
Abstract
BACKGROUND AND PURPOSE: The inaugural “Spinal CSF Leak: Bridging the Gap” Conference was organized to address the complexities of diagnosing and treating spinal CSF leaks. This event aimed to converge the perspectives of clinicians, researchers, and patients with a patient-centered focus to explore the intricacies of spinal CSF leaks across 3 main domains: diagnosis, treatment, and aftercare.
MATERIALS AND METHODS: Physician and patient speakers were invited to discuss the varied clinical presentations and diagnostic challenges of spinal CSF leaks, which often lead to misdiagnosis or delayed treatment. Patient narratives were interwoven with discussions on advanced radiologic techniques and clinical assessments. Treatment-focused sessions highlighted patient experiences with various therapeutic options, including epidural blood patches, surgical interventions, and percutaneous and endovascular therapies. The intricacies of immediate and long-term postprocedural management were explored.
RESULTS: Key outcomes from the conference included the recognition of the need for increased access to specialized CSF leak care for patients and heightened awareness among health care providers, especially for atypical symptoms and presentations. Discussions underscored the variability in individual treatment responses and the necessity for personalized diagnostic and treatment algorithms. Postprocedural challenges such as managing incomplete symptom relief and rebound intracranial hypertension were also addressed, emphasizing the need for effective patient monitoring and follow-up care infrastructures.
CONCLUSIONS: The conference highlighted the need for adaptable diagnostic protocols, collaborative multidisciplinary care, and enhanced patient support. These elements are vital for improving the recognition, diagnosis, and management of spinal CSF leaks, thereby optimizing patient outcomes and quality of life. The event established a foundation for future advancements in spinal CSF leak management, advocating for a patient-centered model that harmonizes procedural expertise with an in-depth understanding of patient experiences.
ABBREVIATIONS:
- CTD
- connective tissue disorders
- CTM
- CT myelography
- CVF
- CSF-venous fistula
- DSM
- digital subtraction myelography
- PDPH
- post-dural puncture headache
- POTS
- postural orthostatic tachycardia syndrome
- RIH
- rebound intracranial hypertension
- SCSFL
- spinal CSF leak
The inaugural “Spinal CSF Leak: Bridging the Gap” Conference, held on November 11, 2023, highlighted collective insights shared by a diverse cohort of clinicians, researchers and, crucially, patients. The goal of this conference was to foster a nuanced, patient-centered understanding of the diagnosis and treatment of spinal CSF leak (SCSFL), a condition that has historically posed profound challenges to both patients and physicians.
SCSFL may be spontaneous, resulting in the syndrome of spontaneous intracranial hypotension, or may be caused by an intentional or unintentional dural puncture, producing acute or chronic post-dural puncture headache (PDPH). SCSFL frequently present a diagnostic conundrum due to ambiguous clinical presentations combined with a relative lack of recognition in the medical community. Many patients with SCSFL are initially misdiagnosed, leading to delays in care, inappropriate treatments, and degrading patient trust in the medical system.1⇓-3 This mismanagement is superimposed on a condition which, when left untreated, can cause immense disability and suffering.4
This conference was designed not only to feature physician experts in the field but to provide a platform for a diverse group of patients to synthesize their experiences in a didactic format and highlight their journey throughout SCSFL care. A variety of perspectives were presented, converging on a proposed framework that balanced cutting-edge diagnostic and treatment techniques with a patient-centered approach. The conference was divided into 3 sessions: diagnosis, treatment, and aftercare.
MATERIALS AND METHODS
Content from lectures at the conference was reviewed and synthesized with current literature to summarize the major themes pertaining to SCSFL care. Patient lectures and video compilations were recorded and transcribed using a large language model (GPT-4) to convert patient narratives into written form. Recommendations were abstracted from the content of the conference and summarized by the authors.
Diagnosis
The Patient Perspective.
The conference opened with a narrative shared by a patient detailing their decade-long struggle with undiagnosed symptoms of a SCSFL. At 11 years of age, the patient had a fall, which led to a diagnosis of postconcussion headaches, and at 15 years of age underwent corrective surgery for scoliosis. The patient developed worsening in orthostatic symptoms postoperatively, initially attributed to a postconcussion syndrome. It was not until a potential chronic surgical leak was identified by a subspecialist years later that the patient received epidural patching and symptom relief. This patient’s journey highlights the potentially disabling delay in diagnosis commonly experienced by patients with SCSFL. This narrative emphasized the need for heightened awareness of SCSFL among health care providers for younger demographics, in whom the condition is often unexpected and the diagnosis challenging.
Another perspective was shared by a patient with a PhD and professional background in trauma therapy who had a CSF-venous fistula (CVF). Given this unique position, he shed light on the psychological challenges accompanying undiagnosed or misdiagnosed SCSFL, including the emotional toll and mental health implications of living with chronic, unexplained symptoms. Additionally, he suggested techniques for patients to process trauma associated with a SCSFL diagnosis and treatment to reclaim their health autonomy. This narrative advocated an enhanced, empathetic, and comprehensive approach by health care professionals to address the mental health aspects inherent in the patient journey of SCSFL. Specifically, it stressed the importance of the patient-provider relationship in SCSFL care, extending beyond diagnostic and therapeutic procedures. This aspect is particularly important for procedural neuroradiologists, who often perform procedures in isolation and without a framework for continuity of care.
