
Abstract
BACKGROUND AND PURPOSE: In theory, ionic solutes diffuse more slowly in cartilage than do nonionic solutes. We tested the hypothesis that the contrast ratio between scar and recurrent disk fragment on MR images is greater after IV administration of an ionic rather than a nonionic contrast medium when a clinical dose is used.
METHODS: Twenty patients who had recurrent lumbar disk herniation were enrolled in this study. The enhancement of epidural scar and recurrent disk fragment was measured at 5, 25, 40, and 50 min after IV injection of ionic and nonionic contrast media (0.1 mmol/kg)
RESULTS: The enhancement was consistently and significantly higher for scar than for recurrent disk fragment, although the contrast ratio between scar and recurrent disk fragment decreased between 5 and 50 min after the administration of each contrast medium. No significant difference was shown between ionic and nonionic contrast media in the enhancement of recurrent disk fragment at 5, 25, 40, and 50 min after injection. The contrast ratio between scar and recurrent disk fragment was not a significant difference at 5, 25, and 40 min after administration of both contrast media. At 50 min, the contrast ratio between scar and recurrent disk fragment was 1.32 ± 0.41 with ionic contrast medium and 1.20 ± 0.56 with nonionic contrast medium. The difference was significant.
CONCLUSION: The contrast ratio between scar and recurrent disk fragment is affected by the timing of the imaging. Images obtained immediately after the injection of each contrast medium showed a greater contrast ratio than did delayed images. In addition, with the ionic medium, this difference was greater than with nonionic medium at 5, 25, 40, and 50 min after injection and that difference reached statistical significance at 50 min.
In theory, nonionized solutes diffuse more quickly into cartilage than do ionized solutes. This principle of diffusion explains the greater efficacy of uncharged, nonionizing antibiotics in the treatment of diskitis than charged ionizing antibiotics that penetrate poorly into disk cartilage. Therefore, in principle, paramagnetic contrast media that have a charge should diffuse less readily in cartilage than contrast media lacking a charge.
The diffusion of the ionic and nonionic contrast media into cartilage have been widely studied with isotope techniques (1–5) and MR imaging (6–14). Nonionic paramagnetic contrast media diffuse more rapidly into cartilage and disk than do ionic contrast media (6–7). Diffusion of paramagnetic contrast media into immature disks is also greater than into mature disks (14). Nguyen et al (8) found that the implanted epidural disk fragments showed less enhancement with the ionic medium than with the nonionic medium, and the tissue contrast between disk fragment and scar was greater after the use of ionic rather than nonionic contrast medium. Therefore, we designed a study to test the hypothesis that with human MR imaging, greater enhancement of recurrent disk fragment occurs with nonionic rather than ionic media. We compared the enhancement of scar and recurrent disk fragment in patients undergoing lumbar MR imaging with an ionic and a nonionic medium. To improve the power of the study, the enhancement of the scar and the recurrent disk fragment was measured at four time points after the administration of contrast medium.
Methods
With the approval of the institutional review board, study patients were recruited from consecutive patients referred for contrast-enhanced MR imaging of the lumbar spine because of suspected recurrent lumbar disk herniation. The recurrent lumbar disk herniation was typically defined as disk herniation on the basis of MR findings (15–21) obtained at the same level, regardless of ipsilateral or contralateral herniation, with a pain-free interval >6 months after lumbar disk surgery.
These patients were studied with serial imaging performed on a 1.5-T superconductive imaging unit. T1-weighted (450/16 [TR/TE]) and T2-weighted (3405/150) sagittal view spin-echo images with a section thickness of 3 mm were acquired with a 256 × 256 matrix and a 24-cm field of view. T1-weighted (475/18) and T2-weighted (3900/150) axial view spin-echo images with 4-mm section thickness were acquired with a 256 × 256 matrix and a 16-cm field of view. Contrast-enhanced MR imaging, started immediately after the administration of 0.1 mmol/kg ionic gadopentetate dimeglumine, consisted of a sagittal view fat-saturated T1-weighted sequence (400/12) for accessory evaluation of the presence and localization of the recurrent disk and scar. The imaging matrix was 256 × 256, with a section of thickness of 4 mm. In addition, T1-weighted axial images were obtained 5 min after injection of contrast medium, with the same parameters as were used for the unenhanced axial view images. If the images suggested recurrent disk, the additional axial view T1-weighted MR imaging series was obtained at 25, 40, and 50 min after injection. Two radiologists reviewed the images to verify that a probable recurrent herniated disk was present. They also reviewed the medical records to verify that the clinical signs and symptoms were referable to the probable disk herniation. The patient was then contacted by phone or referred clinician and was offered the opportunity to participate in the research project in which subsequent MR imaging would be performed with a different contrast medium. If the patient accepted, informed consent was obtained and secondary MR imaging was performed with identical technical factors and imaging timing after injection with nonionic gadodiamide (0.1 mmol/kg) instead of ionic gadopentetate dimeglumine. The interval permitted between imaging sessions for this protocol was 3 to 5 days.
