications were defined as complications that occurred after and could be attributable to the procedure, with or without clinical sequelae. These complications would include hemorrhage and formation of a new embolus. Procedural failure was defined as an inability of device deployment, specifically concerning stent retrievers, due to placement of a guidewire or microcatheter (see the Online Supplemental Data for full definitions). Clinical outcome data collected included the number of patients with intracerebral hemorrhage (ICH), average clinical follow-up time, number of patients available for clinical follow-up, mortality rates (3 months and overall), and the mRS score (3 months and overall).
Primary outcomes were the rate of successful recanalization (mTICI 2b/3) and the rate of good clinical outcome (mRS 0–2) at last clinical follow-up. Secondary outcome measures included rates of postprocedural complications and mortality. The data were further substratified on the basis of primary isolated, primary combined, and secondary ACA occlusion (Online Supplemental Data) and on the type of MT technique (ie, stent, aspiration, hybrid) (Online Supplemental Data). Patients were included in each grouping only if mTICI, intraprocedural complications, ICH, mortality, procedural time, or the mRS score was provided.
Data Synthesis and Quality Assessment
For each included article, continuous variables such as age, ASPECTS, time to recanalization, procedural time, and number of passes were reported as medians with ranges or means (SDs). The crude estimate for each continuous variable was computed as the mean (ie, times) or median (ie, for age, ASPECTS) of all included studies. Categoric variables, such as stroke location (ie, A1–A5), MT technique (ie, stent retriever, aspiration), and postprocedural complications, were reported as proportions for each article. The crude estimate for each variable was the total proportion of all included studies. The χ2 test of independence was performed to assess the relationship between selected variables (ie, mTICI, postprocedural complications, ICH, mortality, mRS) and ACA embolus type or MT technique (Online Supplemental Data). The Kruskal-Wallis test was used to determine significant differences in ASPECTS and NIHSS scores among ACA occlusion types and MT technique (Online Supplemental Data). Statistical analysis was performed using R statistical and computing software, Version 4.2.1 (http://www.r-project.org/). The quality of each study was assessed using the Newcastle-Ottowa Scale (Online Supplemental Data).
RESULTS
A total of 9 studies were included in this review.5⇓⇓⇓⇓⇓⇓⇓-13 The Figure demonstrates the PRISMA flow chart for the selection of studies. The relevant studies differed as far as their scope, which included outcomes of MT for ACA occlusion, outcomes of MT for distal ACA occlusion, comparison of MT and thrombolysis outcomes for ACA occlusion, ACA embolism during MCA thrombectomy, and distal endovascular thrombectomy. Studies varied in the complete clinical, procedural, and outcome data they presented and the degree of statistical analysis. This variation, in addition to the small sample sizes, provides the risk for selection and information bias. The Newcastle-Ottawa Assessment Scale score ranged from 3 to 6 with a median of 6 (Online Supplemental Data).
Patient and ACA Territory Ischemic Stroke Characteristics
Baseline patient and stroke characteristics, procedural details and complications, and clinical outcomes of each individual study are summarized in the Online Supplemental Data. The Online Supplemental Data detail patient demographics and baseline stroke characteristics. Among the 9 studies, there were 168 patients with acute ACA occlusion treated with MT. The median patient age was 74 years (range, 64–80 years) and 47% (77/163) were women. Regarding occlusion type, 43% (72/168), 24% (40/168), and 33% (56/168) had primary isolated ACA occlusion, primary combined ACA occlusion, and secondary ACA occlusion, respectively. Stroke etiology was atherosclerotic in 23% (20/87), cardiogenic in 41% (36/87), and other in 36% (31/87). The location of occlusion along the ACA included the A1 in 13% (18/134), A2 in 43% (57/134), A3 in 22% (29/134), A4 in 21% (28/134), and A5 in 1% (2/134).