Clinical Challenges
The complexity of diagnosing SCSFL hinges on the wide spectrum of clinical presentations that often lead to misdiagnosis or delayed treatment (Table). The classic clinical presentation of SCSFL is characterized by an orthostatic headache. The headaches themselves can have nuanced features, which should be addressed via a thorough history. Patients also frequently describe acephalgic symptoms including fatigue, tinnitus, ear fullness, light sensitivity, cognitive dysfunction. and neck pain, and often experience worsening of symptoms during the day.5 Patients with acephalgic symptomatology may be particularly susceptible to misdiagnosis and inappropriately dismissed if a classic orthostatic headache is not described.
| Overlap with SCSFL | Key Differences from SCSFL | |
|---|---|---|
| Chronic migraine | Headache as primary clinical presentation |
|
| Postconcussion headache | Both can be precipitated by trauma |
|
| Postural orthostatic tachycardia syndrome | Orthostatic symptoms |
|
| Chiari I malformation | Cerebellar tonsillar ectopia may be present in both conditions |
|
Differential diagnoses in patients presenting with SCSFL
Patients with SCSFL are frequently misdiagnosed with migraine. Chronic migraine is characterized by headaches on >15 days per month for at least 3 months, with at least one-half of these days demonstrating unilateral throbbing pain, physical activity exacerbation, light and noise sensitivity, or nausea.6 Chronic migraine evolves across time with increased frequency of attacks, while SCSFL symptoms often begin suddenly. Cephalgia in SCSFL is typically orthostatic and worsens as the day progresses, while migraine attacks often occur in the morning. Patients may also be frequently misdiagnosed with postconcussion headaches, because some SCSFL leaks are precipitated by trauma.7 However, the postconcussion syndrome more commonly presents with migraine-like, nonorthostatic headaches and cognitive issues.8
Postural orthostatic tachycardia syndrome (POTS) is a condition predominantly affecting young women and is characterized by an abnormal heart rate increase on standing.6 Many patients with POTS also have headache; however, most POTS headaches are nonorthostatic and resemble migraine, while orthostatic headache and neck stiffness are more common in SCSFL.9
SCSFL can be radiographically misdiagnosed as Chiari I morphology due to potential presence of cerebellar tonsillar ectopia in both conditions. Scrutiny of the posterior fossa structures on brain MR imaging aids in the reliable differentiation of these 2 entities.2,10 While patients with both SCSFL and Chiari I can present with occipital headaches and neck pain, patients with Chiari I do not commonly have orthostatic headaches but may experience lightheadedness or fainting.11
Connective tissue disorders (CTD) are common in patients with SCSFL.12 Patients with CTD often exhibit chronic, debilitating symptoms that are challenging to treat due to multifactorial etiologies. For instance, mast cell dysfunction has been linked to CTD, causing disordered immune/inflammatory responses.13 Patients may undergo evaluation for Ehler Danlos syndrome, small fiber neuropathy, and/or craniocervical instability, and pinpointing a specific diagnosis is often difficult. In designing diagnostic and treatment strategies for such patients, the interplay of these various disorders must be considered.
It is the synthesis of both clinical and radiographic clues that leads to diagnostic optimization for patients with SCSFL. Discussing patients in a formal, multidisciplinary conference incorporating expertise from neurologists, neurosurgeons, and neuroradiologists can be critically important in this regard.14
Radiologic Challenges
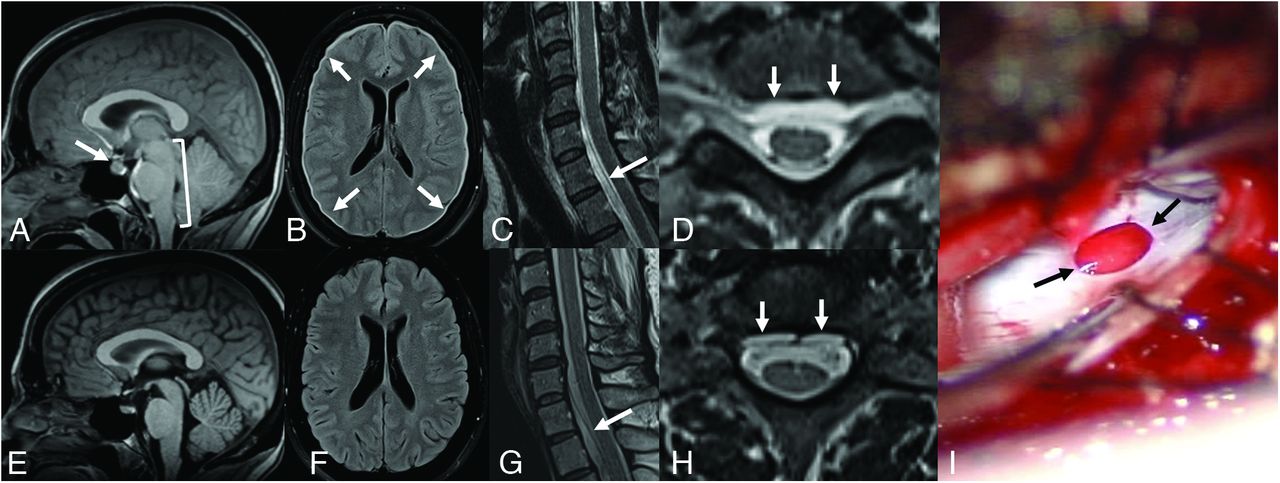
