
Abstract
Summary: Coiling of a wide-necked basilar tip aneurysm can be accomplished in selected cases by placing a single Neuroform stent horizontally across the aneurysm neck via a posterior communicating artery approach rather than by placing 2 stents in a Y configuration via a basilar artery approach.
Treatment of a wide-necked cerebral aneurysm may require a modification of the standard coiling technique such as use of 3D coils, balloon neck remodeling, or placement of one or more stents across the aneurysm neck to prevent coil prolapse into the parent artery (1, 2). In the case of a terminal aneurysm, it is often difficult or impossible to place a device such as a balloon or stent exactly perpendicular to the axis of the aneurysm or, in the case of a basilar tip aneurysm, horizontally, parallel to both P1 segments. One approach has been to place 2 stents at the arterial termination in a Y configuration, one through the other, both beginning proximally in the parent artery and ending distally, one in each of the 2 terminal branches (3). Placing 2 stents in this manner is a compromise that does not quite allow either stent to reach the aneurysm neck at its midportion, leaves more metal in the arterial system permanently, and doubles the cost compared with placing one stent in optimal position. We present a case with follow-up in which one Neuroform stent was placed horizontally at the basilar termination via a posterior communicator approach for coiling of a wide-necked basilar tip aneurysm.
Description of the Technique
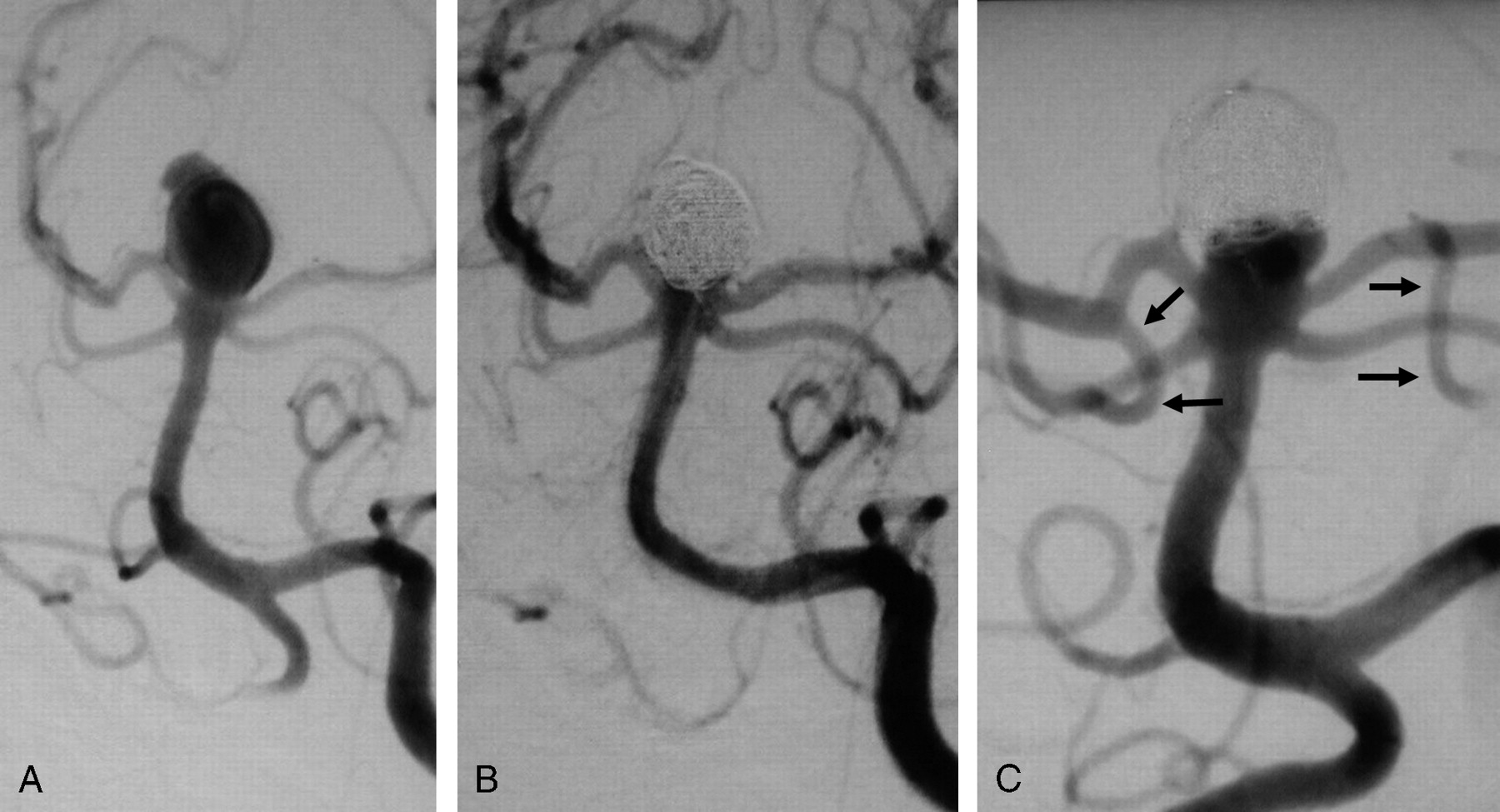
A 29-year-old woman presented in June 2003 with complaints of sudden, severe headache, nausea, and vomiting. Her past history was notable for hypertension and chronic headaches, and her family history was positive for aneurysmal subarachnoid hemorrhage. On examination, she was drowsy but otherwise neurologically intact. In addition to subarachnoid and intraventicular blood, her brain CT scan showed mild hydrocephalus. A ventricular drain was placed. Her cerebral angiogram demonstrated a 10-mm aneurysm projecting superiorly and posteriorly with an irregular dome and a 4-mm neck atop a basilar artery having a junctional infundibulum (Fig 1A).