The median NIHSS score at admission of all patients was 17.5 (range, 10–24). The median ASPECTS was 8 (range, 7–8.5). Among 18 patients with data regarding clinical presentation, 78% (14/18) and 94% (17/18) presented with speech disturbance and hemiparesis, respectively. Among primary isolated, primary combined, and secondary ACA occlusions, the median NIHSS scores at admission were 18 (range, 10–21), 23 (range, 18–28), and 19 (range, 14–24), respectively (χ2 = 1.13, P = .57) (Online Supplemental Data). The median ASPECTS was ten, 8.5 (range, 8–9), and 8 for primary isolated, primary combined, and secondary ACA occlusion, respectively (χ2 = 2.25, P = .33) (Online Supplemental Data).
Thrombectomy Procedural Characteristics
The Online Supplemental Data summarize procedural characteristics during MT. Thrombolytic therapy was performed in 41% (62/151) of patients. Stent-retriever MT was performed in 65% (85/131) of patients, aspiration was performed in 23% (30/131) of patients, and stent retriever with aspiration was performed in 12% (16/131) of patients.
Procedural failure occurred in 3% (5/168) of patients. The mean time from onset to recanalization was 219 (SD, 50) minutes, and the mean procedural time was 58 (SD, 13) minutes. The median number of passes was 1. mTICI 2b/3 was achieved in 80% (134/168) of all patients included in the study. Among patients with primary isolated ACA occlusion, 74% (37/50) achieved mTICI 2b/3, while 88% (14/16) of primary combined ACA occlusion and 89% (8/9) of secondary ACA occlusion had this result (χ2 = 1.95, P = .38) (Online Supplemental Data). Among ACA occlusions treated with stent retrievers or aspiration alone, mTICI 2b/3 was reached in 82% (42/51) and 94% (17/18), respectively (Online Supplemental Data). When a stent retriever with aspiration was used, mTICI 2b/3 was achieved in 100% (12/12) (χ2 = 3.78, P = .15) (Online Supplemental Data).
Complications and Clinical Follow-up Outcomes
The Online Supplemental Data describe postprocedural complications and clinical follow-up data. Postprocedural complications occurred in 17% (29/168) of patients, with a symptomatic postprocedural complication rate of 11% (19/168). Symptomatic complications included ICH (8.3% [14/168]), cerebral edema (2% [4/168]), and ACA dissection (0.5% [1/168]) (Online Supplemental Data). Symptomatic postprocedural complications occurred in 2% (1/49), 25% (3/12), and 20% (1/5) of patients with primary isolated ACA occlusion, primary combined ACA occlusion, and secondary ACA occlusion, respectively (χ2 = 8.45, P = .01) (Online Supplemental Data). Symptomatic postprocedural complications occurred in 7% (3/44), 56% (9/16), and 25% (3/12) of patients in whom a stent retriever, aspiration, or combination MT technique was used (χ2 = 17.5, P < .01) (Online Supplemental Data). ICH occurred in 13% (22/168) of patients, symptomatic ICH occurred in 8.3% (14/168), SAH occurred in 6% (10/168), and symptomatic SAH occurred in 1.2% (2/168) (Online Supplemental Data). Symptomatic ICH was located in the MCA territory (2.4% [4/168]), ACA territory (0.6% [1/168]), and unspecified location (5.3% [9/168]) (Online Supplemental Data). Among patients with primary isolated ACA occlusion, primary combined ACA occlusion, and secondary ACA occlusion, symptomatic ICH occurred in 2% (1/49), 25% (3/12), and 20% (1/5), respectively (χ2 = 8.45, P = .01) (Online Supplemental Data).
The mean clinical follow-up time was 3 (SD, 0) months. At the 3-month follow-up, 32% (48/148) and 68% (100/148) of all patients had good and poor clinical outcomes, respectively. Overall, 31% (51/163) of patients had a good outcome, and 69% (112/163) had a poor outcome. When we further substratified the results, good clinical outcome was achieved in 48% (24/50), 25% (4/16), and 0% (0/4) of patients with primary isolated ACA occlusion, primary combined ACA occlusion, and secondary ACA occlusion, respectively (χ2 = 5.5, P = .06) (Online Supplemental Data). Additionally, poor clinical outcome occurred in 52% (26/50), 75% (12/16), and 100% (4/4) of patients with primary isolated ACA occlusion, primary combined ACA occlusion, and secondary ACA occlusion, respectively (χ2 = 5.5, P = .06) (Online Supplemental Data). The mortality rate at 3 months was 19% (22/118), and the overall mortality rate was 22% (30/138). Among patients with primary isolated ACA occlusion, primary combined ACA occlusion, and secondary ACA occlusion with specified outcomes, the mortality rates were 47% (8/17), 13% (2/16), and 44% (4/9), respectively (χ2 = 5.07, P = .08) (Online Supplemental Data).