In SCSFL, brain MR imaging classically demonstrates diffuse pachymeningeal enhancement, subdural collections, venous/pituitary engorgement, and/or sagging of the posterior fossa structures. However, a proportion of brain MR imaging studies will be interpreted as having normal findings in patients with proved SCSFL.15 Some patients experience normalization of brain MR imaging findings with time, despite persistent symptoms and a localizable dural defect or CVF (Fig 1).16 It is, therefore, crucial to obtain all prior imaging for patients presenting with symptoms of SCSFL, particularly imaging available close to the onset of symptoms. Some patients may have their examinations incorrectly interpreted as having normal findings, particularly when these changes are subtle (Fig 2).17 Findings of others are truly normal even with careful scrutinization for subtle MR imaging findings. This outcome is particularly true of patients with PDPH, in whom findings of brain imaging are frequently normal, particularly in the chronic period despite known dural puncture and new headache symptoms.18,19

Normalization of MR imaging findings across time despite persistent spinal CSF leaks. A, Sagittal T1 noncontrast MR imaging in 2018 demonstrates sagging of posterior fossa structures (bracket), engorgement of the pituitary gland, and narrowed suprasellar distance (arrow). B, Axial FLAIR MR imaging in 2018 demonstrates a diffuse, thin subdural collection (arrows). Sagittal (C) and axial (D) T2 MR imaging of the cervical spine in 2018 shows a cervicothoracic ventral epidural fluid collection (arrows). The patient underwent a dorsal nontargeted epidural blood patch in 2018 with partial relief of symptoms. E, Sagittal T1 noncontrast MR imaging in 2023 demonstrates resolution of brain sag, pituitary engorgement, and narrowing of the suprasellar interval. F, Axial FLAIR MR imaging in 2023 with resolution of the subdural collection. Sagittal (G) and axial (H) T2 MR imaging of the cervical spine in 2023 shows persistence of the cervicothoracic ventral epidural fluid collection. I. Intraoperative photograph later in 2023, with a ventral dural defect identified at T2–T3 (arrows). After repair, the patient had substantial symptom improvement, with the Headache Impact Test score improving from 68 to 48 (Headache Impact Test: range, 36–78).

Brain MR imaging findings incorrectly reported as normal in a patient with spontaneous intracranial hypotension. A, Sagittal T1 postcontrast MR imaging demonstrates mild narrowing of the suprasellar (1 mm, dotted arrow), mamillopontine (4.8 mm, dashed arrow), and prepontine (3 mm, solid arrow) distances. B, No pachymeningeal thickening or subdural collection on axial T1 postcontrast MR imaging. C, Left-lateral decubitus dynamic CTM detected a CVF arising from the left T7–8 neural foramen (arrow).
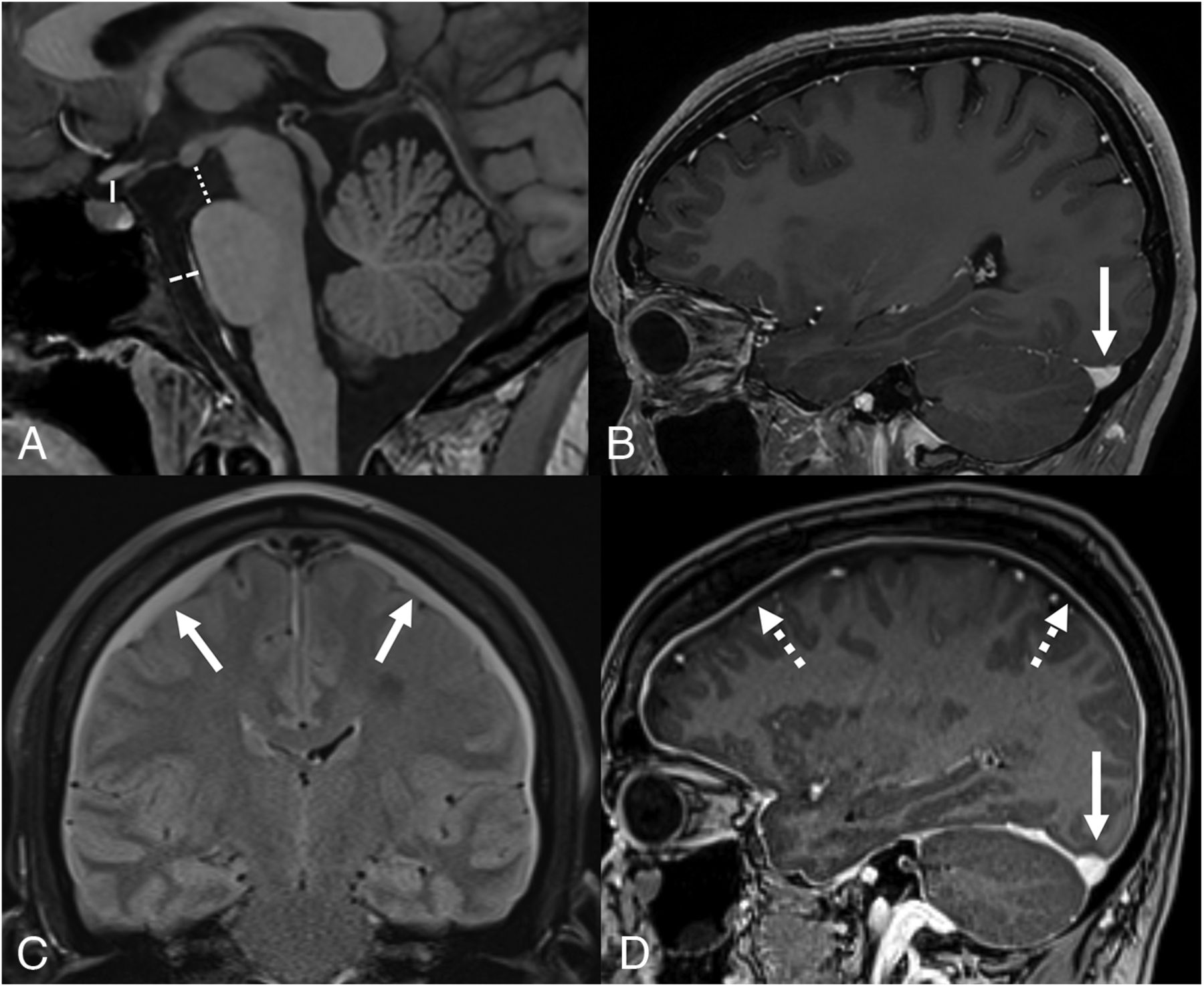
The Bern Score is a probabilistic scoring system reflecting the likelihood of localizing a leak or CVF on myelography (Fig 3).20⇓-22 It is derived from the sum of points ascribed to certain observations on brain MR imaging and can help radiologists avoid inappropriately characterizing an abnormal examination having abnormal findings as having normal findings.17 However, a recent study by Houk et al23 demonstrated that the Bern Score does not correlate with clinical headache severity. This finding challenges the hypothesis that symptoms in SCSFL are directly related to sagging/traction on meningeal layers and/or venous engorgement. Understanding the specific role of brain MR imaging findings and Bern Score applications and limitations is critical to appropriately triage patients with suspected SCSFL.