Twenty patients entered the pilot study group and comprised seven women and 13 men ranging in age from 35 to 65 years (mean, 46.6 years). The time from previous surgery to imaging study varied from 7 months to 6 years (mean, 2.75 years).
The unenhanced and contrast-enhanced images were evaluated together for the presence of recurrent disk. A diagnosis of disk material was made when aberrant soft tissue produced mass effect contiguous to the parent disk and did not enhance on the early contrast-enhanced images. Early linear or band-like enhancement surrounding irregularities of the peripheral parent disk margin without evidence of mass effect was interpreted as a scar (5–10). After MR imaging, two of the 20 patients underwent surgical re-exploration at the site of abnormality noted on the MR images. The operative findings, including the location and the nature of the abnormal tissue, were consistent with the MR imaging findings.
Data Analysis
The measurement of the recurrent disk and scar was performed by a radiologist who did not know what contrast medium was injected when he measured the signal intensity. Signal intensity in the recurrent disk fragments and scar was measured on the T1-weighted axial view MR images with a region-of-interest cursor and resident software. A region-of-interest cursor was placed within the disk fragment and another one in the enhancing scar tissue surrounding the disk fragment on the 5-min image, and signal intensity was recorded (Fig 1). The same cursor locations were used for the baseline, 25-min, 40-min, and 50-min images, and signal intensity was recorded for each of these time points. The enhancement and contrast ratio were calculated as enhancement = (SIpost − SIpre) / SIpre and contrast ratio = SIscar / SIdisk, where SIpost and SIpre were the signal intensities of the targets at contrast-enhanced and unenhanced statuses, respectively. The SIscar and SIdisk represented the signal intensity of scar and recurrent