
Abstract
BACKGROUND AND PURPOSE: Treatment of PICA aneurysms can be technically challenging by either surgical or endovascular means. Our aim was to report our preliminary experience with intrasaccular flow disruption using the Woven EndoBridge (WEB) for the treatment of proximal PICA aneurysms.
MATERIALS AND METHODS: Sixteen PICA aneurysms treated with the WEB at 3 institutions were retrospectively reviewed. Baseline patient and aneurysm characteristics, procedural specifics, clinical outcomes, and angiographic results were evaluated.
RESULTS: All aneurysms were located at the proximal, anteromedullary segment of the PICA. Seven aneurysms were ruptured. The median aneurysm size was 3.9 mm (range, 2–12 mm), and all aneurysms were wide-neck. WEB deployment failed in 1 case due to WEB protrusion in a small PICA aneurysm. Additional stent implantation was required for 2 aneurysms to improve intra-aneurysmal WEB positioning. One patient developed a partial posterior cerebral artery territory infarction with transient hemianopsia. Intraoperative rerupture of a ruptured aneurysm could be immediately stopped by WEB deployment due to intrasaccular stasis; however, it might have contributed to a slight disability of the patient. At last angiographic follow-up, 12/15 aneurysms (80%) were completely occluded and 3/15 (20%) had a neck remnant.
CONCLUSIONS: The preliminary results indicate that WEB treatment of proximal PICA aneurysms is feasible with a reasonable safety and efficacy profile. The advantages of intrasaccular flow disruption include preservation of the PICA, durable aneurysm occlusion, and omission of antiplatelet therapy. The low-profile WEB 17 delivery system might enable navigation to distal PICA aneurysms, which needs to be addressed further.
ABBREVIATIONS:
- RROC
- Raymond-Roy occlusion classification
- SL
- single-layer
Aneurysms located at the PICA are rare and account for approximately 0.5%–3.0% of intracranial aneurysms. Most PICA aneurysms arise from the proximal (anteromedullary) PICA segment near the PICA–vertebral artery junction.1 PICA aneurysms can be treated by both surgical and endovascular means; however, their location and geometry pose individual challenges for either treatment option. Microsurgical clipping is hampered by a narrow surgical corridor and the proximity to the brainstem and cranial nerves IX–XI, allowing only minimal manipulation.2 Established endovascular treatment options for PICA aneurysms include conventional coiling, stent-assisted coiling, balloon-assisted coiling, flow diversion, and, last, parent artery occlusion as the final option. Challenges of the endovascular technique include a broad-based neck anatomy and a small PICA caliber, especially at peripheral aneurysm locations. Moreover, particularly in the proximal location, parent vessel sacrifice should be prevented due to the risk of brainstem and cerebellar infarction.
The concept of intrasaccular flow disruption has not yet been evaluated systematically for PICA aneurysms. The Woven EndoBridge (WEB; Sequent Medical) represents the most studied flow disrupter to date. It consists of a spherical mesh of nitinol wires, which is placed within the aneurysm sac, leaving the parent artery unaffected. It causes an immediate flow-disrupting effect at the aneurysm ostium, leading to subsequent thrombosis of the aneurysm sac with time. The safety and efficacy of the WEB have been demonstrated by numerous studies, predominantly for wide-neck bifurcation aneurysms located at the anterior communicating artery, the middle cerebral artery bifurcation, and the basilar apex.3⇓⇓-6 Further refinements of the WEB include a low-profile, 0.017-inch delivery system for navigation into small-vessel diameters.7
The present case series reports our preliminary multicenter experience in treating PICA aneurysms with the WEB.
MATERIALS AND METHODS
All patients treated with the WEB for a PICA aneurysm at 3 neurovascular institutions between 2011 and 2021 were retrospectively reviewed and included on an intention-to-treat basis. There were no exclusion criteria. In accordance with the institutional guidelines, an ethics committee approval was waived due to the retrospective study design.