A, Aneurysm at presentation after subarachnoid hemorrhage. B, Initial post-treatment appearance. C, Recurrence at 6 months. Note posterior communicating arteries, right larger than left (arrows).
During that hospital admission, her basilar tip aneurysm was treated, while she was under general anesthesia, by standard endovascular coiling using a combination of coated and bare platinum coils. The aneurysm was approximately 90% obliterated (Fig 1B). The patient’s mental status improved to normal, her ventriculostomy catheter was removed, and she was discharged home neurologically intact.
Six months after her initial aneurysm treatment, the patient was well except for intermittent headaches. Her routine follow-up angiogram at that point showed an approximate 25% recurrence at the base of the aneurysm due to coil compaction (Fig 1C). Retreatment of the aneurysm was recommended. The patient delayed retreatment for an additional 6 months.
In July 2004, approximately 1 year following her initial aneurysm treatment, an attempt to retreat the aneurysm was made. The patient was pretreated with aspirin and clopidogrel bisulfate (Plavix), administered under general anesthesia, and anticoagulated with intravenous heparin. Angiography showed no interval change in the appearance of the recurrent aneurysm. Because of the width of the aneurysm neck and the shape of the recurrent sac, the initial retreatment attempt was made by using the balloon neck–remodeling technique. This attempt was abandoned after every type of coil deployed in the aneurysm prolapsed into the basilar artery upon balloon deflation.
In a subsequent procedure, again under general anesthesia with antiplatelet and anticoagulant therapy and with informed consent as mandated by the human studies committee for use of a Neuroform stent (Target Therapeutics, Fremont, CA) as a humanitarian device, the aneurysm was successfully retreated by using a stent-assisted coiling technique. Images of the arterial and aneurysm anatomy demonstrated 2 posterior communicating arteries, right larger than left (Fig 1C). To place the stent horizontally across the aneurysm neck, parallel to the P1 segments and perpendicular to the axis of the aneurysm, the decision was made to place a microcatheter-deliverable stent across the aneurysm neck through a posterior communicating artery, and a right-sided approach was chosen.