The Bern score. A, Sagittal T1 noncontrast MR imaging demonstrating the suprasellar interval (solid line, normal, >4 mm), mamillopontine interval (dotted line, normal, >6.5 mm), and prepontine interval (dashed line, normal, >5 mm). B, Sagittal T1 postcontrast MR imaging illustrates a normal flat appearance of the upward margin of the transverse sinus (arrow). C, Coronal FLAIR MR imaging with bilateral subdural fluid collections (arrows). D, Sagittal T1 postcontrast image demonstrates abnormal venous engorgement evidenced by an abnormal convex upward margin (solid arrow), as well as diffuse pachymeningeal enhancement (dotted arrows). The presence of a narrowed suprasellar interval, venous engorgement, or pachymeningeal enhancement are ascribed 2 points each, while a narrowed mamillopontine interval, prepontine interval, or the presence of subdural collections are ascribed 1 point each. A combined score of ≤2 equates to low probability, a score of 3 or 4 equates to moderate probability, and a score of ≥5 equates to high probability of localizing a CSF leak or venous fistula on subsequent myelography.20
CVFs are not visible on conventional CT myelography (CTM) and thus have long evaded detection, with the first formal description published in 2014.35 Dynamic lateral decubitus CT or fluoroscopic myelography (with or without digital subtraction, digital subtraction myelography [DSM]) producing densely layering contrast along the lateral thecal sac is key to localizing CVF.14 Provocative maneuvers such as resisted inspiration can also enhance fistula conspicuity.24,25 Whether DSM or CTM is performed for CVF localization depends on institutional resources and expertise. Newer CT technology, specifically photon-counting CT, has been shown to increase the sensitivity for small CVFs by using ultra-high-resolution imaging with 0.2-mm slices at lower radiation doses.26
In the case of dural defects or ruptured meningeal diverticula, conventional, nondynamic CTM will confirm the presence of an extradural collection but lacks the temporal resolution for precise leak localization. Furthermore, heavily T2-weighted, noncontrast 3D MR imaging of the spine is noninferior to conventional CTM for the detection of epidural fluid collections.27,28 Thus, conventional CTM is likely of limited utility in the work-up of suspected SCSFL. Additionally, CTM exposes patients to radiation and a dural puncture, risking the development of PDPH.
We recommend that patients with suspected SCSFL undergo contrast-enhanced brain MR imaging and heavily T2-weighted MR imaging of the entire spine before an invasive procedure. The Bern Score should be calculated to assess the potential yield of myelography, and spinal MR imaging should be scrutinized for the presence of any epidural fluid. This work-up strategy maximizes information for procedural planning and patient counseling.12 In patients with a high clinical suspicion of SCSFL but a low Bern score and no spinal epidural fluid, a trial of empiric epidural blood patching is a useful treatment strategy, potentially providing symptom relief while minimizing the risk to the patient.29
Treatment
The Patient Perspective.
The experience of undergoing an epidural blood patch was highlighted in a video montage of patient testimonials. These personal accounts detailed the effects of the procedure, ranging from marked relief to minimal or short-lived symptom improvement. Some patients described intense pain during the procedure, while others noted minimal discomfort. Patients expressed a range of emotions, from gratitude for the relief provided to frustration and disappointment in cases in which symptoms persisted or recurred. Their narratives underscored the complexity and variability of patient responses to this treatment, emphasizing the need for individualized care and the importance of patient-provider communication in managing expectations and outcomes of the procedure.