Procedure
Treatment options for each individual PICA aneurysm were discussed between interventional neuroradiologists and vascular neurosurgeons. The WEB was predominantly selected for wide-neck bifurcation aneurysms, which were inappropriate for conventional coiling as an alternative endovascular treatment option for stent-assisted procedures and parent artery occlusion.
All procedures were performed via a transfemoral approach with the patient under general anesthesia in a biplane angiosuite (Philips AlluraClarity FD 20/15, Philips Healthcare and Siemens Artis Q, Siemens). The standard setup consisted of a triaxial system. A 6F guide catheter was navigated via a 6F sheath to the vertebral artery/PICA junction. The Sofia 5F catheter (MicroVention) was used as an intermediate catheter. Finally, a dedicated VIA microcatheter (Sequent Medical) was inserted coaxially to deploy the WEB.
As measured on 2D DSA, the WEB device was chosen to be slightly larger than the aneurysm width and slightly smaller than the aneurysm height (+1/–1 rule) for optimal aneurysm occlusion.
Antiaggregation Therapy
Patients with unruptured aneurysms were loaded with acetylsalicylic acid, 100 mg/day, 5–7 days before the procedure. After groin puncture, 5000 IU of heparin was administered, followed by aliquots of 1000 IU/h until the end of the procedure. After WEB implantation, acetylsalicylic acid, 100 mg/day, was given for 4–6 weeks. Patients with ruptured aneurysms received neither antiplatelet therapy nor IV administration of heparin. After additional stent implantation, a dual-antiplatelet regimen of clopidogrel, 75 mg/day, for 4 months and acetylsalicylic acid, 100 mg/day, life-long was administered.
Data Collection
Patient charts were retrospectively reviewed to collect patient age, sex, ruptured/unruptured aneurysm status, World Federation of Neurosurgical Societies grade, endovascular technique, complications, and clinical outcome. Baseline angiograms were reviewed to determine PICA location, aneurysm size, neck width, dome-to-neck ratio, and shape. Proximal PICA location refers to the PICA–vertebral artery junction and the anteromedullary segment of the PICA. Aneurysms arising beyond the anteromedullary segment were classified as distal. All complications are reported regardless of their clinical significance. The single-layer (SL) and single-layer sphere WEB types were used. Since September 2018, the WEB 17 was used for aneurysms of <7 mm. Clinical outcome was evaluated with the mRS score. Aneurysm occlusion was evaluated immediately after the procedure and on follow-up angiograms using the Raymond-Roy occlusion classification (RROC): complete occlusion (RROC I), neck remnant (RROC II), and aneurysm occlusion (RROC III).
Statistical Analysis
Descriptive statistics were used.
RESULTS
Patient and Aneurysm Characteristics
Among 105 patients with PICA aneurysms treated at the 3 institutions during the study period, 16 patients underwent WEB embolization (15.2%). The median patient age was 60.5 years (range, 48–78 years), and all patients were women. Seven aneurysms (43.8%) were ruptured. The median aneurysm size was 3.9 mm (range, 2.2–12.0 mm), the median neck width was 3.4 mm (range, 1.7–7.4 mm), and the median dome-to-neck ratio was 1.3 (range, 0.9–2.6). All aneurysms were saccular. Individual patient and aneurysm characteristics are given in Table 1.
