
Abstract
Summary: We describe the appearance of endogenous bacterial endophthalmitis in a patient who underwent MR imaging of the orbits before and during the course of treatment. Intraocular hyperintensity on fluid-attenuated inversion recovery and diffusion-weighted images were found very useful for diagnosing endophthalmitis. After a few days of treatment, a marked relative increase in intraocular mean apparent diffusion coefficient values was observed, which appears to indicate good treatment response.
Endophthalmitis refers to any intraocular inflammatory process that may result from infectious or noninfectious (sterile endophthalmitis) causes, but in clinical practice it usually means inflammation secondary to intraocular infection and is broadly classified as exogenous or endogenous. Exogenous endophthalmitis is more common and occurs following intraocular surgery, penetrating injury, corneal ulcer, or periocular infection, when disruption of the external ocular barriers allows infective agents access to the intraocular spaces. It is most frequently a postoperative complication of cataract surgery (1, 2). Endogenous endophthalmitis, also termed metastatic endophthalmitis, is an intraocular infection resulting from hematogenous bacterial spread when organisms enter the internal ocular spaces by crossing the blood-ocular barrier (1). It can occur in isolation but is usually associated with other foci of infection. Endogenous endophthalmitis is less common than exogenous endophthalmitis and accounts for only 2%–7% of all cases of endophthalmitis (1, 3). Endogenous endophthalmitis is associated with underlying medical conditions, particularly diabetes, intravenous drug use, and renal failure in most patients (1, 3).
The typical presenting symptoms of endogenous bacterial endophthalmitis (EBE) are ocular pain or discomfort, blurred vision, red eye, and swollen eyelids. Classic findings on physical examination include injected and chemosed conjunctiva, corneal edema and clouding, anterior chamber inflammation and hypopyon, a reduced or absent red reflex, decreased visual acuity, elevated intraocular pressure, and poor fundal view secondary to intraocular inflammation (1–3). Radiologic imaging studies are not routinely performed, because diagnosis is generally made on the basis of history and physical examination. Blood cultures and intraocular fluid are obtained to guide therapy. The most common etiologic organisms in endogenous endophthalmitis are S aureus, Klebsiella pneumoniae, Candida, and Aspergillus species. Imaging modalities that may be used to aid diagnosis and follow-up usually include ocular sonography and CT (4, 5). Treatment involves the use of intravenous and intravitreal antibiotics, as well as possible subconjunctival or topical steroids (1–4).
Endogenous endophthalmitis still presents a diagnostic and therapeutic challenge. Most patients with this rare but serious condition are initially misdiagnosed, leading to delay in effective treatment and resulting in a poor visual prognosis. The incidence of endogenous endophthalmitis is expected to rise because of the longer life span of very ill patients and increasing use of invasive medical procedures (1, 3).
