
Abstract
Summary: We report initial experience with the use of a new intracranial stent, the Leo microstent in combination with detachable coils in treatment of patients with wide-necked cerebral aneurysms. The Leo stent represents a significant advance in the vascular treatment of intracranial aneurysm with high radial force and an easy delivery system. It is a feasible, secure, and effective system.
The introduction of the first flexible intracranial stent (Neuroform, Boston Scientific/Target, Natick, MA) represented a significant advance in the vascular treatment of intracranial aneurysms that were previously not considered amenable to endovascular therapy (1–3). Recently, the new-generation intracranial stent, the Neuroform 2 Treo, was introduced, which allows better parent vessel scaffolding to prevent coil prolapse and improves “bringing” of endothelial cells across the aneurysm neck (4).
We report the results of our initial experience in using the Leo self-expanding intracranial stent in combination coil embolization, for the treatment of wide-necked intracranial aneurysms.
Description of the Technique
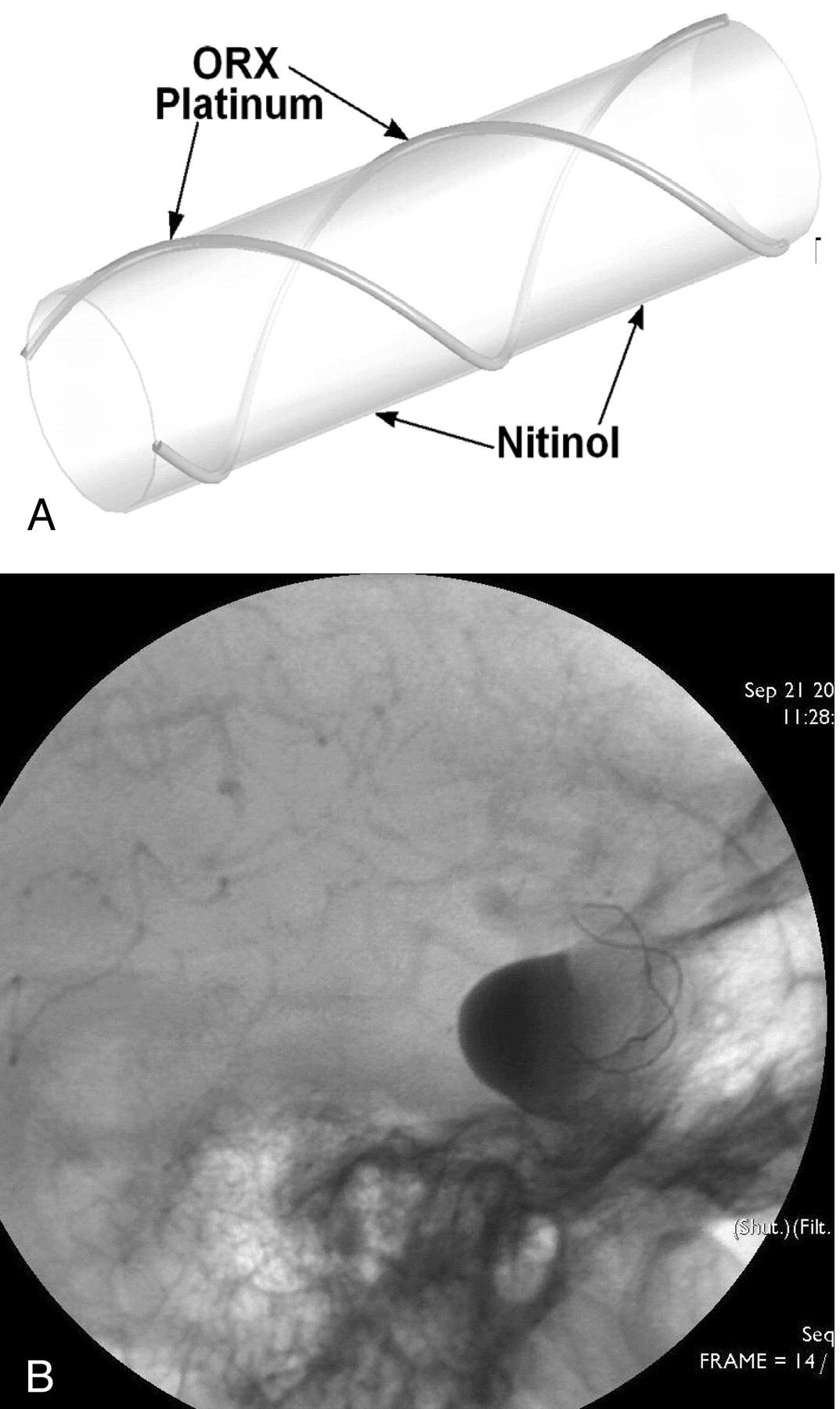
The Leo stent has been designed to combine high radial force and easy delivery. It is made of braided nitinol wires, and there are 2 highly radiopaques wires that ensure visibility of both diameter and length (Fig 1A and -B). The Leo stent has an innovative distal hook that allows for resheathing and repositioning of the stent when as much as 90% deployed (Fig 2A and -B). Leo stents are available in diameters of 2.5–7.5 mm and lengths of 12–50 mm, and coil-delivery microcatheters can access the mesh to fill the aneurysm after placement of the stent. The Leo is delivered through a 3-step process.