A family medicine physician who experienced an SCSFL shared her unique perspective as both a doctor and patient. In 2020, she developed a sudden-onset severe headache following a cough, which only improved on lying down, leading to suspicion of an SCSFL. Despite her medical background, she was unfamiliar with this condition and, like many patients, had to educate herself. She underwent epidural blood patching, which provided only partial relief. Communication with specialists led to a recommendation for surgery due to a suspected ventral dural defect. However, like many patients with SCSFL, she faced challenges obtaining definitive treatment, requiring approval for an out-of-network referral and interstate travel for the procedure. She ultimately underwent surgical repair. The postoperative period was daunting, marked by the challenge of recovering away from her medical team. The surgery successfully alleviated her headaches; however, returning to work as a physician proved challenging due to persistent back pain, requiring an extended medical leave. More than 2 years postsurgery, she still experiences back pain, a condition she accepts as a trade-off for freedom from debilitating head pain. Her experience underscores the importance of having a support network while undergoing treatment and the reality of living with long-term effects of invasive medical interventions.
Percutaneous and Endovascular Therapies
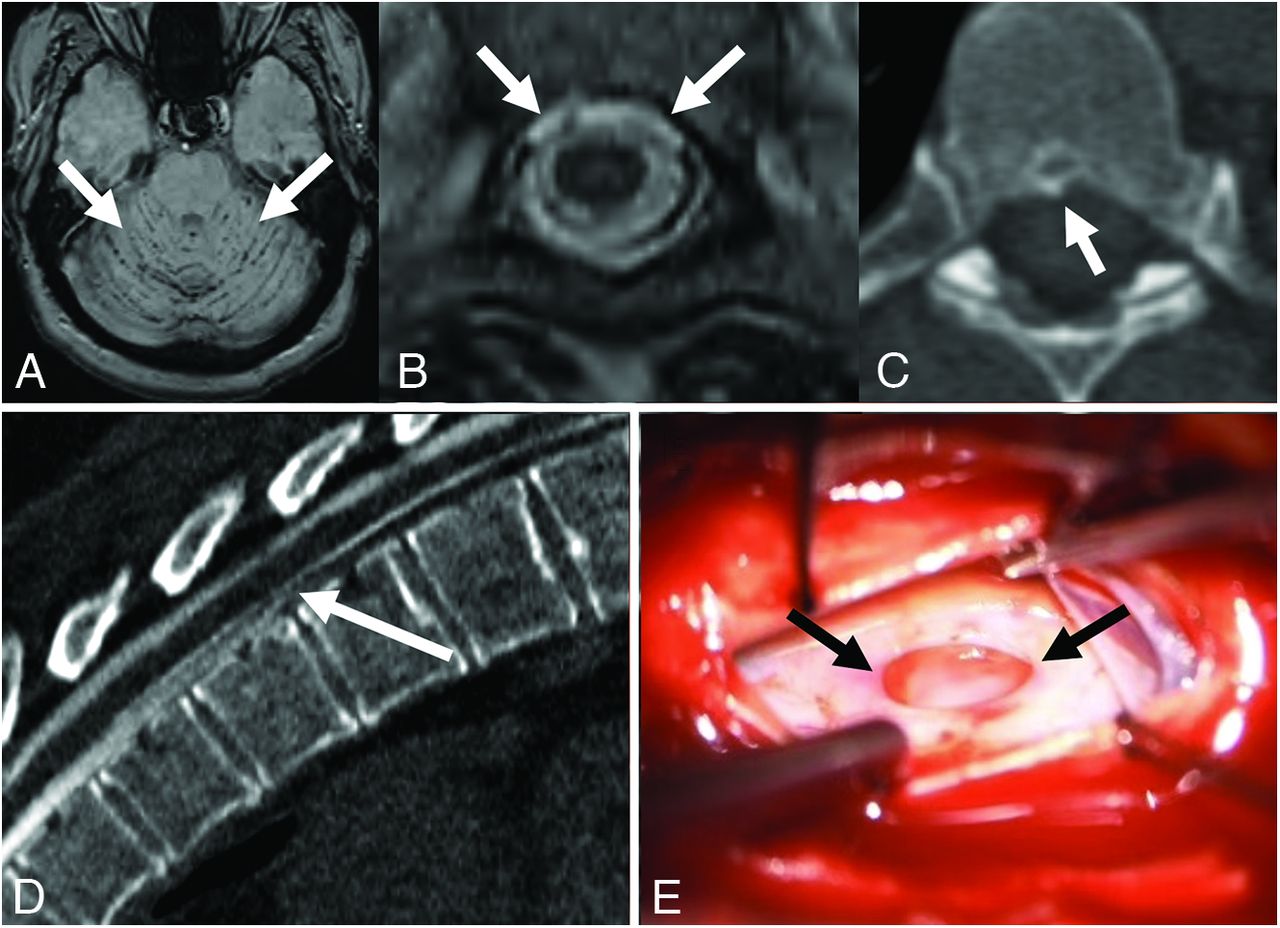
Image-guided percutaneous treatments for SCSFL include image-guided injection of autologous blood and/or fibrin sealant into the epidural space, ideally targeted to the localized dural defect or CVF.30 Patching can close the leak without surgical intervention, particularly when performed near symptom onset. However, as a leak persists into the chronic period, the likelihood that surgery will be required for definitive management increases.31 Thus, prompt recognition of an SCSFL is critical to maximize the success of percutaneous patching. Nontargeted epidural blood patching can be performed using a 2-level thoracolumbar interlaminar approach and ideally injecting at least 20 mL of autologous blood.32,33 Targeted patching is performed when a leak is localized and may be performed with fluoroscopy or CT guidance. When a ventral leak is identified, a far-lateral transforaminal approach may allow injection directly into the ventral epidural space (Fig 4).34 Guidelines for post-patch management vary widely across institutions, especially regarding the duration of bed rest and activity restrictions. In most centers, patients are advised to lie flat for 24–72 hours postpatch and avoid bending, lifting, or twisting for 6 weeks. Because there is a relative lack of high-quality evidence supporting specific recommendations, guidance provided is often based on expert opinion and physiologic principles.