DISCUSSION
An increasing number of ACA occlusions are targeted for endovascular treatment. However, the safety and efficiency of MT for the treatment of acute ACA occlusions have not been clearly defined.4 Here, we identified the literature outlining the outcome data related to ACA occlusions treated with MT. In our review, recanalization was achieved in 80% of patients and postprocedural complications occurred in 17% of patients. At the last clinical follow-up of 3 months, the mortality rate was 19% and the rate of good functional outcome was 32%.
Rigorous clinical trial data support MT in patients with intracranial and extracranial occlusions of the ICA, including tandem or isolated occlusions of the M1 and M2 segments of the MCA.4,14,15 Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke (HERMES), a meta-analysis using individual patient data from 5 of these randomized controlled trials (MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, and EXTENDI IA), found that patients with ICA and proximal MCA occlusions who underwent thrombectomy had similar rates of symptomatic ICH (4.4%) and 90-day mortality (15.3%), with higher rates of functional independence at 90 days (46%) compared with controls (26.5%).16 MT in patients with ACA occlusions may also share similar benefits, specifically improving morbidity outcomes poststroke.17,18 However, because the natural history of these strokes is overall more favorable compared with ICA or MCA occlusions, the risks of MT may outweigh the potential benefits.18 The risk of vessel perforation and vasospasm in MT-treated ACA occlusions may be increased, given the distal location, smaller diameter, and thinner walls of the ACA.17⇓-19 In our review, the overall recanalization rate for MT-treated primary and secondary ACA occlusions was found to be 80% (94% for aspiration, 82% for stent retriever), similar to that of large-vessel occlusions (81.9% for aspiration, 88%–91% for stent retriever).4,20 Procedural time for primary and secondary ACA occlusions treated with MT (58 minutes) was similar to that of MT-treated thrombectomies of the MCA (54–70 minutes).4,17,21 Our data demonstrate that recanalization rates and procedural times in thrombectomy-treated ACA and MCA/ICA strokes are comparable.
Symptomatic complications for MT-treated ACA strokes were ICH (8.3%) and cerebral edema (0.6%). Although the overall rate of symptomatic procedural complications in MT-treated primary and secondary ACA occlusions (11%) is comparable with that of MT-treated MCA/ICA occlusions (range, 7%–16%), in our review, the rate of symptomatic ICH for ACA occlusions treated with MT was found to be greater (8.3%, compared with 4.4% for MT-treated MCA/ICA occlusions).16 This finding may be attributed to more distal and smaller vessel targets that may be injured during ACA MT.7,17 However, among the few studies that reported the location of ICH, the most common location was the MCA territory (2.4% [4/168]). The postprocedural complication rate differed significantly, depending on the type of ACA occlusion. Specifically, primary isolated ACA occlusions were found to be associated with fewer postprocedural complications compared with primary combined and secondary ACA occlusions (χ2 = 8.45, P = .01). The rate of symptomatic ICH also was significantly different among these 3 occlusion types, with primary isolated ACA occlusions associated with the lowest ICH incidence (χ2 = 8.45, P = .01). The symptomatic complication rate for MT-treated ACA occlusions also differed on the basis of the MT technique used, with stent-retriever and hybrid techniques being associated with fewer complications (χ2 = 17.5, P < .01), though in MT-treated MCA/ICA occlusions, the safety profiles of stent and aspiration techniques were similar.4,22
The 90-day mortality rate for MT-treated ACA occlusions (19% [22/118]) was also found to be comparable with that for MT-treated ICA/MCA occlusions in the HERMES meta-analysis (15.3%).7,16 However, relatively fewer patients in our review achieved a good 90-day outcome (32% [48/148]) compared with those with MT-treated ICA/MCA strokes (46% in HERMES).16 We found that patients with primary, isolated ACA occlusions had a relatively greater rate of good outcomes at 90 days (48% [24/50]) compared with those with primary combined (25% [4/16]) or secondary (0% [0/4]) ACA occlusions, though the differences were not statistically significant. Moreover, the rate of good functional outcome at 90 days may be lower in patients with MT-treated ACA strokes compared with the numbers reported for non-MT-treated ACA strokes.1⇓-3 Specifically, patients with non-MT-treated primary isolated ACA occlusions have achieved a 90-day rate of good functional outcome of 85% compared with 48% for MT-treated primary isolated ACA occlusions found in our review.23 In controlled trials comparing MT- and non-MT-treated ICA/MCA occlusions, there were significant differences in good functional outcome that favored MT treatment of selected strokes (46% in MT-treated, 26.5% in controls).16 While there have been no controlled studies to directly compare MT- and non-MT-treated ACA strokes on the basis of initial severity, our findings warrant further investigation to determine the ideal characteristics of ACA occlusions and the patient population that would benefit from MT regarding mortality and morbidity.