disk fragment at the same time point of unenhanced or contrast-enhanced status, respectively. Differences in the enhancement and contrast ratio were tested for significance with a repeated measures analysis of variance test. If a significant difference was present, the posterior comparison test was tested by means of Bonferroni t test. P < .05 was considered statistically significant.

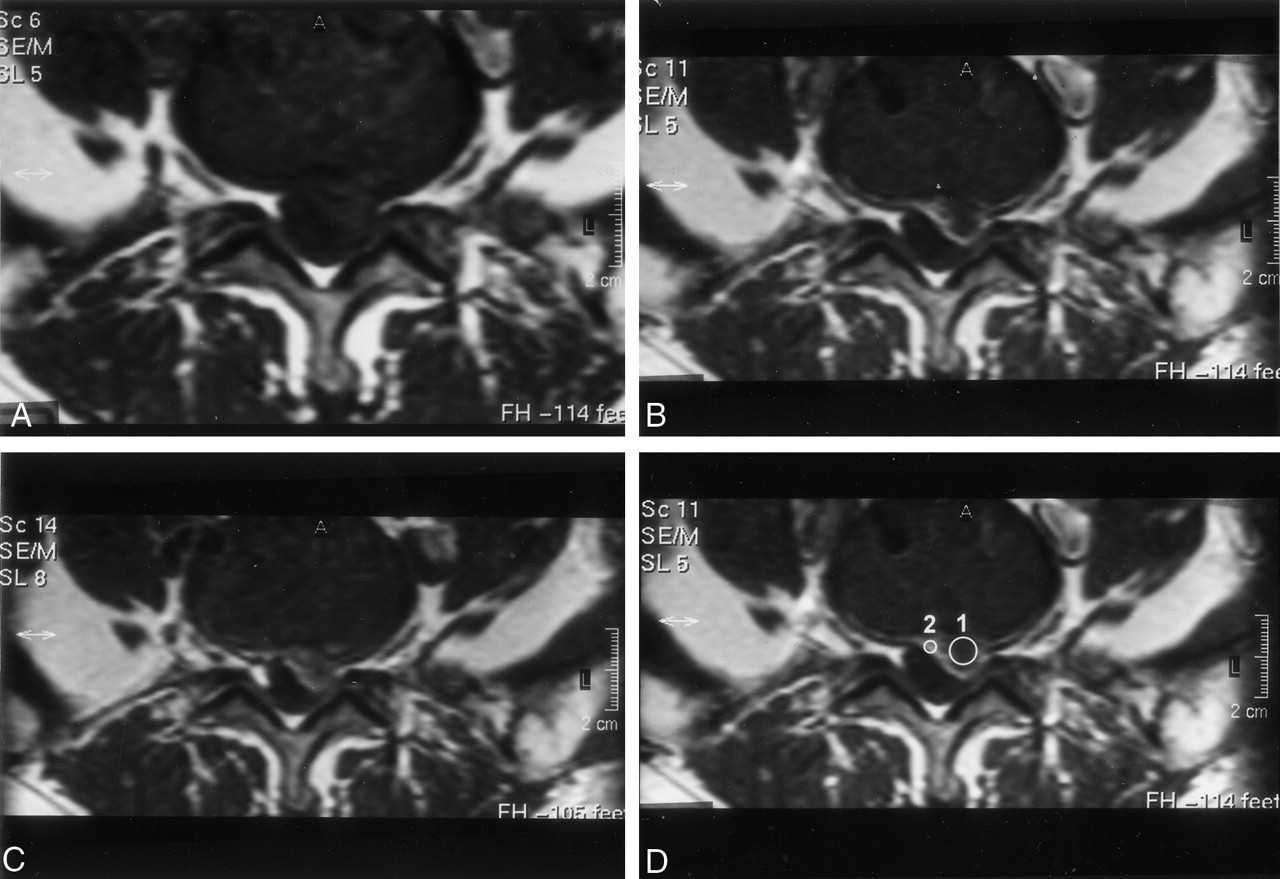
Axial view images of a patient with surgically confirmed recurrent herniated disk.
A, Obtained before the administration of gadopentetate dimeglumine (0.1 mmol/kg).
B, Obtained 5 min after the administration of gadopentetate dimeglumine (0.1 mmol/kg).
C, Obtained 50 min after the administration of gadopentetate dimeglumine (0.1 mmol/kg).
D, Obtained 5 min after the administration of contrast medium. Placement of cursor to measure recurrent disk (1) and scar (2) enhancement. Contrast ratio between scar and recurrent disk fragment is greater at 5 min than at 50 min.
Results
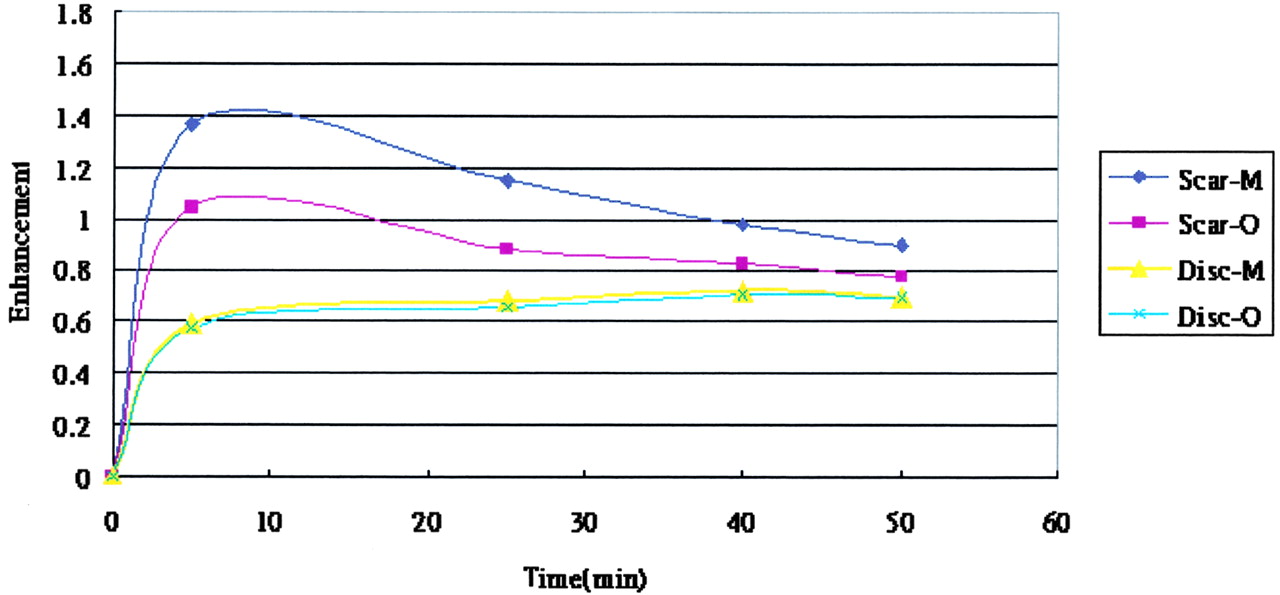
Average enhancement in scar and in recurrent disk fragment after injection of gadopentetate dimeglumine or gadodiamide is summarized in Table 1 and in Figure 2. In the MR imaging studies, the scar and recurrent disk fragment showed different rates of enhancement. The scar showed greater enhancement at 5 min than at 25, 40, and 50 min after injection of either contrast medium, whereas the disk fragment tended to increase in enhancement for 50 min after injection of either contrast medium. Average enhancement of scar was greater than that of recurrent disk fragment for both contrast media at 5, 25, 40, and 50 min (P < .05) (Fig. 3). Average enhancement of scar was less with gadodiamide than with gadopentetate dimeglumine at 5, 25, 40, and 50 min (P < .05). No significant difference was shown in the enhancement of recurrent disk fragment after the administration of either contrast medium at 5, 25, 40, and 50 min (P > .05).