Baseline patient and aneurysm characteristics
Aneurysm Treatment
Procedural specifics and patient outcome are detailed in Table 2. WEB deployment was feasible in all cases except one. In case 12, treatment of a small PICA aneurysm (2 mm) with the smallest available WEB in stock (SL, 3.5 × 2 mm) failed because the WEB was too large and it protruded into the parent artery (Fig 1). Due to WEB-induced vessel stenosis, additional stent implantation seemed inappropriate. Hence, the WEB was carefully removed before detachment, and the aneurysm was subsequently coiled in the same procedure. In case 2, the patient with a ruptured PICA aneurysm was treated with an additional stent in a staged procedure to improve intrasaccular WEB positioning and, subsequently, aneurysm occlusion. This case is presented in Fig 2. In case 11, the WEB tended to protrude into the parent artery as well; this protrusion could be counteracted by additional implantation of a low-profile stent. Complications occurred in 3 procedures (18.8%). In the first patient (case 1), an apposition thrombus occurred at the WEB, which could be dissolved with tirofiban. The patient had no infarction and no neurologic deficits. In the second patient (case 4), a ruptured PICA aneurysm reruptured immediately after intrasaccular WEB deployment; however, the bleeding stopped shortly thereafter due to intrasaccular stasis. Although cerebral infarction was not seen on follow-up imaging, the rebleeding might have contributed to the slight-but-permanent disability of the patient after SAH (mRS 1). This case is illustrated in Fig 3. In the third case (case 5), the patient had a partial posterior infarction, which was associated with transient hemianopsia, probably due to a procedural thromboembolism. Figure 4 depicts a further case of successful WEB embolization.

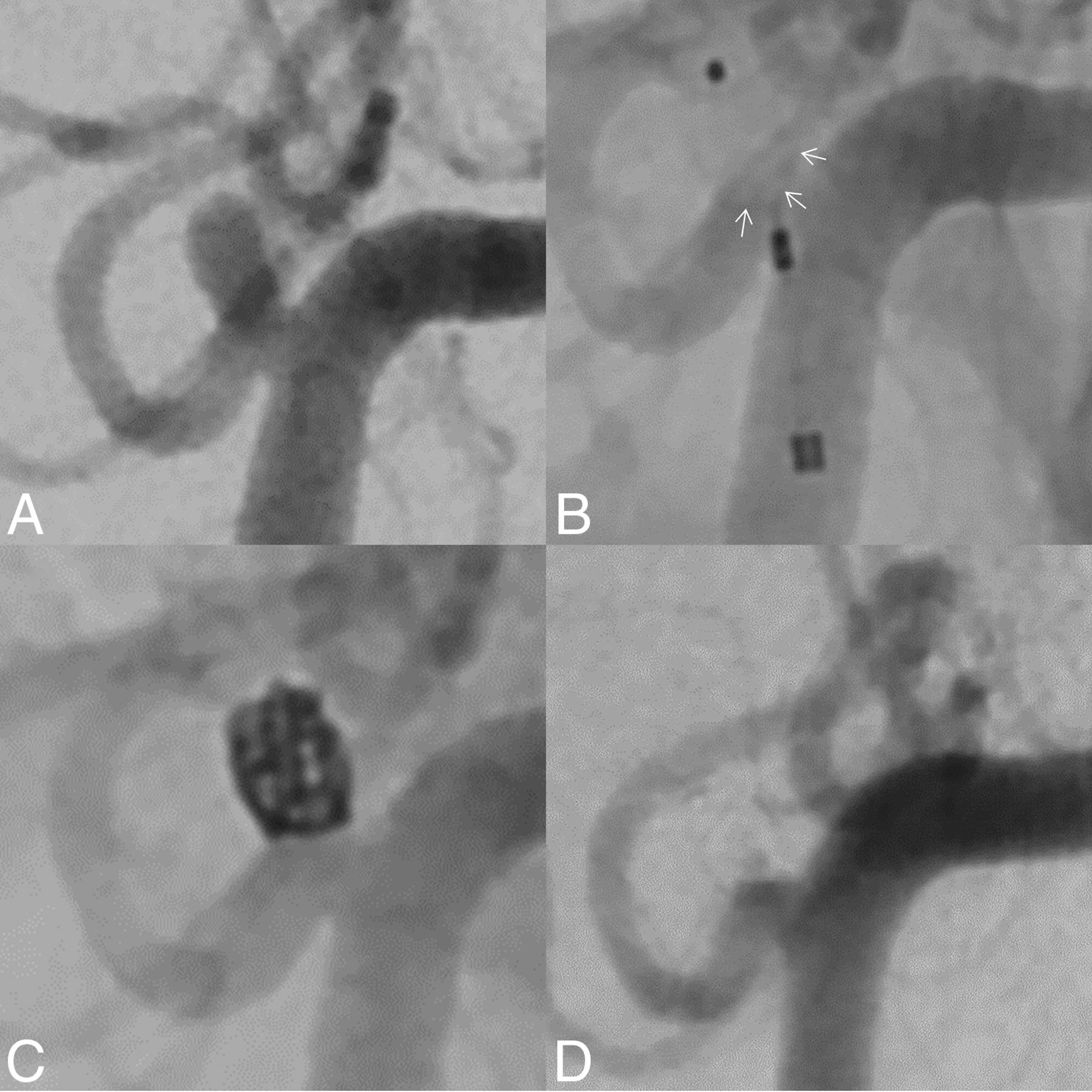
DSA shows a small, proximal PICA aneurysm (2 mm) in a patient with an SAH (A). Due to the broad neck of the aneurysm, the smallest available WEB in stock (SL, 3.5 × 2 mm) was deployed (B). However, the lower base of the WEB protruded markedly into the parent vessel (WEB contour highlighted by arrows). Implantation of an additional microstent seemed contraindicated because it might occlude the parent vessel (diameter, 1.3 mm) and would require permanent antiplatelet therapy. Hence, the WEB was removed before deployment, and the aneurysm was treated by implantation of a single coil (C). At final angiographic follow-up (21 months), the aneurysm was fully occluded and the PICA remained patent (D).