A, A twisted nitinol wire body and 2 platinum markers.
B, ORX visualization of both diameter and length.

A and B, The innovative Leo stent distal hook.
1. Stent reference selection.
The artery diameter has to be precisely measured for a secure process. With 2D imaging systems, a dimension reference must be used, such as a coin. The length must be equal to or larger than the aneurysm neck length + arterial diameter.
2. System positioning.
After the placement of a 6F, 90-cm Envoy guiding catheter within the cervical segment, a digital substration roadmap is made, and a microwire (.0014 inch) loaded coaxially inside a Vasco (Balt, Montmorency, France) microcatheter is navigated distal to the aneurysm. The microcatheter is then advanced over the wire until it reaches the space intended for the distal end of the stent. The wire is then removed.
3. Stent Deployment.
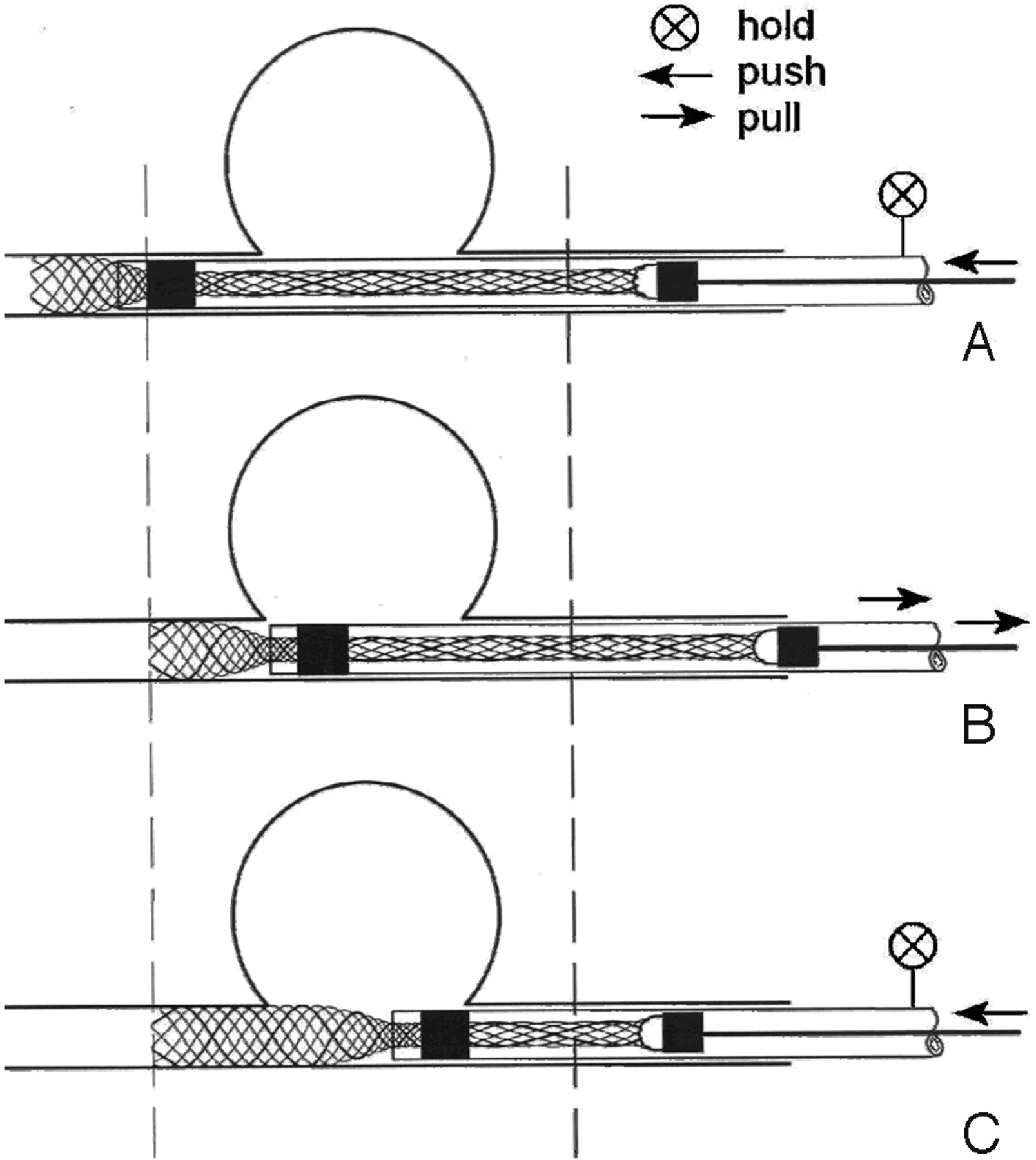
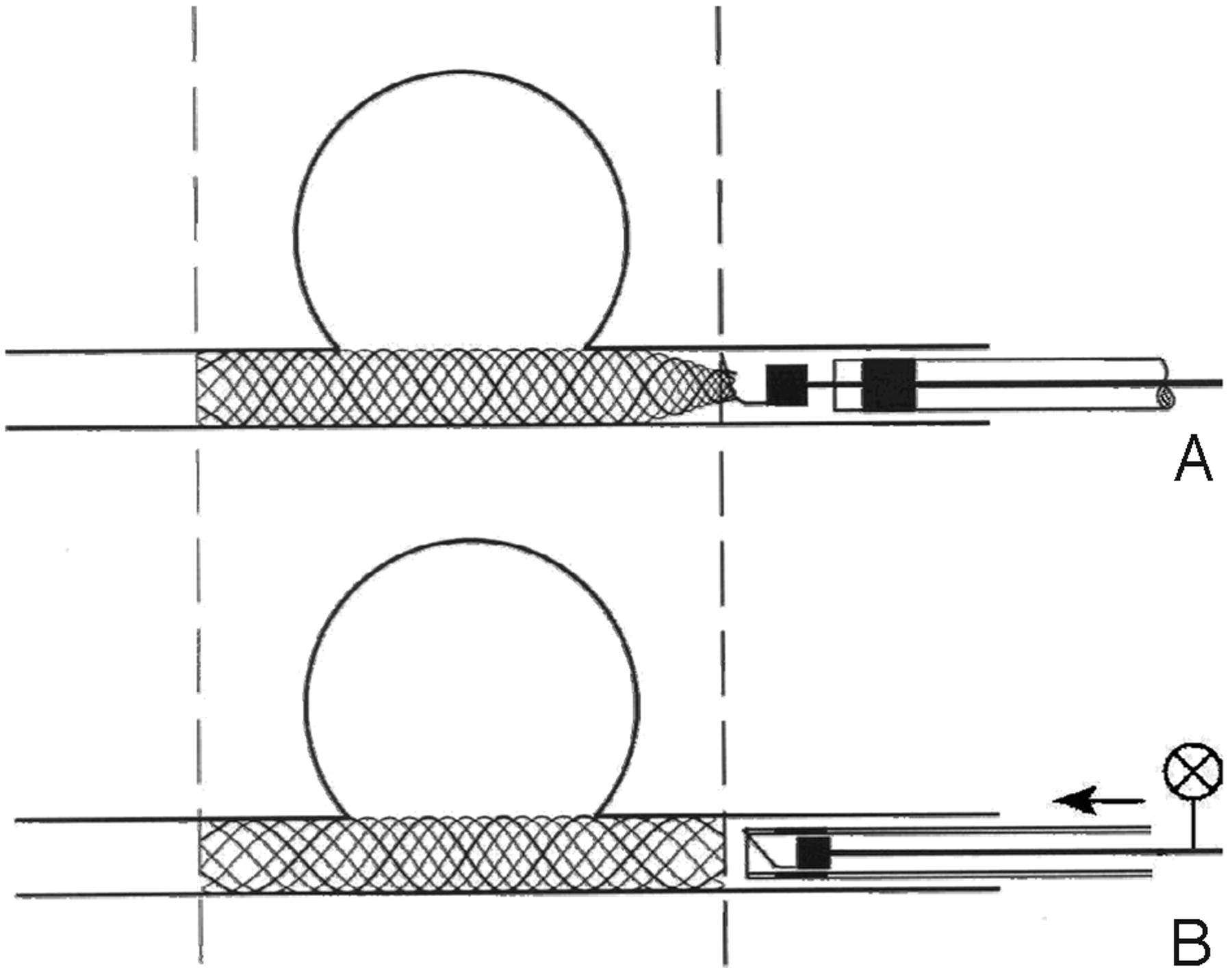
The delivery system is then advanced inside the Vasco microcatheter. One must depress the pusher to make the stent extend beyond 5 mm (Fig 3A). One must then pull the catheter and the stent back until the distal end of the stent is precisely positioned (Fig 3B). Once the distal end of the stent is positioned, its delivery is continued by depressing the pusher. (One must be cautious not to pull the catheter, which is self-retrieving; Fig 3C). The stent can be resheathed and repositioned if needed. Both ends of the stent must remain within a relatively straight section of the artery.

