
Abstract
SUMMARY: The term ecchordosis physaliphora (EP) has been used historically to describe a benign notochordal remnant with no growth potential, most commonly occuring in the central clivus. Unfortunately, the radiologic appearance of EP overlaps considerably with the appearance of low-grade chordomas, which do have the potential for growth. In this article, we review new pathologic terminology that better describes this family of diseases, and we propose new radiologic terms that better address the uncertainty of the radiologic diagnosis. The surgical importance of accurate terminology and the implications for patient care are discussed.
ABBREVIATIONS:
- BNCT
- benign notochordal cell tumor
- EP
- ecchordosis physaliphora
Ecchordosis physaliphora (EP) is a term that has been traditionally used for a notochordal remnant that arises from ectopic rests, most commonly at the spheno-occipital synchondrosis of the clivus. It is characterized by a low proliferative index, a lack of bony invasion, small size, and no clinical symptoms.1 It is usually discovered incidentally on neuroimaging performed for other reasons. Since the establishment of the defining histopathologic criteria, the pathology nomenclature has been revised from EP to benign notochordal cell tumor (BNCT).2 Unfortunately, the radiologic and pathologic features of BNCT overlap those of clival chordoma, the malignant counterpart of EP, which similarly derives from notochordal remnants.3 Although attempts have been made to differentiate EP from chordoma, no definitive radiographic parameters have been validated. Furthermore, histologic features of these entities overlap and can be subjective in borderline cases. Therefore, we suggest that radiologists abandon the potentially misleading term EP in favor of the more modern terminology. Notochordal remnants are best understood as a spectrum of disease ranging from benign to low-grade to frankly malignant.
Case Presentation
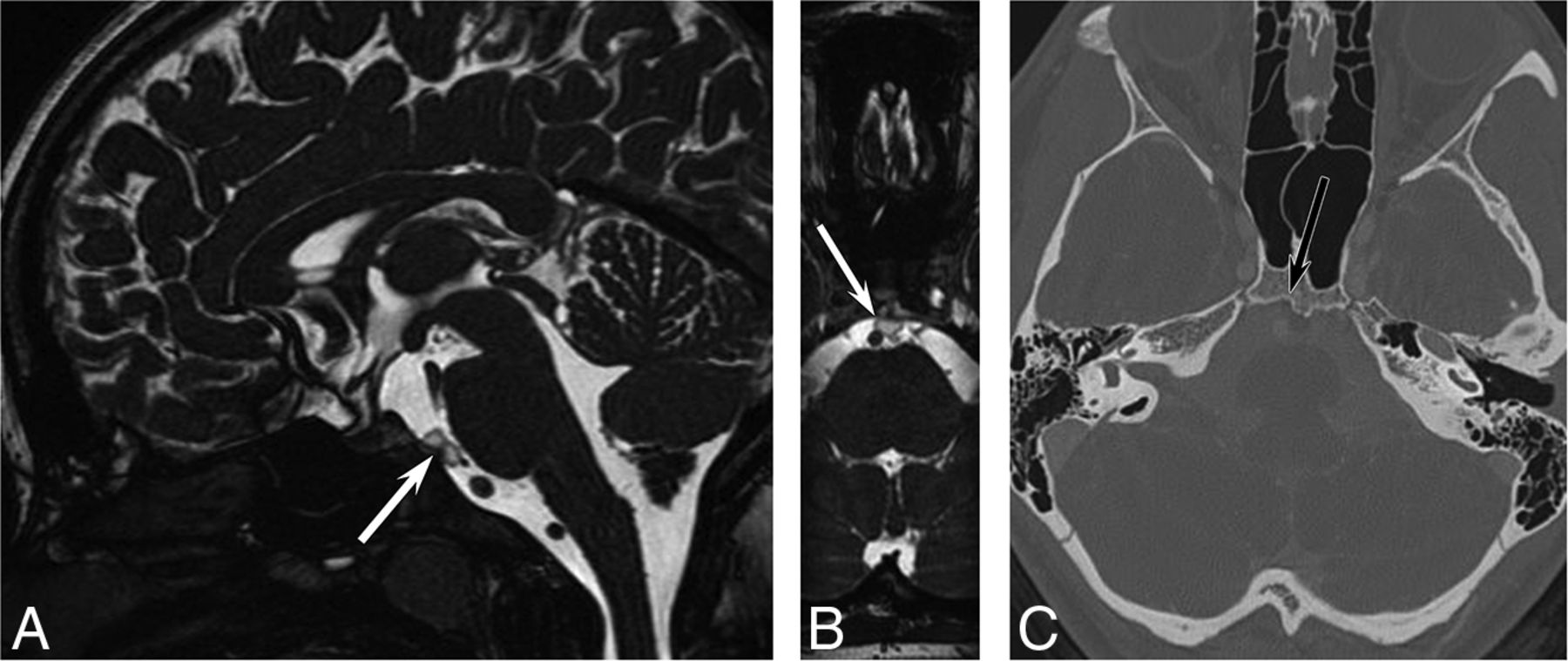
A previously healthy 16-year-old girl underwent MR imaging for headaches. The examination findings were normal except for a well-defined 5-mm T2-hyperintense prepontine mass with a dark rim and clival extension (Fig 1). A CT was performed for further characterization, showing a well-defined sclerotic margin to the clival component. There was no associated enhancement or mass effect. The interpreting radiologist stated that the lesion presumably represents ecchordosis physaliphora, and long-interval follow-up imaging was recommended.