Graph of the average enhancement in scar and in recurrent disk fragment as a function of time after the injection of 0.1 mmol/kg gadopentetate dimeglumine (M) or gadodiamide (O). The scar tended to decrease in enhancement and the recurrent disk fragment tended to increase in enhancement with time.

MR images of a patient with recurrent herniated disk
A, Sagittal view unenhanced T2-weighted MR image.
B, Axial view image obtained before the IV administration of ionic contrast medium.
C, Axial view image obtained 5 min after the IV administration of ionic contrast medium.
D, Axial view image obtained 50 min after the IV administration of ionic contrast medium. Contrast ratio is greater after administration of ionic rather than nonionic contrast media at 50 min (see panel G).
E, Axial view image obtained before the IV administration of nonionic contrast medium.
F, Axial view image obtained 5 min after the IV administration of nonionic contrast medium.
G, Axial view image obtained 50 min after the IV administration of nonionic contrast medium. Contrast ratio is greater after administration of ionic rather than nonionic contrast media at 50 min.
Contrast enhancement in recurrent disk fragment and scar after IV injection of ionic and nonionic contrast media
The contrast ratio between scar and recurrent disk fragment after injection of gadopentetate dimeglumine and gadodiamide is summarized in Table 2 and in Figure 4. The contrast ratio between scar and recurrent disk fragment was greater at 5 min than at 25, 40, and 50 min. No significant difference was shown between gadopentetate dimeglumine and gadodiamide in the contrast ratio between scar and recurrent disk fragment at 5, 25, and 40 min (P > .05). At 50 min, the average contrast ratio was 1.32 ± 0.41 with gadopentetate dimeglumine and 1.20 ± 0.56 with gadodiamide. The difference was significant (P < .05).

Graph of the contrast ratio between scar and recurrent disk fragment as a function of time after injection of 0.1 mmol/kg ionic (M) and nonionic (O) contrast medium. The contrast radio tended to decrease with time (arithmetic mean ± SD, n = 20).
Contrast between the scar and recurrent disk fragment after IV injection of ionic and nonionic contrast media
Discussion
Once a molecule is injected into the blood stream, it encounters the following barriers before reaching the interstitial space: distribution through vascular space, transport across the microvascular wall, and transport through the interstitial space. The intra- and extravascular exchange of fluid and solute molecule in a tissue is determined by two mechanisms: diffusion and convection (22). The factors involved in the molecular transport included the transluminal concentration and pressure gradients, the surface area available for exchange, and three transport parameters: vascular permeability (related to diffusion), hydraulic conductivity (related to hydrostatic convection), and reflection coefficient (related to osmotic convection). These three transport parameters are governed by the number and the width of the endothelial junctions on the vessel wall for a given size of molecule. Once the molecules are transported into the interstitial space, their distribution in the interstitium is again governed by molecular diffusion and possible convection due to pressure heterogeneity within the interstitium (23). For small molecular weight hydrophilic and lipophilic solute molecules, diffusion is the primary mechanism in the cartilage (3). Small molecules such as glucose and sulfate with molecular weight greater than 1000 diffuse readily through the proteoglycans gel (24, 25), which is the major constituent of cartilage, the nucleus pulposus, and inner annulus fibrosis and in diarthrotic joints. Gadopentetate dimeglumine (molecular weight 938) and gadodiamide (molecular weight 547) may diffuse into intervertebral disk and recurrent disk fragment (1–5).