A, Depressing the pusher to make the stent extend approximately 5 mm.
B, Pulling the catheter and the stent back until the distal end of the stent is precisely positioned.
C, Once the distal end of the stent is positioned, it may be delivered by depressing the pusher. The catheter is self-retrieving.
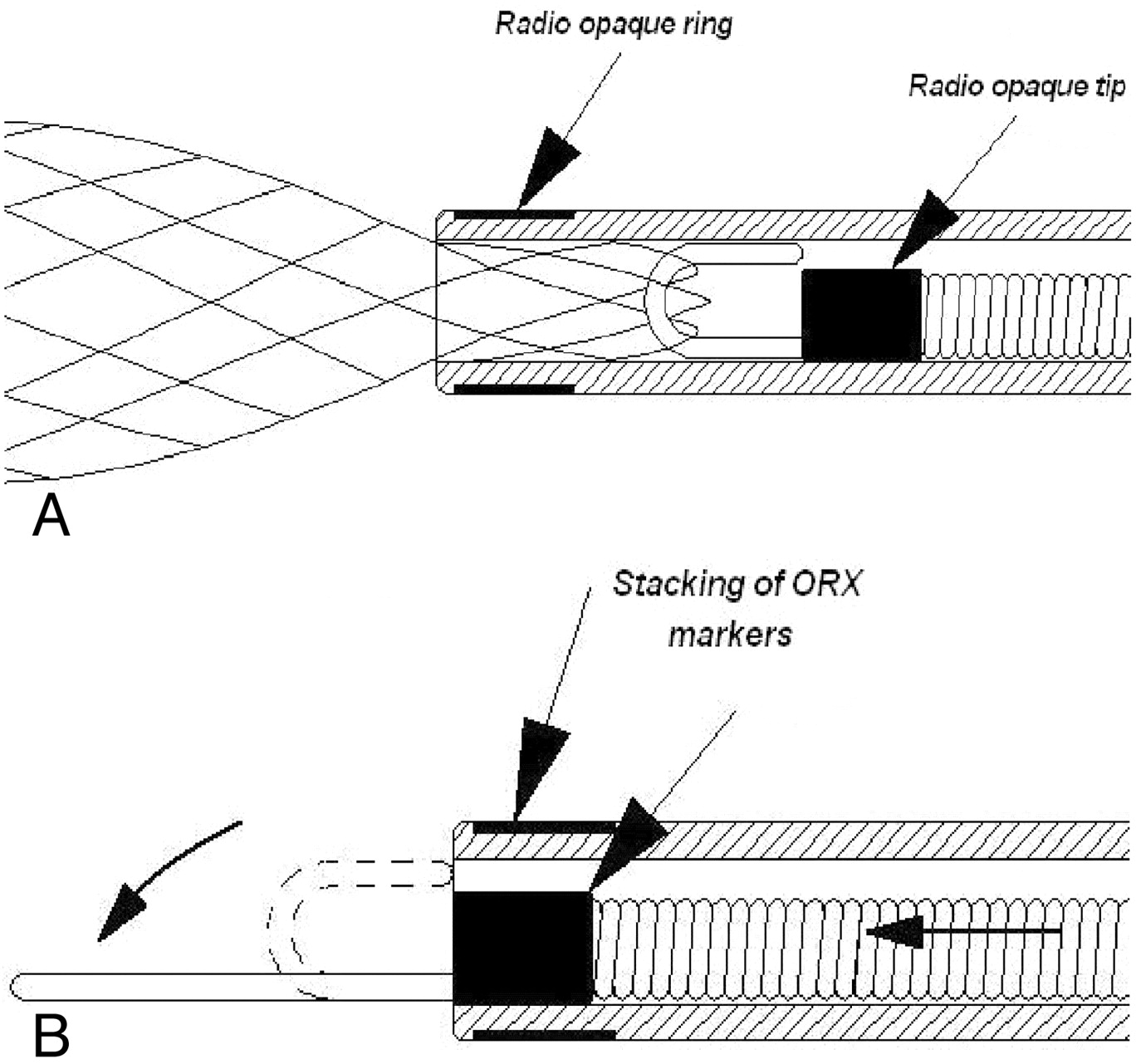
When the pusher comes out of the Vasco catheter (staking of ORX [opaque ray X mark] markers), the stent is fully out and cannot be resheathed, but it is still attached to the hook (Fig 4A). Finally, to detach the stent, it is necessary to resheath the pusher inside the catheter by advancing the catheter (Fig 4B).

