
Abstract
SUMMARY: Clear cell carcinoma of the base of the tongue is a rare minor salivary gland neoplasm, and to our knowledge, the MR imaging appearance of this entity has not been described. We present the MR imaging findings in such a case and review the differential diagnosis for tongue base masses in an adult.
Clear cell carcinoma (CCC) (also known as clear cell adenocarcinoma and hyalinizing clear cell carcinoma[HCCC]) is one of the rarest tumors of the minor salivary glands and infrequently occurs at the base of the tongue.1 It is classified as a low-grade epithelial neoplasm and has a female predominance. To our knowledge, the MR imaging appearance of this entity has not been described. We report a case of a pathologically proved CCC of the base of the tongue in a patient presenting with progressive dysphagia.
Case Report
A 47-year-old woman presented to her primary care physician with a 5-month history of episodic swallowing difficulties, a sore throat, and a single episode of hemoptysis.
On initial presentation, physical examination of the patient’s head, eye, ear, nose, and throat revealed a firm mass lesion at the right base of the tongue. Hematologic and serum chemical laboratory indices were within normal limits with the exception of mild anemia. The patient was referred to an otolaryngologist for further evaluation and for an MR imaging examination of the neck and oral cavity.
An MR imaging examination of the neck was performed with and without intravenous gadolinium contrast material (Fig 1A, -B). This revealed an approximately 1.6 (anteroposterior) × 2.6 (craniocaudal) × 2.3 cm (transverse) diffusely enhancing pedunculated mass at the base of the tongue with extension into the bilateral valleculae. This mass was fairly well circumscribed, except at its anterior margin with the tongue, and was isointense to the tongue on T1-weighted and hyperintense to the tongue on T2-weighted imaging. Differential diagnostic considerations at the time of imaging included lymphoma, squamous cell carcinoma, and granular cell tumor. There was no significant lymphadenopathy by size criteria.

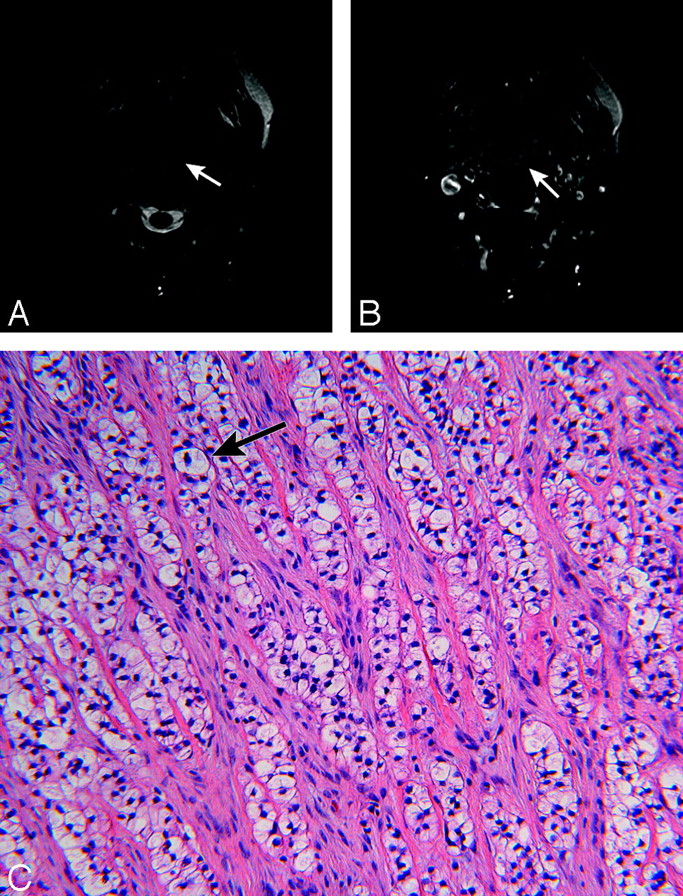
Forty-seven-year-old woman with a mass at the base of the tongue. A, Axial T2-weighted fat-suppressed MR image (TR/TE, 4050/88) shows a well-demarcated hyperintense mass at the base of the tongue (arrow). B, Axial T1-weighted fat-suppressed gadolinium contrast-enhanced MR image (TR/TE, 500/20) shows diffuse enhancement of the mass at the base of the tongue (arrow). C, High-power photomicrograph of the tumor shows infiltrative nests of plump cells with optically clear cytoplasm (arrow) within a hyalinized stroma (hematoxylin-eosin, original magnification ×400).
Twenty-two days after the MR imaging examination, 2 biopsies of this lesion were subsequently performed under direct laryngoscopic visualization. A moderate amount of bleeding occurred during this procedure. The histologic analysis of the biopsy specimens demonstrated some typical features of a pleomorphic adenoma; however, some areas had an infiltrative pattern so that a low-grade polymorphous carcinoma could not be excluded. Hence, complete excision of the lesion was recommended. One month later, the tumor was completely excised with the patient under general endotracheal anesthesia. The patient had an uneventful postoperative course. Surgical specimens were subsequently sent to the Armed Forces Institute of Pathology for analysis.