A 35-year-old man with spontaneous intracranial hypotension who underwent 2 prior nontargeted dorsal epidural blood patches. Sagittal (A) and axial (B) T2-weighted MR imaging sequences demonstrate a ventral epidural fluid collection (arrows). C, Prone dynamic CTM detected contrast extravasating from the subarachnoid into the ventral epidural space at T1-2, consistent with a ventral dural defect (arrow). D, Procedural image from a CT-guided epidural blood and fibrin patch using a 15-cm 22-ga spinal needle via a far-lateral transforaminal approach to target the ventral epidural space adjacent to the defect (arrow). Postinjection sagittal (E) and axial (F) images demonstrate spread of injected blood and fibrin glue along the ventral epidural space (arrows). Posttreatment sagittal T2 (G) and axial 3D T2 fat-saturated MR imaging (H) with resolution of the epidural fluid collection.
Initially described treatment for CVF included surgical ligation of the associated nerve root.35 More recently, both transvenous embolization with liquid embolic agents and percutaneous occlusion with fibrin sealant have been described with success rates of >50%.36,37 At institutions equipped with such treatment modalities, an initial trial of either transvenous embolization or fibrin occlusion may be attempted before surgical ligation. If these procedures fail to relieve the patient’s symptoms, surgical intervention should be considered.
Surgical Treatment
Advancements in radiology, particularly DSM and dynamic CTM, have revolutionized the surgical approach to spinal CSF leaks, enabling a precise identification of the leak type and location and allowing minimally invasive approaches.38 Such techniques can include a hemilaminectomy performed under microscopic visualization using tubular retractors placed through small incisions, thereby reducing postoperative pain.
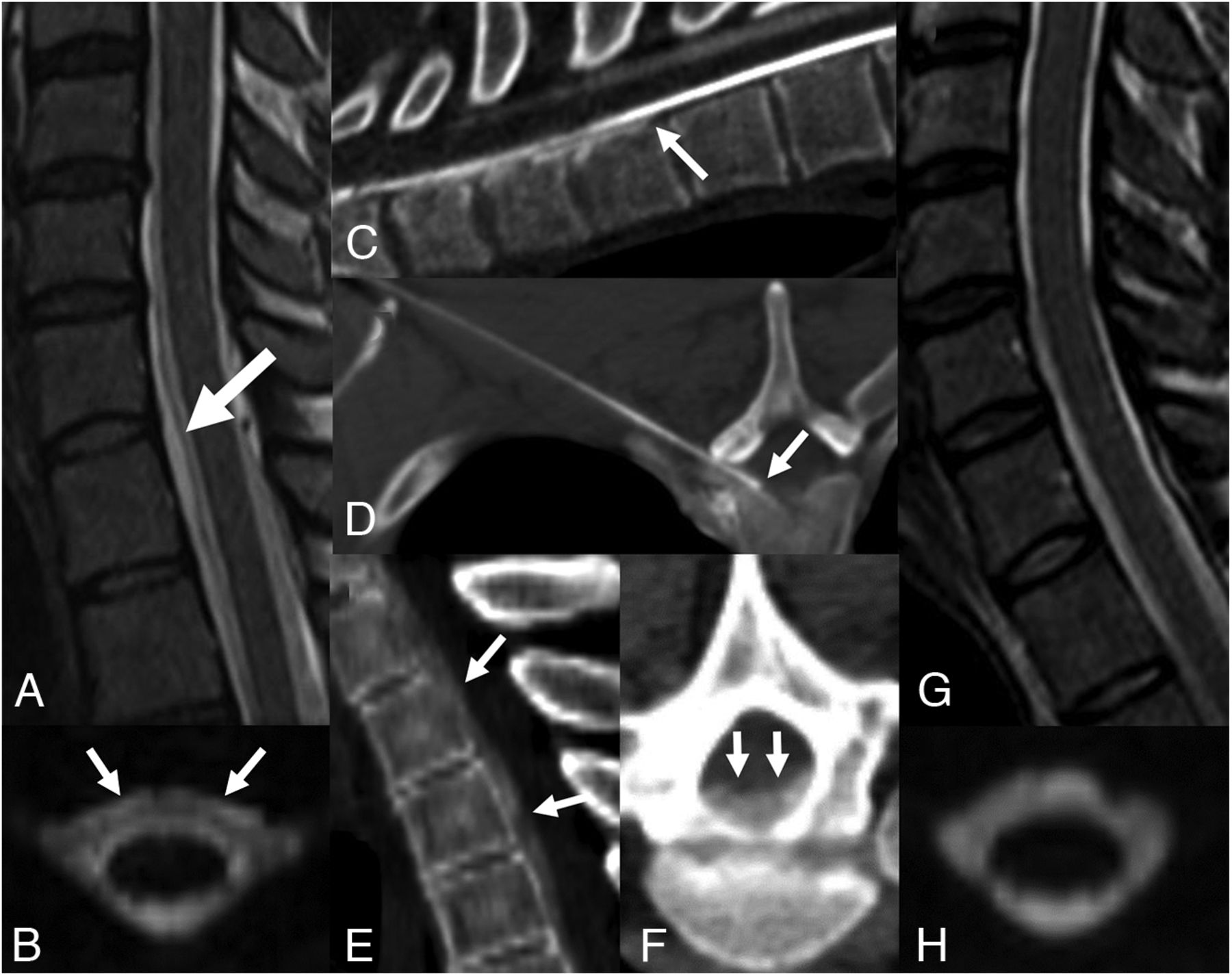
Surgical strategies for repair of ventral dural defects have evolved with time. Rather than requiring an anterior approach with corpectomy and potential thoracotomy, ventral dural defects may be repaired using a transdural, posterior approach, improving patient outcomes and recovery time (Fig 5).39,40 Defects may be closed with direct suturing, collagen patches, or fat/muscle grafts.