A, When the pusher comes out of the Vasco catheter (staking of ORX markers), the stent is fully out and cannot be resheathed, but it is still attached to the hook.
B, To detach the stent, it is then necessary to resheath the pusher inside the catheter by advancing the catheter.
Ten patients with broad-necked aneurysms were treated with stent-assisted coiling. Six aneurysms were initially coiled, followed by stent placement.
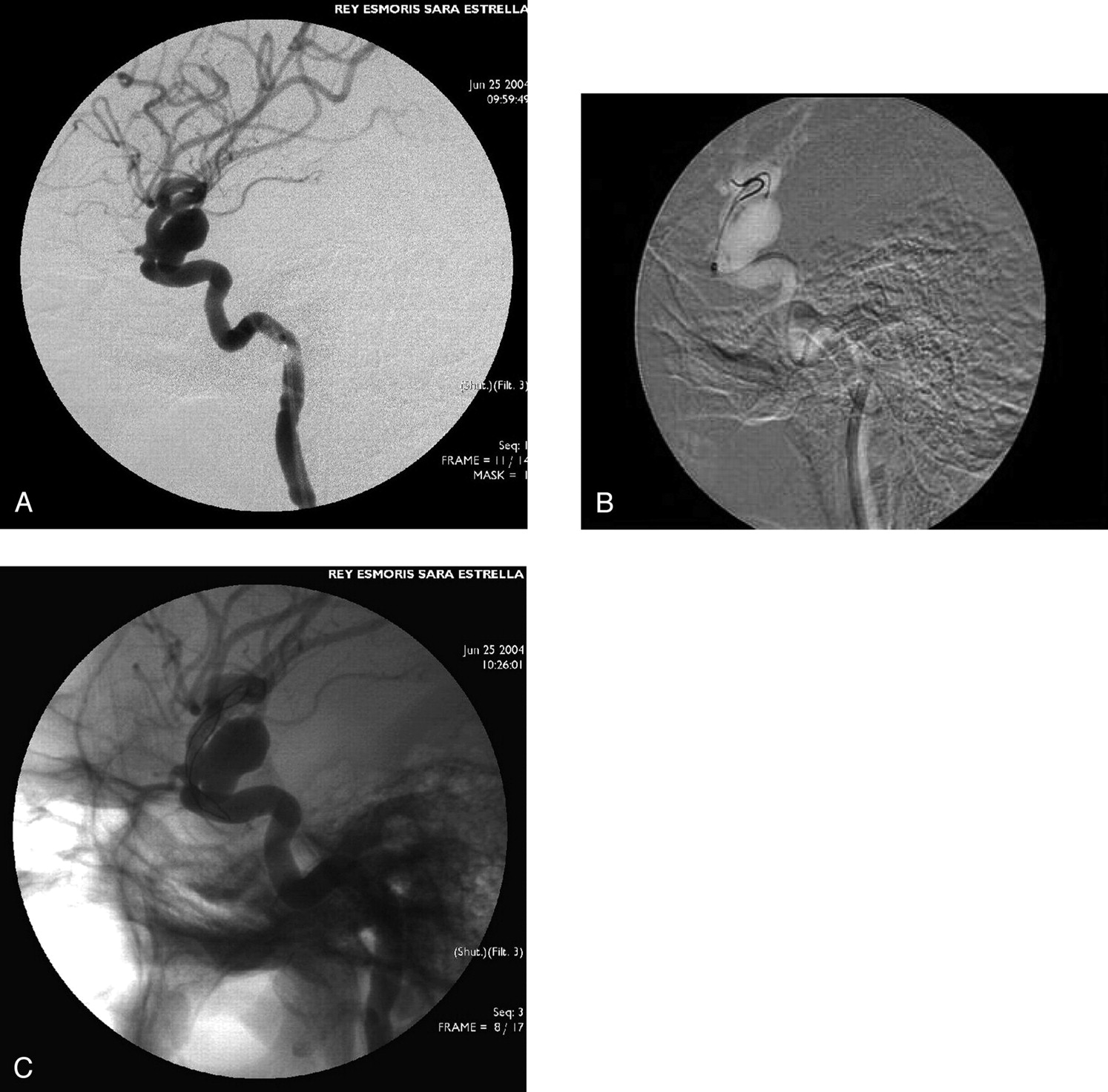
In all cases, the Leo stent delivery system could be negotiated successfully (Fig 5 and Fig 6). Significant difficulty, however, was encountered in one case; the Vasco microcatheter could not be advanced at the segment cavernous internal carotid artery; it was achieved after by using 2 microwires (.0014 inches), and then no difficulty was encountered in manipulating the stent within the microcatheter delivery (Fig 7).