Our results showed that the enhancement measured with gadopentetate dimeglumine and gadodiamide in clinical dose (0.1 mmol/kg) agrees with previously obtained results (8). Both recurrent disk fragment and scar in postoperative spines normally show enhancement on MR images. The enhancement of scar is more than that of disk fragment, and the disk fragment tends to increase in enhancement with time after IV injection of either ionic or nonionic contrast medium. The scar shows apparent enhancement because the blood supply of scar has a capillary fenestrate endothelium, which allows contrast media to enter the interstitial space rapidly (26). Gradual diffusion of contrast medium into the disk fragment probably explains the enhancement mechanism of the disk fragment (6–14). In our study, abrupt change was noted in the enhancement during the first 5 min; gradual increased enhancement was then noted at 25, 40, and 50 min after injection of either ionic or nonionic contrast medium. This confounding effect of a jump in the enhancement during the first 5 min may result from the partial volume effects of scar and recurrent disk in the region-of-interest cursor. In an animal study of mongrel dogs, Nguyen et al (8) showed that the epidural implanted disk fragment tended to gradually increase in signal intensity and showed less enhancement with gadopentetate dimeglumine (0.3 mmol/kg) than with gadoteridol (0.3 mmol/kg). This occurred because the charges on the ionic medium slow its entry into cartilage, which contains a high concentration of fixed negative charges. The difference between the enhancement of implanted disk fragment and that of scar was therefore thought to be greater after the use of ionic rather than nonionic contrast medium. Our study, however, showed no significant difference between ionic and nonionic contrast media in the enhancement of recurrent disk fragment when a clinical dose was used. In addition, the ionic contrast medium showed greater contrast ratio than did the nonionic one at 5, 25, 40, and 50 min after injection and the difference reached statistical significance at 50 min. The difference between the results of our study and those of the study presented by Nguyen et al (8) could be explained by the dose difference of the contrast media. Diffusion is the primary mechanism that determines enhancement of disk fragment. The higher dose may produce higher concentration gradients that increase the permeation of more nonionic contrast media into recurrent disk than that of ionic ones because nonionic solutes diffuse more quickly in disk than do ionic solutes. Our study, however, showed that this phenomenon is less prominent when a clinical dose is used.
The study conducted by Haughton et al (27) showed that contrast between disk fragment and scar tissue was greater after the use of an ionic contrast medium than a nonionic one with clinical dose in eight patients. The sample size was small. In our study, the ionic contrast medium provided relatively greater contrast ratio between the scar and the recurrent disk than did the nonionic one at 5, 25, 40, and 50 min after injection and the difference reached statistical significance at 50 min after injection in 20 patients. The difference between our results and those reported by Haughton et al may be attributable to the relatively small sample size in the other study. Additional studies with larger sample sizes may be necessary for evaluating the difference of ionic and nonionic contrast media-induced differentiation between the scar and recurrent disk in clinical practice. In addition, the study presented by Haughton et al also showed that the enhancement of scar tended to be greater with gadodiamide than with gadopentetate dimeglumine (27). Our study showed contrary results. Gadopentetate dimeglumine and gadodiamide are nonspecific extracellular agents and have similar pharmacokinetics and biodistribution (28). The blood supply of the scar includes capillary fenestrate endothelium that allows contrast media to enter interstitial space rapidly (26). In our experience, some variation exists in the enhancement of the scar. These differing results may be caused by different stages of the scar or the other unknown mechanisms.
One limitation of our study was the relatively small sample size. Another potential source of error was the placement of the region-of-interest cursor. To sample the signal intensity in disk fragment or scar, relatively small region-of-interest cursors are required. Partial volume effects, inhomogeneity of scar and disk tissue, and motion between the baseline and the subsequent two series may have affected the accuracy of enhancement calculations. Imprecision in the timing of the images obtained after injection of contrast medium may have skewed the enhancement calculations; however, these sources of error are likely to produce random rather than systematic errors.
Conclusion
For optimal enhancement in imaging recurrent disk fragments and scar, it is important to choose the most favorable timing. The ionic medium showed greater contrast ratios than did the nonionic medium at 5, 25, 40, and 50 minutes after injection, and the difference reached statistical significance at 50 minutes when a clinical dose was used.
References
- Received March 11, 2003.
- Accepted after revision November 6, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.