A 49-year-old man with a history of spontaneous intracranial hypotension, with persistent symptoms after 3 epidural blood patches. A, Axial SWI with hypointense signal along the cerebellar folia (arrows), consistent with superficial siderosis, a rare complication of chronic CSF leak. B, Axial T2-weighted MR imaging demonstrates a ventral epidural fluid collection (arrows). C, Axial noncontrast CT image shows a small osteophyte (arrows) along the ventral canal at T6–7. D, Prone dynamic CTM demonstrates extravasation of contrast from the subarachnoid space into the ventral epidural space at T6–7 (arrows), consistent with a ventral dural defect. E, Intraoperative photograph during repair of the ventral dural defect (arrows) at T6–7, accessed via hemilaminectomy, posterior durotomy, and lateral mobilization of the cord after dentate ligament resection .
Iatrogenic leaks can also require surgical intervention. Post-dural puncture pseudomeningoceles, also known as arachnoid “blebs,” have been reported to cause symptoms of SCSFL and can be repaired using minimally invasive surgical approaches.41,42 Treatment of a CVF can include ligation of the fistula alone versus transection of the involved nerve root. The postoperative length of the hospital stay can vary, influenced by the surgical approach and patient-specific factors such as rebound intracranial hypertension (RIH).
A recent study identified substantial gaps in the evidence for the efficacy of epidural patching and surgery in the treatment of SCSFL.43 Thus, there are opportunities for future research in this area, which could be supported by patient registries and multicenter collaborations.
Posttreatment
Patient Perspective: Recovery.
A patient discussed her personal journey navigating the recovery process from a SCSFL. She shared her experience with a difficult-to-localize leak, and the many procedures were required before the leak was durably repaired. She described the challenge of undertaking recovery without locally available comprehensive care. She noted that for many patients who lived for years with SCSFL, recovery becomes an existential experience, questioning the meaning of healing and reckoning with a new reality that, while potentially characterized by meaningful clinical improvement, may look nothing like a prior normal life.
She reported that uncertainty is typical during the recovery process, even after successful treatment. Some techniques used to cope with her evolving posttreatment state included tracking symptoms, which helped her take a long view of ongoing severity or resolution, and using talk therapy to process the trauma of living with a SCSFL for so many years.
As noted in her talk, current quaternary referral programs are unable to provide sustained, holistic, comprehensive care to address not only diagnosis and treatment but the recovery process as well. She concluded with a call to action for those in the medical community to consider that although a leak may be closed, it does not mean that the patient’s symptoms have been fully addressed.
Patient Perspective When Treatments Fail: Living with a Leak
Another patient shared her experience with a chronic SCSFL in a presentation focused on acceptance and adaptation, highlighting practical tools and home modifications that have aided in managing daily life. Her journey began with a lumbar puncture performed with an 18-ga cutting needle, leading to a chronic PDPH that significantly impacted her daily activities. After undergoing several rounds of epidural patching, she experienced temporary relief before relapsing. She emphasized the challenges of living with an invisible illness, the emotional toll of acceptance, and the importance of therapy in coping with the condition. She described her fluctuating “uptime,” the duration she could spend upright, and how it shaped her living situation and reliance on family and friends.
She detailed various assistive devices and modifications in her home, including a spill-proof cup for drinking while lying down, a tool for picking up items, comfortable pillows for sleep support, and accessible kitchen and bathroom equipment. She stressed the importance of creating a living environment tailored to the unique needs of individuals with SCSFL. This presentation offered a glimpse into the possibilities of independent living for those affected by long-term SCSFL, while simultaneously providing physicians a firsthand look at the modifications and adaptations required for daily living when available treatment options are inadequate.
RIH
Because treatment of SCSFLs can alter CSF homeostasis, RIH occurs in some cases. The symptoms of RIH include headaches different in character from the original SCSFL headache, often described as frontally located and worse when lying down rather than standing; patients may also experience symptoms of visual disturbances, nausea, and pulsatile tinnitus.44 The morphology and caliber of the transverse venous sinuses, including unilateral hypoplasia and/or stenosis, have been linked to the development of RIH, suggesting a link between venous and CSF dynamics underpinning patient symptomatology.45
The diagnosis of RIH involves clinical assessment and sometimes imaging studies to rule out other causes of increased intracranial pressure. Papilledema may or may not be present and can appear before symptoms occur. In some cases, patients may have had untreated idiopathic intracranial hypertension resulting in eventual dural dehiscence and subsequent SCSFL.46 These patients can experience marked intracranial hypertension after leak repair. Management can be challenging and typically focuses on symptom relief while allowing gradual CSF pressure homeostasis. Treatment options include medication to reduce production of CSF or relieve pain, and in severe cases, CSF diversion may be necessary. RIH can present acutely in the immediate posttreatment period or be delayed.47 The course of RIH varies, with some patients experiencing a resolution of symptoms with time, while others may require ongoing management. It is important for clinicians to monitor patients closely after SCSFL treatment to identify and manage RIH promptly. Critically, a clinical follow-up infrastructure is needed to optimize symptomatic management for patients in the acute and chronic posttreatment period.