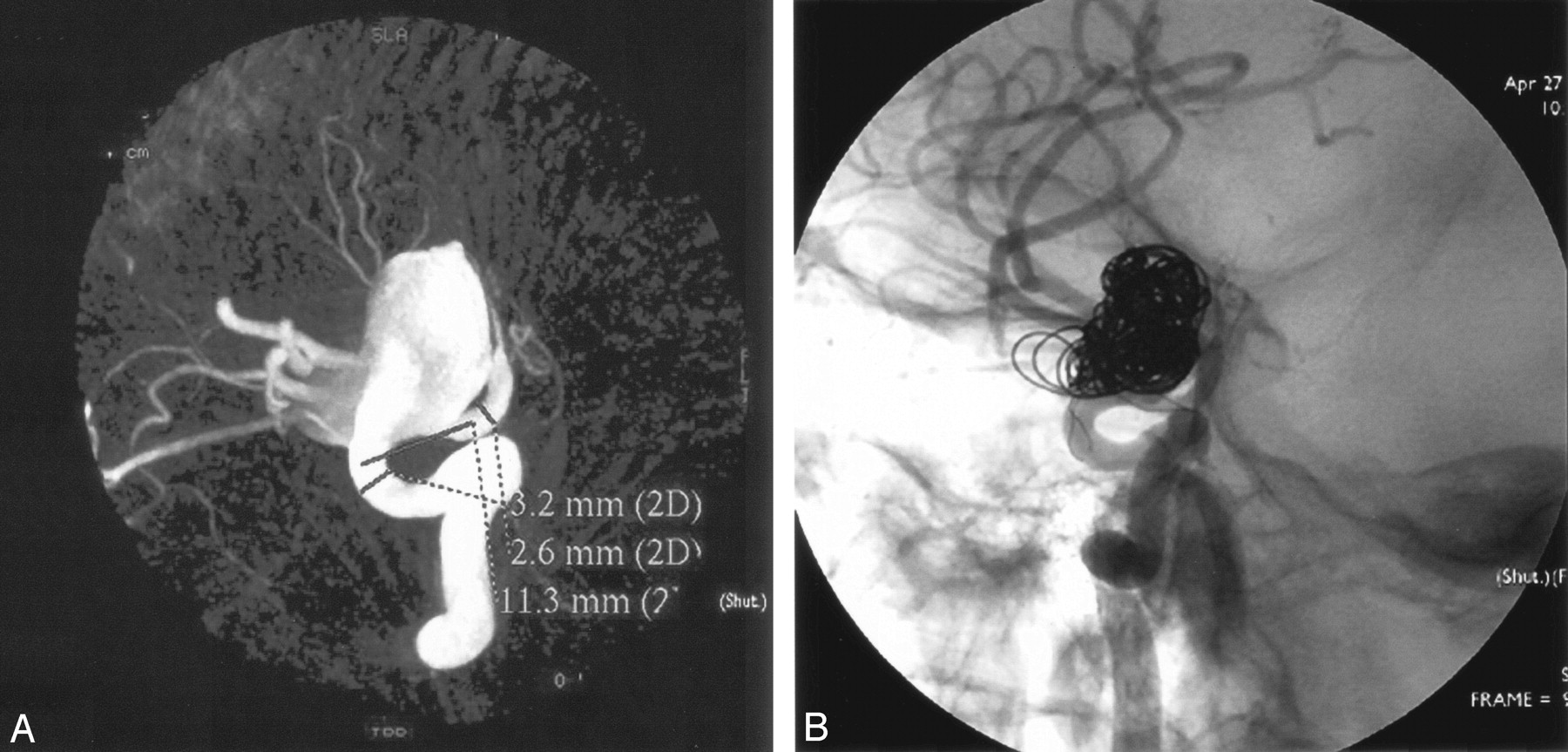
A, Reconstructed image from a 3D rotational angiogram demonstrating a wide-necked paraophthalmic aneurysm of the cavernous internal carotid artery.