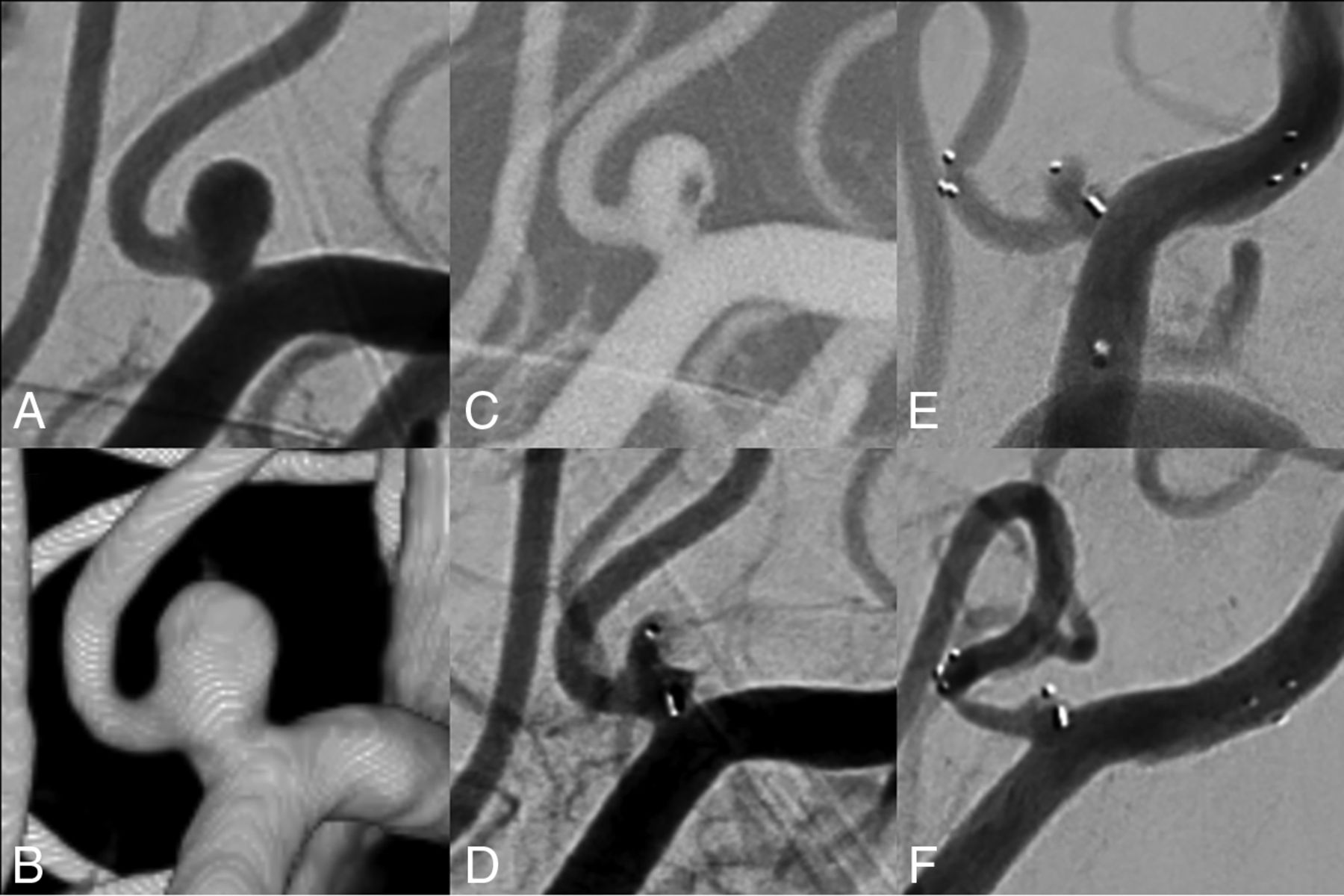
DSA shows a ruptured proximal PICA aneurysm (3.2 mm; neck width, 3.0 mm; dome-to-neck ratio, 1.1 mm) (A and B). Due to the broad-based geometry and the ruptured aneurysm status, intrasaccular flow disruption was envisaged. After probing the aneurysm with a low-profile VIA 17 microcatheter (C), a WEB 17 SL (4 × 2 mm) was placed within the aneurysm sac, achieving immediate contrast stasis to prevent aneurysm rerupture (D). After neurointensive care treatment of the patient, the aneurysm showed persistent residual filling. Hence, an Acclino microstent was placed across the aneurysm neck from the PICA into the distal vertebral artery to optimize WEB positioning (E). At 3-month angiographic follow-up, the aneurysm was completely occluded. There was a moderate in-stent stenosis, which was asymptomatic (F).

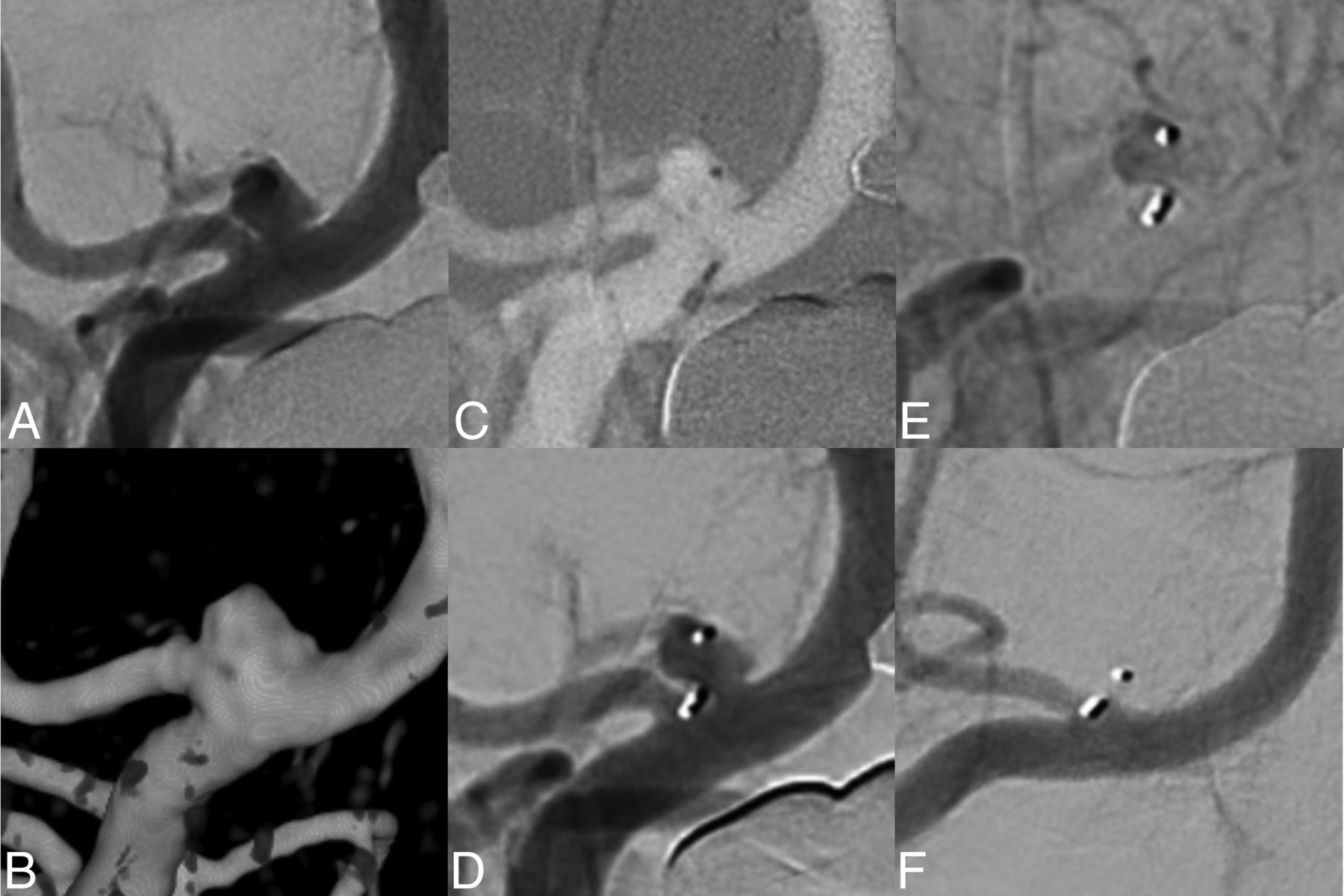
A 51-year-old female patient presented with a ruptured aneurysm at the proximal PICA (A and B). The aneurysm reruptured while the aneurysm sac was probed with the microcatheter. Extravasating contrast can be seen on the angiogram (C). However, directly after WEB deployment, the bleeding stopped due to intrasaccular stasis (D). Cerebellar infarction and herniation were excluded by a control CT (not shown). Although experiencing severe vasospasm, the patient survived and was transferred to a rehabilitation center with mild neurologic deficits (mRS 1). At 2 months, the WEB seemed to be fully thrombosed (E); however, the origin of the PICA, in particular the V4/PICA junction, appears to be dysplastic, warranting further angiographic control.

DSA (A) and 3D reconstructions of rotational data sets (B) show an unruptured wide-neck aneurysm at the branching of the PICA from the vertebral artery. Due to its very broad-based geometry, treatment by conventional coiling is not feasible. To avoid crossing-over stent-assisted coiling, WEB embolization was envisaged. After we probed the aneurysm sac with a low-profile VIA 17 microcatheter (C), a WEB SL 3.5 × 2 cm was implanted (D), which sealed the aneurysm at its neck level and maintained full patency of the PICA. Immediate angiographic control after WEB implantation shows contrast stasis within the WEB (E). Six-month DSA shows complete aneurysm occlusion (RROC I) and patency of the PICA (F).