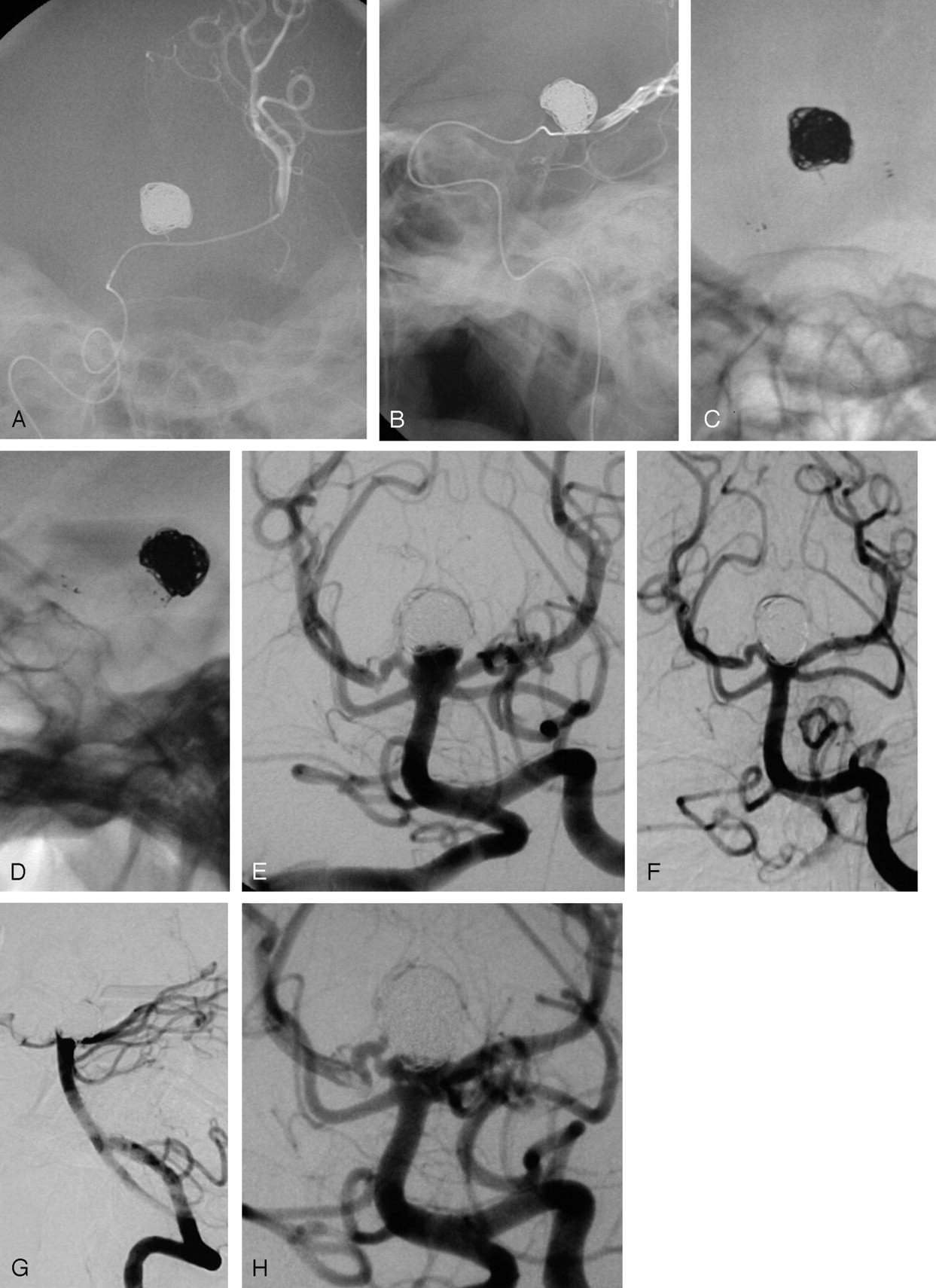
A Prowler-14 microcatheter introduced through a 5F Envoy (Cordis) right internal carotid artery guide catheter was advanced over an Agility-14 microwire (Cordis) into the right posterior communicating artery. Using roadmaps obtained by injecting the guide catheter and microcatheter at various points, the microcatheter tip was directed into the right P1 segment, across the basilar artery tip, into the left P1 segment, and then into the left P2 segment (Fig 2A and B). By using a microcatheter-generated roadmap of the left posterior cerebral artery, the standard length Agility microwire was replaced with an exchange length (350 cm) Agility-14 microwire. The exchange wire tip was positioned in a left parieto-occipital branch, and the Prowler-14 microcatheter was exchanged for a 3.5 mm × 20 mm Neuroform-II stent delivery system. The stent was positioned and then deployed so that its distal markers were in the left P1 segment beyond the neck of the aneurysm and the proximal markers were in the right posterior communicating artery (Fig 2C–E). Coils previously placed in the aneurysm served as a convenient reference for the position of the aneurysm. The stent delivery system and microwire were removed. The carotid guide catheter was removed.