Gross pathologic examination revealed a 4.4 × 4.0 × 2.0 cm ovoid lesion with a light-pink granular exterior and a cut surface that was homogeneous, glistening, gray-white, and rubbery. Microscopically, the tumor consisted of infiltrative nests of cytologically bland cells within a hyalinized stroma (Fig 1C). Beneath the mucosa, nested cells were smaller with round nuclei. These had a modest amount of eosinophilic cytoplasm, and only sparse clear cells were present. In the deeper nests and within most of the tumor, however, cells were almost exclusively plump with optically clear cytoplasm. There was only minimal nuclear pleomorphism. These deeper nests were arranged in infiltrating cords, as well as nests, within the hyalinized fibrous connective tissue stroma (Fig 1C). Scattered chronic inflammatory cells were also present in the tumor. Immunohistochemically, the tumor cells were positive for cytokeratin, but negative for vimentin, calponin, CD10, epithelial membrane antigen, and smooth-muscle actin. A special stain for mucin was also negative. Final pathologic diagnosis was hyalinizing CCC of minor salivary gland origin.
The patient received no further treatment and returned 8 months after resection for follow-up gadolinium contrast-enhanced MR imaging, which showed no evidence of local recurrence or residual tumor.
Discussion
Most tongue base tumors arise from the mucosa and are squamous cell carcinoma (SCC).2,3 The differential diagnosis for masses of the tongue base includes normal lymphatic tissue, ectopic thyroid tissue, lymphoma, lipoma, hemangioma, schwannoma, granular cell tumors, benign and malignant tumors of minor salivary gland origin, rhabdomyosarcoma, and metastatic disease.3
Salivary gland tumors account for less than 0.5% of all malignancies and approximately 3%–5% of all head and neck cancers. The overall incidence of salivary gland tumors in the western world is 2.5–3.0/100000 per year. More than 50% of salivary gland neoplasms are benign. The soft palate is the most common site for minor salivary gland tumors. Overall, however, most salivary gland tumors originate in the parotid gland. Most tumors that occur in the parotid gland are benign, whereas most tumors that occur in the minor salivary glands are malignant.2,4
The most common minor salivary gland tumors include adenoid cystic carcinoma, mucoepidermoid carcinoma, adenocarcinoma, malignant mixed tumor, acinar cell carcinoma, and pleomorphic adenoma.2 The most common benign major and minor salivary gland tumor is the pleomorphic adenoma. The most common malignant major and minor salivary gland tumor is the mucoepidermoid carcinoma.5 Salivary gland–origin tumors that occur at the tongue base include mucoepidermoid carcinoma, adenocarcinoma, adenoid cystic carcinoma, and CCC.6
CCC is a rare histologic subtype of salivary gland tumor, which is now recognized as a distinct entity.7–9 This entity was first described by Batsakis et al10 in 1980 and then further characterized histologically by Milchgrub et al in 1994 and 20008,9 and Ellis in 1998.11 To date, less than 20 cases have been reported in the literature, and an exact incidence is difficult to ascertain because of inconsistencies in reporting and classification. Among the reported cases, there appears to be a female predominance.12 This entity previously was misclassified as other clear cell–containing tumors, including mucoepidermoid carcinoma, epithelial-myoepithelial carcinoma, and adenocarcinoma not otherwise specified.11,12 The oral cavity is the major site of occurrence, most commonly involving the palate, lips, and buccal mucosa. Rare occurrence in the oropharynx and larynx has been reported.1 CCC is typically a low-grade carcinoma. However, rare aggressive variants, metastases, and recurrences have been reported.1,7,12 Treatment typically involves wide surgical resection with or without lymph node dissection. Radiation therapy is reserved for recurrent lesions or those with lymph node metastases.1,12
Histologically, CCC can be divided into 2 subtypes.1 The first subtype is the biphasic epithelial-myoepithelial carcinoma, which is more commonly associated with the major salivary glands. The second subtype is the monophasic myoepithelial or ductal carcinoma, which is more commonly associated with minor salivary glands. This monophasic subtype is accompanied by cords, nests, and trabeculae of glycogen-rich clear cells and eosinophilic cells surrounded by fibrohyaline stroma, hence the designation HCCC. Prominent mitotic activity is not a noticeable feature of HCCC.
Although the initial work-up for tongue base tumors is typically performed by direct visualization and biopsy, imaging is extremely valuable in defining the extent of tumor growth into the deep and adjacent tissues, as well as metastatic spread to lymph nodes.2 Imaging helps to define the exact extent of the lesion and determine possible extension into adjacent tissues. This information plays an important role in staging and treatment planning, as well as in assessing recurrence. CT and MR imaging are the techniques of choice.2 MR imaging offers some advantages over CT because of its superior tissue characterization and multiplanar capabilities.
In general, low-grade lesions of the tongue base tend to be well demarcated, enhance uniformly, and demonstrate T1 hypointensity and T2 hyperintensity. High-grade lesions tend to have less distinct and infiltrative margins. In addition, high-grade minor salivary gland tumors tend to demonstrate low-to-intermediate signal intensity due to the their high cellularity.2,3
The imaging characteristics of CCC of the tongue base have not been previously described. Our case occurring in a 47-year-old woman demonstrated a well-circumscribed diffusely enhancing T2 hyperintense mass at the base of the tongue. These imaging characteristics are nonspecific and may be seen in other salivary gland lesions, as well as other tongue base lesions such as SCC, lymphoma, and schwannoma. Therefore, when evaluating tongue base lesions with MR imaging or CT, one can consider CCC in the differential diagnosis.
References
- Received June 9, 2005.
- Accepted after revision December 9, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.