Procedural specifics
Angiographic Outcome
Immediate complete aneurysm occlusion was achieved in 3 patients (18.8%), 4 had a neck remnant (25.0%), and 9 (56.3%) had an aneurysm remnant. The coiled PICA aneurysm after failed WEB implantation had a small neck remnant, which progressed to complete occlusion at follow-up (Fig 1). Among 15 patients available for angiographic follow-up in the intention-to-treat cohort (median, 6 months; range, 1–21 months), 12 aneurysms (80.0%) were completely occluded and 3 (20.0%) had a neck remnant. There were no aneurysm remnants. Among 14 patients eventually treated with the WEB, 11 showed complete occlusion (78.6%) and 3 had neck remnants (21.4%). All followed aneurysms with an initial RROC III improved to RROC I or II, respectively. There was no aneurysm recurrence. At clinical follow-up, of 16 patients, 13 (85%) had a favorable outcome (mRS ≤1) and 3 patients had an mRS > 1, mainly due to the sequelae of SAH (cases 6, 9, and 13).
DISCUSSION
In the present study, we presented our multicenter experience in the treatment of wide-neck proximal PICA aneurysms with the WEB. WEB deployment was technically successful in all cases except one, and required additional stent implantation in 2 cases. In 1 case, procedural aneurysm rerupture might have contributed to a slight permanent SAH-related disability. At angiographic follow-up, the complete occlusion rates were 80% in the intention-to-treat cohort and 78.6% in the per-protocol group. There was no aneurysm recurrence, and no aneurysms were retreated.
Endovascular embolization has bec-ome the treatment of choice for PICA aneurysms because surgical therapy is associated with a high neurologic complication rate due to the proximity to the brainstem and the lower cranial nerves. For instance, Horowitz et al8 reported an overall complication rate of 68% after surgical PICA repair. In the surgical study by Al-Khayat et al,2 postoperative temporary and permanent lower cranial nerve palsies were observed in around 50%. Although lower cranial nerve palsies can resolve with time, surgery is generally reserved for complex aneurysms and distal locations that are difficult to treat by endovascular means.
The largest study on endovascular PICA aneurysm treatment to date has been published by Chalouhi et al9 and comprised 76 patients treated by conventional coiling, stent-assisted coiling, balloon-assisted coiling, and parent artery occlusion. The technical success rate was 96%. Complications were reported in 12.7%, and permanent morbidity, in 2.8%. In 90% of proximal PICA aneurysms, the parent artery could be preserved.
Proximal PICA aneurysms located at the anterior medullary, lateral medullary, and tonsillomedullary segments pose a particular challenge because parent artery sacrifice should be avoided due to brainstem perforators.10 Among 6 proximal PICA aneurysms treated by parent artery occlusion in the study by Peluso et al,11 1 patient developed hemiparesis due to lateral medullary and cerebellar infarction and 3 had small asymptomatic infarctions. For small-neck aneurysms, conventional coiling is often feasible, but recurrence rates were reported to be >20%.9 Furthermore, PICA aneurysms often present with a wide neck, which would require stent- or balloon-assisted coiling or flow diversion. However, navigation of conventional 0.021- and 0.027-inch stent delivery systems into the PICA is hampered by a sharp angle at the vertebral artery/PICA junction and the small-vessel caliber.11 In this context, low-profile stents and delivery systems seem to bring benefit for stent implantation in the PICA. In a small series by Samaniego et al,12 treatment with the Low-profile Visualized Intraluminal Support (LVIS Jr; MicroVention) device was successful in all 7 cases, and there was no treatment-related morbidity. However, even if stent implantation is possible, there is an enhanced risk of acute thrombotic stent occlusion due to the small-vessel diameter of the PICA.
Intrasaccular flow disruption with the WEB has become a proved treatment concept for wide-neck bifurcation aneurysms. In 2019, the WEB received US FDA approval for anterior communicating artery, MCA bifurcation, terminal ICA, and basilar apex aneurysms.13 As a purely intrasaccular device, the WEB causes immediate flow disruption through the aneurysm ostium, leading to subsequent aneurysm thrombosis, and it does not require antiaggregant therapy urgently, making the device suitable for treatment of ruptured aneurysms.14 Due to its spherical shape, the WEB can be generally securely anchored in wide-neck aneurysms without a supporting stent.