A 16-year-old girl with headaches. A, Sagittal steady-state free precession MR imaging shows a lobular, well-defined T2-hyperintense lesion (arrow) in the prepontine cistern. Axial reformatted image (B) shows a benign-appearing abutment to the clivus. Axial CT (C) shows slight remodeling of the posterior clivus without erosion.
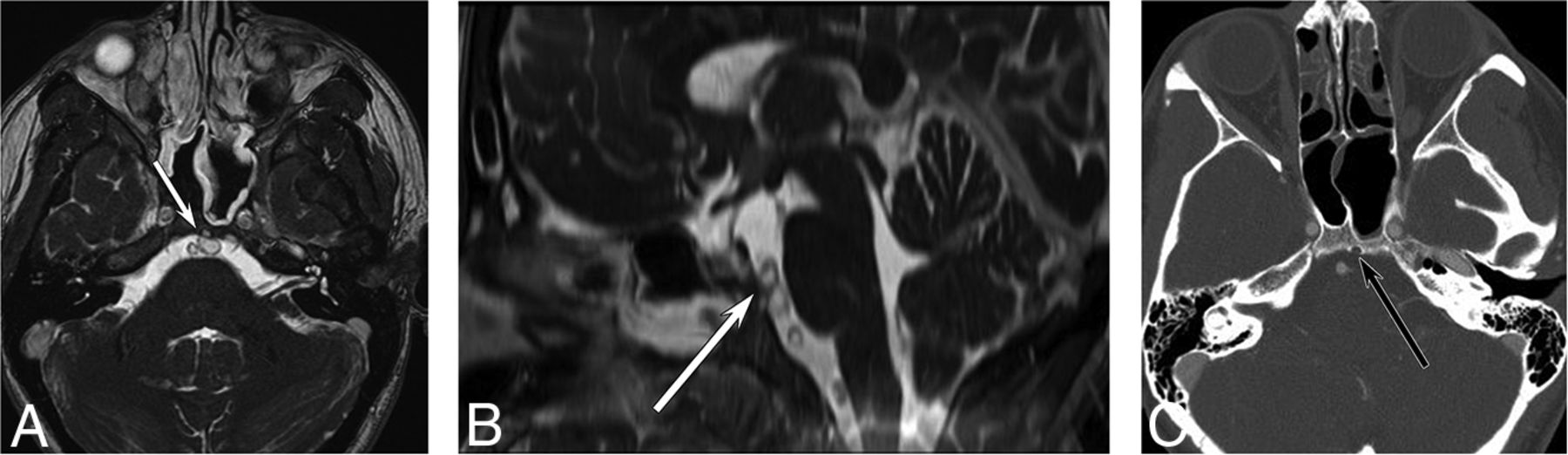
The patient returned 4 years later with recurrent headaches and again underwent MR imaging (Fig 2). The lesion had marginally enlarged but retained all of its benign features. Because of the change in size, the neurosurgery team advised resection, and the patient agreed. The resection was accomplished with an endoscopic endonasal transclival resection.4 Histopathologic analysis (Fig 3) revealed a neoplasm composed of cells with multivacuolated (physaliphorous)-to-eosinophilic cytoplasm embedded in a myxoid background, with a chronic lymphocytic inflammatory infiltrate seen in fibrous septa separating the lobules of the tumor. There was a variable degree of nuclear enlargement, hyperchromasia, and nuclear membrane irregularities. Mitotic activity was sparse, and the Ki-67 proliferation index was very low (<1%), indicating indolent or benign disease. However, no amplification of 1p36 or 9p21 was detected with fluorescence in site hybridization, so the tumor could not be classified as having minimal risk. Lobules of the tumor were identified intradurally as well as extending into the clivus, indicating some degree of aggressive features. Immunohistochemical staining for Brachyury showed strong, diffuse nuclear staining, confirming notochordal origin. When all of the histopathologic, genetic, and fluorescence stain data were taken into consideration, a diagnosis of low-grade chordoma was made, with a description of the relatively bland histologic features displayed by the tumor. Follow-up MR imaging 6 months later revealed no evidence of residual disease.