B, Angiogram obtained after stent deployment and after coiling through the stent interstices shows aneurysm is occluded.

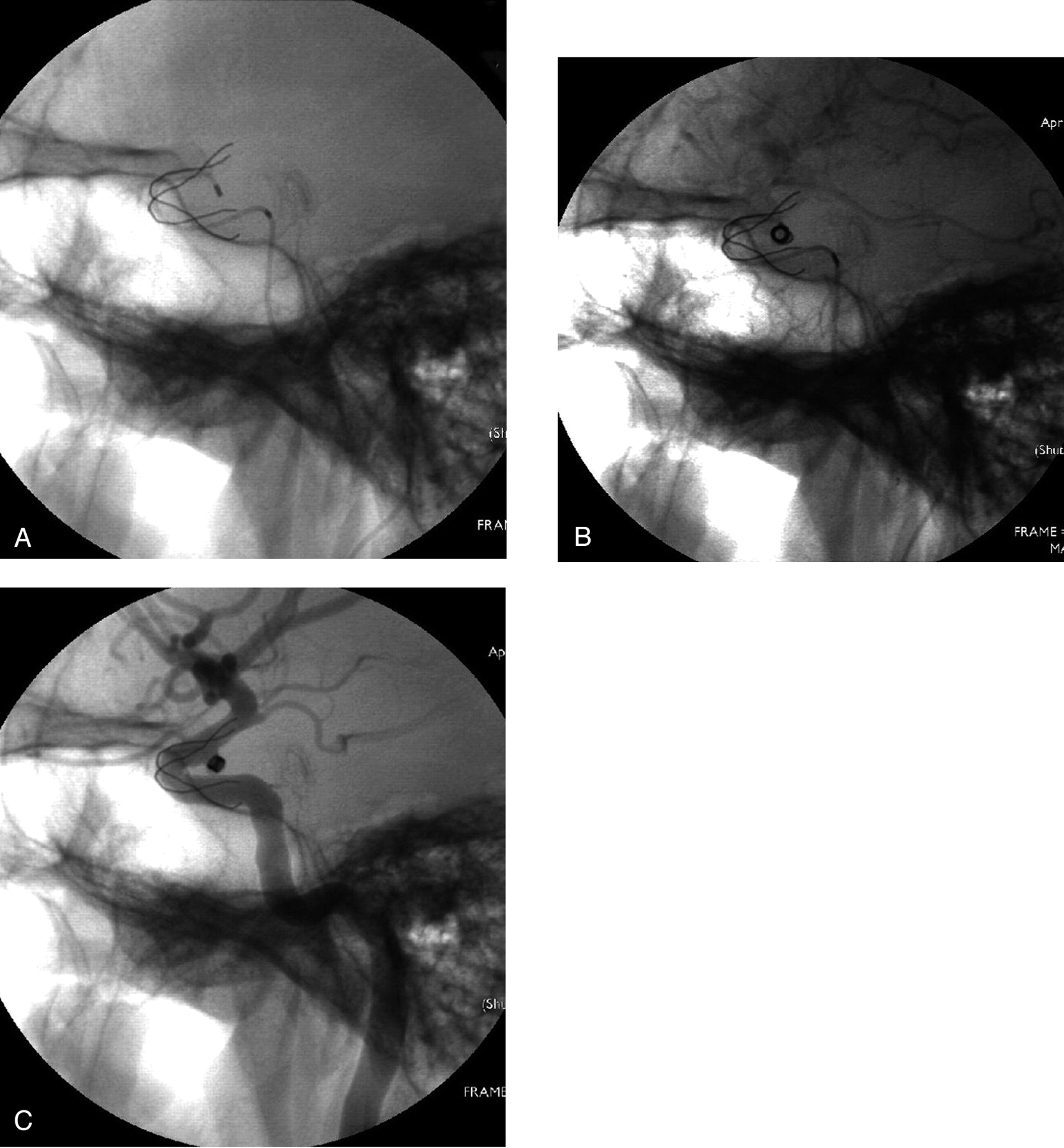
A, Prowler microcatheter in place within a cavernous aneurysm through the interstices of the stent.
B, Coiling of aneurysm across the stent.
C, Finally, total exclusion of the aneurysm.

A, Aneurysm of the cavernous internal carotid artery.
B, Two microwires (.0014 inches), which make advancing the Leo stent easier.
C, An implanted Leo stent.
In addition even the tortuous arterial segments, such as than carotid siphon, can be stented. In one case, the stent was minimally displaced during microwire manipulation for aneurysm microcatheterization through the mess stent, without clinical complications. We considered it safer to wait for the full endothelialization of the stent to the vessel wall before the complementary coiling.