The efficiency of the WEB is well-documented. In the cumulative population of the WEB Clinical Assessment of IntraSaccular Aneurysm Therapy (WEBCAST) trial, WEBCAST-2, and the French Observatory studies, complete and adequate occlusion was reported in 52.9% and 79% at 1 year, respectively.15 Between the 1- and 3-year follow-ups, aneurysm occlusion was stable or improved in 87%, and the overall retreatment rate was 11.4%.4
Owing to these promising results, the indication for WEB embolization has been subsequently extended to further aneurysm locations such as the paraophthalmic ICA16 and narrow-neck aneurysms.17
In our experience, PICA aneurysms often have a spherical, saccular shape, which is suitable for the WEB. Moreover, the novel WEB 17 can be delivered via a 0.017-inch low-profile microcatheter, which might facilitate navigation into the PICA.
Recently, Khattar et al18 reported a case of WEB embolization of a ruptured, dissection-related distal PICA aneurysm (5 mm) with a WEB SL 4 × 3 mm, which is compatible with a low-profile 0.017-inch microcatheter. Navigation toward the aneurysm and WEB deployment were not problematic despite the small-vessel caliber. The authors reported immediate intrasaccular stasis and complete aneurysm occlusion at follow-up.
In the current series, we presented 16 broad-based aneurysms at the PICA–vertebral artery junction, which were treated with the WEB. However, treatment with WEB implantation only was feasible in 13 cases (81%). In 1 case, WEB embolization failed due to WEB protrusion, and in 2 further cases, additional stent implantation was necessary to improve the WEB positioning. In the 2 latter cases, the advantages of the WEB, namely preservation of the parent artery and omission of antiplatelet therapy, were counteracted. However, additional stent implantation can serve as salvage therapy if treatment by the WEB is technically impossible. All aneurysms showed complete occlusion or neck remnants at angiographic follow-up, comparing favorably with the 21% recurrence rate reported by Chalouhi et al9 for coiling. The PICA remained patent in all cases, both during the intervention and at follow-up. One patient developed transient anopsia, which was probably caused by a detached apposition thrombus.
In 1 case, the aneurysm reruptured during WEB deployment caused by the microcatheter. PICA aneurysms have been reported to be susceptible to intraoperative rupture, as demonstrated by a 19% rupture rate in the study by Peluso et al.11 The authors suggested that a small aneurysm size and the upward projection of most PICA aneurysms could lead to a slack in the microcatheter caused by the V3 loop of the vertebral artery, which could be transferred in an upward jump of the catheter during pushing, resulting in rupture of the aneurysm dome.11 Noteworthy, the bleeding stopped directly after subsequent WEB deployment due to intra-aneurysmal stasis. Most important, there was no treatment-related permanent morbidity in our series.
In conclusion, the results imply that the WEB is suitable for proximal PICA aneurysms, offering good angiographic results and sufficient safety. Hence, the WEB may become a further treatment option for PICA aneurysms, in particular for wide-neck aneurysms that are difficult to treat by coiling only. However, further studies will be required to establish the WEB as a primary tool for PICA aneurysms, especially at more distant locations.
Limitations
The limitations of the current study include a moderate number of included patients and the retrospective study design. All aneurysms were located at the proximal PICA; hence, the feasibility of the WEB for distal PICA aneurysms remains uncertain. Finally, long-term angiographic outcome was not reported and needs to be addressed further.
CONCLUSIONS
Due to the typically broad-based anatomy of PICA aneurysms, bare coiling can be challenging and might require implantation of a supporting stent. Due to the saccular, broad-based shape, WEB implantation would often be suitable for PICA aneurysms, as was the case in the present study. Additional stent implantation could be avoided in most cases, there was no major treatment-related morbidity, and retreatment was not required in any case. Further studies are warranted to confirm our preliminary results and establish the WEB for this specific aneurysm location.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received January 24, 2022.
- Accepted after revision May 12, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.