A and B, Microcatheter coursing from right internal carotid through right posterior communicator, right P1 segment, basilar tip, and left P1 segment into left P2 segment. C (PA) and D (lateral), Neuroform stent deployed across aneurysm neck, with distal markers in left P1 segment and proximal markers in right posterior communicating artery. E, Arterial appearance immediately following stent deployment. F and G, Aneurysm after coil embolization of recurrent portion with stent support. H, Appearance 6 months after stent placement and coil retreatment. (Unopacified inflow from posterior communicating artery confirms its patency.)
Through a left vertebral artery Envoy guide catheter, a Prowler-14 microcatheter and Agility-14 microwire were advanced through the basilar artery, through the Neuroform stent, and into the recurrent aneurysm. Coils (Target GDC-10 2D 6 mm × 20 cm and 5 mm × 15 cm; GDC-10-soft SR 5 mm × 8 cm, 4 mm × 8 cm, 4 mm × 6 cm, and 3 mm × 6 cm; and GDC Ultrasoft 2 mm × 4 cm, 2 mm × 3 cm, and a pair of 2 mm × 2 cm) were deployed and detached in the recurrent aneurysm, this time without the problem of prolapse into the basilar artery. Left vertebral and right internal carotid angiography at the conclusion of the procedure showed approximately 95% aneurysm obliteration (Fig 2F and G), preservation of the right and left P1 segments and right posterior communicating artery, and no arterial thrombus or embolus. The heparin infusion was terminated. The patient remained neurologically intact throughout the remainder of her hospitalization and was discharged home with the prescription of 2 months of Plavix, 75 mg, and aspirin, 325 mg, daily, then aspirin alone.
On follow-up 6 months after retreatment, the patient remained neurologically intact with occasional mild headaches. Her angiogram at that point demonstrated stable 95% obliteration of the aneurysm and preserved right P1, left P1, and right posterior communicating arterial segments. There was slight narrowing of the right P1 segment (Fig 2H).
Discussion
Achieving a stable, complete, uncomplicated obliteration of a ruptured basilar tip aneurysm with a wide neck is a challenge, despite recent modifications in coil configurations, the addition of various coatings to platinum surfaces, and procedural modifications such as balloon remodeling and stent support across the aneurysm neck. This example illustrates some typical problems encountered early in the course of treatment of a ruptured aneurysm with this geometry and a variation in stent placement used electively that may be useful in similar situations to achieve a good final result.
The variation in stent placement herein was deployment of a Neuroform stent across the neck of the basilar tip aneurysm from a carotid approach through the posterior communicating artery. This differs from the usual vertebral approach in which one Neuroform stent is deployed from the distal basilar artery into one P1 segment across a portion of the basilar tip aneurysm neck or 2 Neuroform stents are deployed, one through the other, both from the distal basilar artery, each into one P1 segment in a Y configuration across the aneurysm neck. There are several potential advantages of the posterior communicating approach.