Our systematic review of the literature suggests that MT can be used to treat primary or secondary ACA occlusions with recanalization rates, procedural complications, and 90-day mortality comparable with those of MT-treated MCA/ICA occlusions. However, ACA thrombectomy is associated with higher rates of ICH compared with those reported for ICA/MCA thrombectomy, and outcomes of primary ACA occlusion following thrombectomy do not appear to differ from the reported natural history of primary ACA occlusion. Of note, the outcomes are dependent on the type of ACA occlusion (primary, primary combined, or secondary) and type of MT technique used (stent, aspiration, hybrid). Currently, the safety and efficacy of MT in medium-sized cerebral vessels, including the ACA, are being evaluated in the DISTAL multicenter, randomized clinical trial that ends in 2026.24 Until the initial results are known, it is important to understand that the initial baseline functional status of the patient as well as degree of severity of ACA stroke are complex factors to consider when deciding to use MT for the treatment of ACA occlusion
Limitations
We acknowledge several limitations of this review. The relevant studies identified differed as far as their scope and varied in the complete clinical, procedural, and outcome data they presented. Many studies did not report the location, type, or severity of ICH, which may overestimate ACA thrombectomy complications and provide a barrier for decision-making. While many articles screened for full-text review included MT-treated ACA occlusions in their data, they did not specify individual results for this group and could not be included in the analysis. Individual patient data and further subgroup analysis were not possible. As a result, we were unable to completely substratify complications and outcomes on the basis of baseline functional outcomes (ie, baseline mRS score), MT technique used, the use of concurrent thrombolytic therapy, and the type of ACA occlusion (ie, primary, secondary).
We could not directly compare the outcomes of MT-treated ACA occlusions with those of either non-MT-treated ACA occlusions or MT-treated ICA/MCA occlusions because no study to date has produced a comparison. Several studies had small sample sizes, increasing the risk of selection and information bias. The included studies varied as to the degree of statistical analysis because only 2 studies performed a complete multivariable analysis, leading to an increased risk of confounding bias for the remaining studies.
To minimize bias associated with data collection, 2 authors were involved in data extraction; one author (N.D.) conducted the data extraction and rated the certainty of evidence, while the second (P.M.) checked the accuracy of the data. Both authors contributed to data analysis.
CONCLUSIONS
MT for the treatment of ACA occlusions offers a favorable overall safety and efficacy profile associated with rates of recanalization, procedural complications, and mortality comparable with that of MT in larger vessels. However, the rate of short-term good functional outcome appears to be decreased, while the rate of symptomatic ICH seems to be increased compared with MT-treated MCA/ICA occlusions, necessitating the establishment of criteria to determine the appropriate ACA occlusions amendable by MT treatment. More single and multicenter studies are needed to further examine the safety and efficacy of MT in ACA occlusions. Increased operator experience and more direct comparisons with alternative approaches are necessary to establish the optimal treatment for ACA occlusions.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 9, 2022.
- Accepted after revision September 27, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}