In our experience, one patient suffered a left temporal thromboembolic complication that resolved with administration of abciximab (20 mg) through selective intra-arterial and venous routes, with complete resolution.
When possible, all patients who had stent-supported coiling underwent MR imaging within 24 hours of the procedure to assess subclinical complications related to stent placement, stent patency, and level of correlation between the MR angiography and conventional angiography (2). We performed follow-up review with angiography after 6 months. If there was still residual lesion the aneurysm was then completely occluded with coils.
Discussion
The first stent designed for intracranial use was the Neuroform device (Boston Scientific). This stent is constructed of nitinol and has diameters ranging from 2.5 mm to 4.5 mm and lengths ranging from 10 mm to 20 mm. It is composed of 6–8 linked cells that are essentially radiolucent and the ends of the stent are demarcated by 4 radiopaque markers that splay as the stent is unsheathed from the delivery catheter, which indicates deployment and marks the proximal and distal ends of the stent within the parent vessel. The disadvantage with this method is that there is the potential risk to move or even damage the stent when removing the microcatheter. Several technical problems with stent delivery have been reported in the literature (2, 5), including misplacement of the stent into the target aneurysm during deployment or by dislodgment during catheterization. This may be attributed to the minimal radial force exerted by the stent against the vessel wall. The Neuroform system subsequently underwent structural revision to improve the delivery characteristic of the stent and was reintroduced as the Neuroform 2 Treo (4). This stent, with its open-cell design, is similar to the Neuroform but contains a modified geometry with 3 connectors between adjacent segments, providing a 39% decrease in the area of the open cells, with the advantage of increased aneurysm neck coverage.
In our series, we used the Leo microstent, a new self-expanding stent that was designed specifically for the treatment of patients with wide-necked postcarotid siphon aneurysms. The Leo stent is constructed of a nickel-titanium shape-memory, commonly known as nitinol. The success of nitinol is attributable to 2 unique properties—shape-memory effect and superelasticity—based on the ability of nitinol to exist in 2 reversible crystalline phases. Thermal shape-memory enables nitinol implants to be compressed for insertion into delivery system and deployment but then restored to their original shape following release (6).
The Leo stent has twisted nitinol wires and 2 platinum markers. It represents important benefits: a high radial force compared with another intracranial self-expanding stents, continuous surface coverage, and ORX visualization of both diameter and length (Fig 1B). The major advantage of this delivery system is an innovative distal hook (Fig 2) that allows resheathing and repositioning of stent when it is as much as 90% deployed.
The high radial force reduces the possibility of stent displacement after deployment. Fiorella et al (2) and Broadbent et al (5) reported difficulties with redeployment of the Neuroform stent and with displacement after deployment. In our experience with the Leo stent, we have encountered none of these difficulties. In all cases, the Leo stent delivery system could be negotiated successfully.
The Leo stent represents a significant advance in the vascular treatment of intracranial aneurysms in terms of high radial force and ease of delivery.
In most cases, the Leo stent can be deployed accurately even within the most tortuous segments of the cerebral vasculature. It is a feasible, secure, and effective system in treating wide-necked intracranial aneurysms and in combination with coiling embolization offers a promising therapeutic alternative in the treatment of wide-necked aneurysms.
- Received April 8, 2005.
- Accepted after revision May 18, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Stent-assisted coiling of cerebral aneurysms: multi-center analysis of radiographic and clinical outcomes in 659 patients
- Long-term follow-up of aneurysms treated electively with woven stent-assisted coiling
- Endovascular treatment of complex intracranial aneurysms using Acandis Acclino stents
- Aneurysm pressure measurement before and after placement of a Pipeline stent: feasibility study using a 0.014 inch pressure wire for coronary intervention
- Low-profile Visualized Intraluminal Support device (LVIS Jr) as a novel tool in the treatment of wide-necked intracranial aneurysms: initial experience in 32 cases
- Use of Flow-Diverting Devices in Fusiform Vertebrobasilar Giant Aneurysms: A Report on Periprocedural Course and Long-Term Follow-Up
- Intra-aneurysmal hemodynamic alterations by a self-expandable intracranial stent and flow diversion stent: high intra-aneurysmal pressure remains regardless of flow velocity reduction
- A Novel "Y" Stent Flow Diversion Technique for the Endovascular Treatment of Bifurcation Aneurysms without Endosaccular Coiling
- Stent Conformity in Curved Vascular Models with Simulated Aneurysm Necks Using Flat-Panel CT: An In Vitro Study