The geometric problem of placing a single Neuroform stent across a basilar tip aneurysm neck into one P1 segment from a vertebral approach is that the stent does not cover the entire neck of the aneurysm. A stent placed in such a way is not perpendicular to the axis of the aneurysm or parallel to the axis of the aneurysm neck, so coils deployed in the aneurysm can still prolapse into the basilar artery through the aneurysm neck around the stent. The geometric problem of placing 2 Neuroform stents in a Y configuration from a vertebral approach is that neither stent approximates the midportion of the aneurysm neck at the middle of the Y, so coils deployed in the aneurysm could still protrude into the basilar artery lumen at its termination, despite being contained by the stents, assuming the aneurysm neck is in a horizontal configuration. One advantage of placing a Neuroform stent from a posterior communicating approach is a geometric one, deployment of the stent horizontally across the aneurysm neck, with the stent parallel to the P1 segments and axis of the aneurysm neck and perpendicular to the axis of the aneurysm dome. Advantages of placing a single stent over placing dual stents include the reduction in device-related cost (several thousand dollars) and the reduction in the amount of metal remaining permanently within the parent arterial system to serve as a source for thrombi or emboli.
Whether a horizontally placed single stent would lead to less intimal hyperplasia in the distal basilar artery and P1 segments than 2 stents placed in a Y configuration is a matter of speculation, as is whether flow dynamics at the aneurysm neck following deployment of a horizontally oriented stent would be any more favorable for further aneurysm thrombosis and less coil compaction over time (4). In this case illustration, the slight narrowing of the right P1 segment on the 6-month posttreatment angiogram is likely related to intimal hyperplasia along the course of the stent. This aneurysm initially treated with a combination of coated and bare platinum coils recurred, whereas there was no recurrence following its retreatment with bare platinum coils supported by a single horizontally oriented stent. This case also illustrates the advantage of Neuroform stent placement over balloon remodeling, because a permanent barrier was required across the aneurysm neck to prevent coil prolapse into the parent artery.
This technique cannot be used when the posterior communicating artery is very small in size or when its geometry is too tortuous to allow catheterization via this route. Placement of Neuroform stents for aneurysm treatment is generally reserved for elective situations, because use of Plavix and aspirin is contraindicated in acute subarachnoid hemorrhage and ventriculostomy catheter placement, maintenance, and withdrawal (5). If this approach is feasible from an anatomic standpoint, it may be preferable, as in this case, to treat an aneurysm as effectively as possible by using a standard endovascular coiling method at the time of subarachnoid hemorrhage and treating any recurrence or residual aneurysm later under controlled conditions. This, of course, would not be an issue in the elective treatment of an unruptured aneurysm.
Conclusion
In anatomically and clinically appropriate situations, placement of a single Neuroform stent via a posterior communicating artery approach horizontally across a wide basilar tip aneurysm neck may be the optimal stent deployment method.
References
- Received April 8, 2005.
- Accepted after revision May 18, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transcirculation approach for stent-assisted coiling of intracranial aneurysms: a multicenter study
- Kissing-Y stenting for endovascular treatment of complex wide necked bifurcation aneurysms using Acandis Acclino stents: results and literature review
- Treatment of basilar tip aneurysms with horizontal PCA to PCA stent-assisted coiling: case series
- Y-Configuration Stent Placement (Crossing and Kissing) for Endovascular Treatment of Wide-Neck Cerebral Aneurysms Located at 4 Different Bifurcation Sites
- Stent-Assisted Coiling of Intracranial Bifurcation Aneurysms Leads to Immediate and Delayed Intracranial Vascular Angle Remodeling
- Horizontal deployment of an intracranial stent via an antegrade approach for coil embolization of a basilar apex aneurysm: technical note
- Treatment of coil embolization failed recurrent giant basilar tip aneurysms with bypass and surgical occlusion
- Treatment of Intracranial Aneurysms by Functional Reconstruction of the Parent Artery: The Budapest Experience with the Pipeline Embolization Device
- Neuroform stent assisted aneurysm treatment: evolving treatment strategies, complications and results of long term follow-up
- Retrograde crossing stent placement strategies at the basilar apex for the treatment of wide necked aneurysms: reconstructive and deconstructive opportunities