
Abstract
Summary: We describe two cases of a bifid mandibular condyle. The first case is a 48-year-old woman with headaches and a pain and clicking sensation in her right jaw during mastication. The second case is an asymptomatic 17-year-old woman with a history of bilateral microtia and hemifacial microsomia. In both patients, the bifid condyle was first identified by CT and affected the temporomandibular joint. The imaging findings of both patients’ bifid mandibular condyles led us to conclude that both patients likely had an abnormal development of the mandibular condyles. We believe that an intervening fibrous or vascular structure may have split the condyle into two heads.
The presence of a bifid mandibular condyle is a rare condition (1–5), most commonly reported as an incidental, unilateral finding (1, 6–8). More cases have been identified on autopsy than in clinical settings (6). Reported cases of the bifid mandibular condyles in living subjects have been reported in asymptomatic patients and in association with temporomandibular joint (TMJ) ankylosis (7, 8). Our review of literature identified only 56 cases of this rare anomaly (Table). There has been only one case report of a bifid mandibular condyle in association with the hemifacial microsomia, which was identified in our second patient (9).
Cases of bifid condyles reported in literature
Herein, we report two subjects with a bifid mandibular condyle. CT identified duplication of the condylar head in both cases; furthermore, MR imaging was used to further characterize the meniscus of the affected TMJ.
Case Reports
Case 1
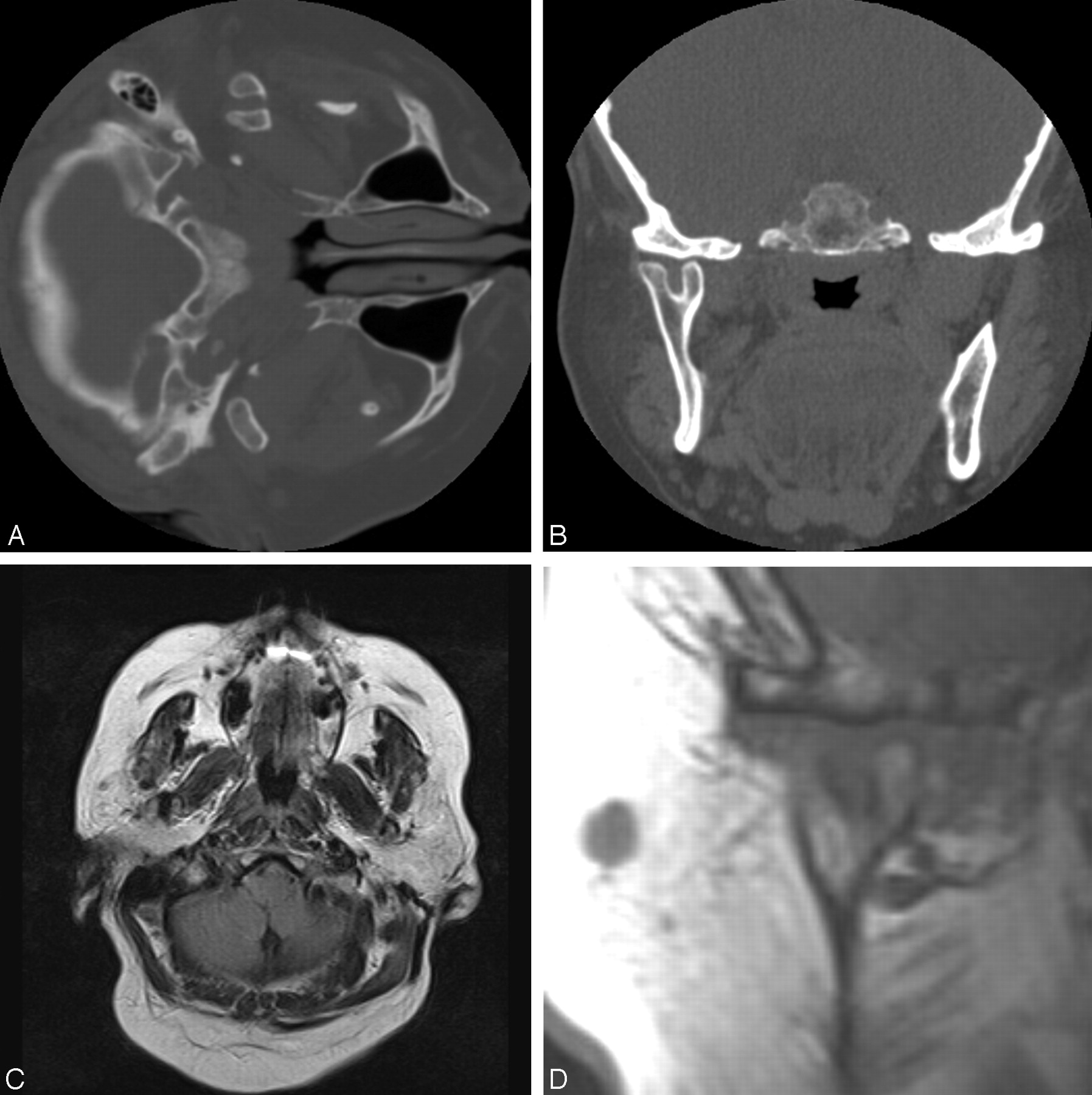
The patient was a 45-year-old woman with a history of headache that lasted several hours in duration and occurred multiple times a week for several years. She described poorly localized pain, which radiated throughout her head. During a particularly severe episode, the patient presented to an emergency department and underwent head CT imaging. The study revealed a right mandible with two condylar processes with a side-by-side orientation, one medially and the second laterally. The patient was asked to return for further imaging. Follow-up axial (Fig 1A) and coronal (Fig 1B) images of the mandible better demonstrated the medial and lateral condylar heads of the affected side. These images further demonstrated the two articulating facets in the right temporomandibular fossa, each articulating with one of the condylar processes. On further questioning, the patient revealed that she experienced a clicking sensation near the