Follow-up imaging 4 years later. Axial steady-state free precession MR imaging (A) shows increased lesion size (arrow) with new involvement of the clivus. Sagittal reformat (B) shows increased superoinferior extent. The clival involvement is confirmed on axial contrast-enhanced CT (C).

H&E-stained sections demonstrate a lobulated neoplasm composed of predominantly physaliphorous cells in a myxoid extracellular matrix, with a chronic inflammatory infiltrate centered in the fibrous septa (A) and extending to involve clival bone (B). Higher-power view shows cells with nuclear enlargement and atypia (C). An immunohistochemical stain for Brachyury shows strong diffuse nuclear staining in tumor cells (D).
On a follow-up visit, the patient asked whether the lesion should have been resected when she first presented at age 16 and, in particular, whether the extent of surgery would have been less at that time.
Notochordal Embryology
Notogenesis is the formation of the embryologic notochord from precursor epiblasts during the third week of fetal development. The notochord initiates the process of neurulation, which results in the development of the CNS. On the formation of the brain and spine, the notochord regresses into the nucleus pulposus. Incomplete regression can result in persistence of isolated notochordal remnants, which are a potential source of neoplastic disease. Notochordal remnants usually remain near the midline, with a predilection for the sacrococcygeal region and the spheno-occipital synchondrosis.5⇓-7 Both benign entities (BNCT) and malignant entities (chordoma) can occur in these locations, presumably originating from these remnants.
EP/BNCT
BNCTs (a term that encompasses both extraosseous lesions [EP] as well as intraosseous notochordal remnants) are typically asymptomatic, so the lesions are often discovered incidentally when imaging for other reasons. A radiologic hallmark of BNCT that can be detected on CT or MR imaging is a small bony stalk or pedicle projecting from the basal portion of the clivus.8 Like other radiologic features, however, this parameter may only be used to suggest BNCT over other retroclival pathologies such as epidermoid or neurenteric cysts.9 Other nonspecific MR imaging findings include T1-hypointensity, T2-hyperintensity, lack of gadolinium enhancement, and lack of bony erosion.10 A diagnosis of BNCT is often made presumptively on imaging without histopathologic proof, because excisional biopsy is considered overly invasive for a benign disease.
Histologically, BNCTs display sheets of physaliphorous cells, which are characterized by mucin-containing intracytoplasmic vacuoles and lack lobular architecture, fibrous septa, necrosis, and nuclear atypia that characterize chordomas. The lesions are often hypocellular, have bland nuclear features, and lack mitoses. BNCTs also have a low Ki-67 proliferation index, indicating low growth potential.11,12 However, there can be substantial overlap in the histology and immunophenotype of BNCT and chordoma, and the architectural features that help distinguish these entities may be difficult to appreciate on surgical samples of small lesions. Similar challenges can arise in distinguishing a BNCT from a chordoma in the lumbosacral spine, and the term “atypical notochordal cell tumor” has been recently proposed for cases that defy definitive classification.13
Chordoma
Chordomas are typically locally invasive, aggressive tumors that are presumed to arise from persistent notochordal cells. They can arise anywhere along the craniospinal axis, with a predilection for the base of the skull and sacrococcygeal region. Histologically, conventional chordomas are composed of the same physaliphorous cells seen in benign notochordal cell tumors, along with eosinophilic cytoplasm and intracytoplasmic vacuoles.14 Interspersed within the physaliphorous cells are variable amounts of myxoid material, which results in variable imaging characteristics for this tumor.15 The tumors typically have a capsule and grow in lobules separated by fibrous septa, often accompanied by an inflammatory infiltrate. The degree of nuclear pleomorphism and mitotic activity is highly variable, with conventional chordomas ranging from histologically bland tumors with mild nuclear atypia, sparse mitotic activity, and low proliferative activity, up to more overtly atypical, highly proliferative lesions. Poorly-differentiated chordomas are defined by loss of nuclear INI-1 (SMARCB1) expression and often have increased cellularity and mitotic activity. A dedifferentiated chordoma consists of a frankly sarcomatous component juxtaposed with conventional chordomas. Poorly differentiated and dedifferentiated chordomas are quite rare, with conventional chordomas (including the chondroid subtype) accounting for ∼95% of all tumors. Within conventional chordomas, histologic grading criteria to stratify tumor behavior do not exist, though molecular panels to improve prognostication have been recently developed.16,17 By definition, chordomas are considered malignant and are thus capable of locally destructive behavior and metastasis.18
The radiologic appearance of conventional chordoma depends on location, aggressivity, and molecular makeup. On MR imaging, chordomas are typically lobular, septate, and heterogeneous, showing hypointensity on T1-weighted images (but frequently containing high-signal foci) and hyperintensity on T2-weighted images. Enhancement after gadolinium administration is also heterogeneous and often septal, with myxoid areas enhancing poorly.19