Final Patient Presentation: What Doctors Should Know
The concluding patient talk of the day was a montage of personal experiences and insights from individuals living with SCSFL, detailing struggles with a debilitating condition affecting their daily lives, ambitions, and relationships. The speakers discussed the isolating nature of SCSFL and the need for self-advocacy when pursuing treatment. Some patients expressed the disappointment of having normal imaging findings despite severe symptoms and the relief experienced when procedures confirmed a leak. Above all, they spoke to doctors directly, noting that patients suffer more when providers are unable or unwilling to listen to them and urging physicians to believe their patients.
DISCUSSION
While the understanding of optimal diagnostic strategies and treatments for SCSFL has rapidly increased in the past several years, these techniques are limited to a few institutions, leaving many patients underserved. Additionally, these advances are not stand-alone solutions. Patient experiences offer key clinical insights instrumental in refining diagnostic acumen, which is of particular value to the procedurally inclined neuroradiologist. Neuroradiologists are uniquely situated to advocate for the patient with SCSFL because they may be the first to suggest the condition on the basis of imaging and often have procedural skills required to localize and treat the leak. We advocate a patient-centered model, in which these skills are combined with a deeper, nuanced understanding of clinical presentations in the pre- and posttreatment period.
Discussions at the Bridging the Gap Conference illuminated several key topics for future focus. One such area is the need for a standardized-yet-flexible diagnostic protocol. Variability in clinical presentations and often-subtle radiographic findings necessitate a protocol adaptable to the nuances of individual cases. This process should integrate the latest radiologic techniques with thorough clinical assessment, incorporating patient history as a critical component in the diagnostic process. Specifically, key historical features including any prior intended or unintended dural puncture, how and when symptoms started, and the nature of the symptoms should be ascertained.
Another focal point of the conference was the need for collaborative, multidisciplinary care teams. Such teams, composed of neuroradiologists, neurologists, headache/pain specialists, neurosurgeons, and other health care professionals, are essential for providing comprehensive care that addresses all facets of SCSFL diagnosis, treatment, and recovery. The value of this approach was evident through shared patient narratives in which multidisciplinary teams were often critical to achieving a correct diagnosis and effective treatment plan. Moreover, these teams can serve as a platform for ongoing education and awareness-building within the medical community, further improving the recognition and understanding of SCSFL.
The conference also highlighted the importance of patient support and advocacy. Patients’ narratives and questions revealed common themes of physical, emotional, and psychological distress, often exacerbated by the struggle for diagnosis and effective treatment. This outcome underscores the need for health care providers to adopt a holistic approach, going beyond addressing physical symptoms in isolation. Providing emotional and psychological support, ensuring clear and empathetic communication, and fostering patient empowerment and education are key to improving the overall quality of life for individuals with SCSFL. Additionally, strengthening informed patient support networks and advocacy groups can provide crucial resources and a sense of community for those affected by this condition.
Attendees of the conference reported high levels of satisfaction with the content. A postconference survey was administered to patient attendees who were asked to rate their level of satisfaction with the content on a 5-point Likert Scale: 63% of responders reported being “very satisfied” with the content, while the remaining 36% reported being “satisfied.” A CME evaluation form administered to physician attendees showed similar positive feedback, with 90.9% of physicians stating they would change the way they practice because of attending the conference.
The conference is planned to recur annually. A principal goal for the conference in the coming years includes the advocacy of patient-centered research through incorporation of a peer-reviewed scientific abstract-submission process. As the scope of the conference grows, we aim to incorporate additional institutions and more varied health care specialties/perspectives to increase both the breadth and depth of discussion surrounding optimal care of patients with SCSFL.
CONCLUSIONS
The Bridging the Gap Conference provided not only a comprehensive overview of the current state of SCSFL diagnosis and treatment but also set the stage for future advancements in this field. The ideal forward-focal points in SCSFL care include developing adaptable diagnostic protocols, fostering multidisciplinary care teams, and enhancing patient support and advocacy. These steps are essential for bridging the existing gaps in the understanding and management of spinal CSF leaks, ultimately leading to improved patient outcomes and quality of life.
APPENDIX
The “Spinal CSF Leak: Bridging the Gap” Study Group comprises: Nick Stevens, Deborah Friedman, John Reiman, Jessica Houk, Jill Rau, Ian R. Carroll, Wouter Schievink, Claudia Perez Sandhu, Terri Baker, Lalani Carlton Jones, Prem Subramanian, Ilene Ruhoy, Jodi Ettenberg, Danielle Wilhour.
Footnotes
Financial support for this conference was provided by the Spinal CSF Leak Foundation and the University of Colorado Departments of Neuroradiology, Neurosurgery, and Neurology.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received November 27, 2023.
- Accepted after revision December 18, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}