right TMJ with chewing. The patient also recalled intermittent TMJ pain following meals requiring excessive mastication. She described bilateral pain, more severe on the right. The patient also admitted to favoring her left side during chewing. The patient denied any history of bruxism or problems swallowing. Review of the family history and discussion with family members failed to elucidate similar symptoms in other members of the family.

Axial (A) and coronal (B) thin-cut CT images through the mandible demonstrate a bifid mandibular condyle on the right side with mediolaterally oriented heads.
C, Axial, T1-weighted MR imaging demonstrates the bifid mandibular condyle on the right side, but also demonstrates subtle fatty atrophy of the muscles of mastication ipsilaterally.
D, Coronal T1-weighted MR imaging images demonstrate the bifid condyle on the right side and also demonstrate that the meniscus has the shape of a T, with a third limb interdigitating between the two mandibular heads.
The additional MR imaging study identified atrophy and fatty replacement of the muscles of mastication, including both of the pterygoid muscles, the masseter, and the lower temporalis muscles on the right side, as compared with the unaffected, contralateral side (Fig 1C). Marrow edema was seen in the duplicated right condylar heads but was more prominent in the lateral head. The meniscus of the affected TMJ was T-shaped with a separate limb for each of the condylar heads. A third limb of the meniscus was seen interdigitating between the two mandibular heads (Fig 1D).
Case 2
The second patient was a 17-year-old woman from Bolivia with left hemifacial microsomia and bilateral microtia, who sought treatment for her facial asymmetry. CT of the temporal bones was requested for the surgical planning. The left mandibular condyle was noted to have an aberrant small medial condyle in addition to a larger, lateral condyle (Figs 2A–D). Further questioning failed to elicit any symptoms referable to her TMJ. Additional CT findings included the bilateral, complete atresia of the external auditory canals with abnormalities of the middle ear structures, including the opacified mastoid air cells, a small epitympanic recess, and the malformed, hypoplastic ossicles.

A, Coronal thin-cut CT images demonstrate that the left mandibular condyle is bifid, with mediolaterally oriented heads. Although both mandibular heads are small and deformed, the left is much smaller than the right.
B and C, Axial, T1-weighted MR imaging images again demonstrate the bifid mandibular condyle.