Due to the infiltrative nature of these tumors, they often present clinically with pain and site-related neurologic symptoms. Cranial and skull base chordomas may present with headache or cranial nerve dysfunction. The most frequently affected cranial nerve is the abducens nerve (CN VI) because it is exposed to clival tumors while traveling through the Dorello canal along the posterior clivus in the clival venous plexus.20 In rare cases, clival chordomas can present with rhinorrhea due to CSF leak.21 Craniocervical and cervical chordomas tend to present with nonspecific neck and upper-extremity pain. Dysphagia may be present due to mass effect. Thoracic, lumbar, and sacral chordomas tend to present with nonspecific dull pain.22
Although chordomas have a slow rate of progression, they are associated with substantial morbidity from mass effect.23 If a biopsy confirms the diagnosis of chordoma, en bloc resection with wide margins is performed.24 Chordomas have a high rate of reoccurrence, so adjuvant radiation and yearly MR imaging surveillance are often recommended.25
Recent data suggest that homozygous 9p21 deletions (p176/CDKN2A) and 1p36 deletions can further risk-stratify chordomas, even within the “conventional chordoma” category, and are predictive of progression-free survival.16,17 These markers were also found to be relevant to seeding.26 Depending on the prevalence of these deletions within the tumor cells, skull base chordomas can be further classified into an indolent group A, a highly aggressive group C, and an intermediate group B. According to this data set, radiation therapy did not confer any benefit after complete resections in groups A and B.17 Tumors in group A were more likely to be found in younger patients, were smaller, and were more likely to be asymptomatic on presentation. This group may encompass cases that would more accurately be described as EP or BNCT. Whether circulating tumor DNA would have a role in differentiating EP/BNCT from chordomas remains to be determined.27
Spectrum of Disease
Unfortunately, low-grade chordomas may have imaging features that overlap with the classic imaging appearance of BNCT. Imaging differentiation relies on sequential imaging, with BNCT remaining stable indefinitely and low-grade chordoma slowly enlarging. However, there is no established minimum rate of growth that indicates chordoma. Thus, it is difficult to recommend imaging intervals that would properly assess growth rates of a tumor with uncertain malignant potential. Furthermore, there are cases of presumed BNCTs that, on later excisional biopsy, are better classified as chordomas (as exemplified in the above case presentation). Several cases of BNCT have been published that displayed atypical characteristics, with resemblance to chordomas clinically or radiologically.28⇓-30 Similarly, there are documented cases of chordoma that display a low proliferative index, a diameter of <2 cm, and a lack of any clinical symptoms, with detection occurring only incidentally.3,31⇓-33
Given the overlap in clinical, radiologic, and histopathologic findings for EP/BNCT and low-grade chordoma, the distinction between these entities may be arbitrary. Until histopathologic analysis is completed, radiologically characteristic lesions in typical locations are best described as “benign-appearing notochordal lesions,” to avoid ascribing expected behavior before repeat imaging. Repeat imaging, first after 6 months, then with larger intervals (doubling each time) as stability is established, is a more clinically relevant method for evaluating the malignant potential of these lesions and will allow more nuanced prognostic discussions with patients. Although many of these tumors will never require surgical intervention, a patient-centered approach can be used that factors in patient age, the presence of attributable symptoms, rate of tumor growth, changes in imaging characteristics, and patient preferences (Table). The potential for malignant transformation of benign lesions should be considered, and continued imaging surveillance should be pursued even in cases that do not demonstrate appreciable growth or development of symptoms. More research is needed to establish evidence-based criteria for surgical intervention.
Considerations for excisional biopsy of benign-appearing notochordal lesions
CONCLUSIONS
The classic dichotomy of a benign notochordal remnant (ecchordosis physaliphora) and a malignant notochordal tumor (chordoma) is outdated. Notochordal lesions fall on a spectrum of disease from completely benign to aggressively malignant. Although aggressive disease can be identified radiologically, low-grade malignancies cannot be reliably distinguished from benign disease, and even benign disease has the occasional potential for malignant transformation. Repeat imaging, beginning at a 6-month interval, is recommended even for lesions that appear completely benign on MR imaging. The term benign-appearing notochordal lesion is a more accurate descriptive term that does not make undue assumptions about the clinical behavior of incidentally discovered lesions in the central clivus and skull base.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received January 9, 2023.
- Accepted after revision June 8, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}