D, Coronal images demonstrate the mediolaterally oriented heads and also show the T-shaped meniscus, with the descending limb of the T interdigitating between the mediolaterally oriented heads.
The patient’s past surgical history was significant for prior auricular reconstructions in 1992 and 1994 and also mandibular distraction osteogenesis. The limited records and operative reports from Bolivia made no specific mention of any mandibular abnormalities.
Discussion
Duplication of the mandibular condyle is exceptionally rare. The study of 1,882 cadaveric skulls by Szentpetery et al found the incidence of this anomaly to be 0.48% (8). Two differing theories have been postulated to account for the pathogenesis of the mandibular condyle duplication. Blackwood (10) and Moffett (3) have suggested that a retained fibrous septum or a vascular structure impede ossification of the mandible, splitting the condyle into two heads. By contrast, Thomason and Yusuf (11) have suggested prior trauma as a cause; however, the duplication has been described in patients without any antecedent identifiable traumatic event (1–3, 6).
The orientation of the mandibular head has been used as a differentiating factor. The mediolateral orientation is presumed to result from a developmental cause; however, a sagittal split with anteroposterior orientation has been associated with an antecedent identifiable, traumatic event (2, 6, 8, 12). Yao et al, however, demonstrated experimentally that a fracture of the mandibular condyle could result in mediolateral (13) as well as anteroposterior orientation (14) of the mandibular condyles.
We tend to support the hypothesis that a bifid condyle with mediolateral heads is likely to be related to a developmental phenomenon rather than trauma. Neither patient in this study had identifiable traumatic injury or duplicated condylar heads with mediolateral orientation. The association of the anomaly in the second patient with a rare hemifacial microsomia also prompts us to conclude that the cause for her duplicated condylar head is likely to be developmental.
In the past, duplication of the mandibular condyle had been described on conventional radiographs, mostly panorex views (4, 6, 8, 15). The panorex views often demonstrated the two mandibular heads with either anteroposterior orientation, as in the case of traumatically induced bifid mandibular condyle, or mediolateral in the setting of a presumed developmental abnormality. Conventional radiographs of the mandible were not available for either of our patients, because of their clinical histories and presentations. To the best of our knowledge, this report is the first description of a T-shaped meniscus and the first depiction of the MR imaging appearance of the bifid mandibular condyle in the English-language medical literature.
According to the Blackwood’s postulate, a band of vascular or fibrous tissue should have been identified between the two condylar heads on MR imaging (10). The lack of MR imaging visualization of a fibrous band or of an abnormal vascular structure would contradict this hypothesis. The fibrous or vascular tissue, however, may have been present in the embryonic period before the ossification of the mandibular condyle but regressed later in the development.
Conclusion
We believe this case report to be only the second reported association of hemifacial microsomia and the bifid mandibular condyle (9). Further cases may be identified with a more systematic imaging approach to patients with hemifacial microsomia. In the future, the mandibular condyle may come under closer scrutiny during the reviews of these imaging studies.
We have herein reported two patients with a bifid mandibular condyle. A study of a series of patients with hemifacial microsomia would be helpful to evaluate the true prevalence of the bifid mandibular condyle as part of a syndromic association or predisposition. Although, the panorex views have been traditionally used for diagnosis, With CT imaging becoming more common, CT scans rather than conventional radiographs were used to diagnose our patients. We believe that special attention should be given to the mandible in patients with any referable symptoms. MR imaging evaluation in the identified patients may reveal other variants of the meniscal shape or potentially confirm the T-shaped meniscus, seen in our patient, as a common finding in patients with a bifid condyle.
References
- Received June 7, 2004.
- Accepted after revision October 7, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Bifid mandibular condyle
- Bifid mandibular condyle: CT and MRI appearance
- Tetrafid mandibular condyle: a unique case report and review of the literature
- Bifid Mandibular Condyle: A Disorder in Its Own Right?
- The frequency of bifid mandibular condyle in a Turkish patient population
- Bifid mandibular condyle with associated temporomandibular joint ankylosis: a computed tomography study of the patterns and morphological variations
- The prevalence of bifid mandibular condyle detected in a Brazilian population