Case Report
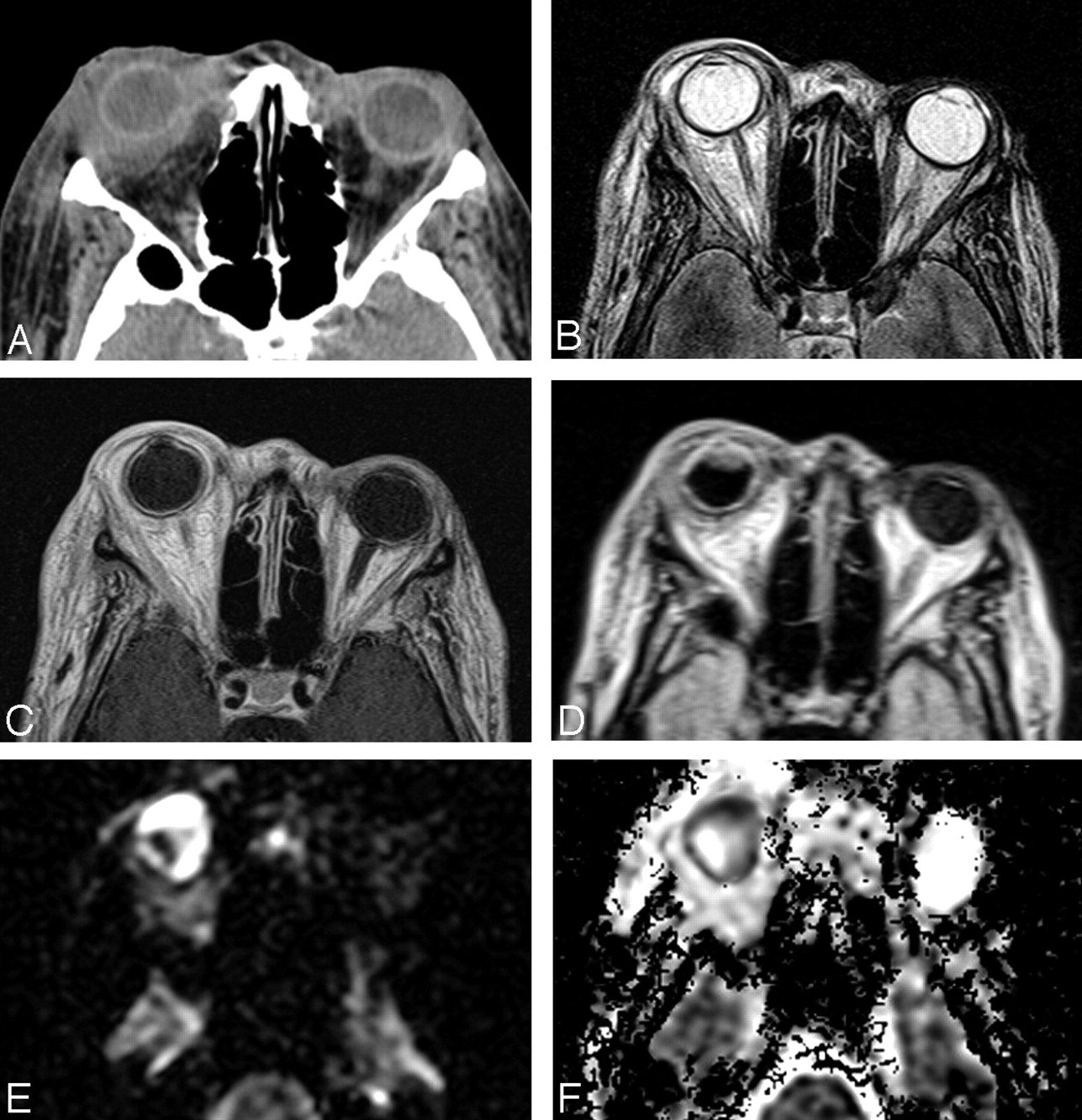
A 52-year-old woman with poorly controlled diabetes mellitus was admitted to the ophthalmology service for a 1-week history of progressive right eye erythema, swelling, pain, and proptosis. The physical examination revealed a frozen globe, injected and chemosed conjuctiva, scleral edema, absence of red reflex, and blindness of the right eye. The patient had a history of bilateral cataracts and remote surgery for bilateral glaucoma. On admission, the patient underwent a contrast-enhanced CT of the orbits (Fig 1A), which showed right preseptal edema with diffusely thickened and enhancing sclera. There was also exopthalmos and intraconal fat stranding, consistent with orbital cellulitis. After obtaining samples for blood cultures and intravitreal specimens, the patient was empirically started on antibiotics and antifungal medications. Later the same day, the patient underwent MR imaging of the orbits, including diffusion-weighted imaging (DWI), apparent diffusion coefficient (ADC) mapping, and fluid-attenuated inversion recovery (FLAIR) sequence. Conventional T2-weighted, short time inversion recovery (STIR), and T1-weighted MR of images with and without contrast did not reveal additional diagnostic information (Fig 1B, -C). There was increased signal intensity within the peripheral aspects of right globe on FLAIR and DWI (Fig 1D, -E), with corresponding very low signal intensity on ADC mapping (Fig 1F), with mean ADC values decreased down to 20% compared with the values in the contralateral globe. These findings were interpreted as representing endophthalmitis. There was no evidence of infectious process spread into the cavernous sinus or intracranially.

Imaging of a 52-year-old woman with endophthalmitis, before intravitreal and systemic antibiotic therapy.
A, Axial contrast-enhanced CT image shows marked periscleral thickening and enhancement on the right. The right vitreous body is of slightly increased attenuation.
B, Axial T2-weighted image at a similar level shows periscleral hyperintensity surrounding the right globe. There is no difference in signal intensity or appearance between the 2 vitreous bodies.
C, Corresponding axial contrast-enhanced T1-weighted image reveals enhancement on the right, both periscleral and along the entire uveal tract. There is no evidence of enhancement within the vitreous body.
D, Corresponding axial FLAIR image shows hyperintense uveal tract that is contiguous with a nodular lesion in the anterior aspect of the right globe. The rest of the right vitreous body appears hypointense compared with the contralateral globe. The periscleral abnormality is less conspicuous.
E, Axial DWI at a similar level demonstrates marked hyperintensity within the right orbit, especially in the anterior and medial aspect of the globe.
F, Corresponding axial ADC map shows that the diffusion is indeed decreased within the right globe, with signal intensity comparable to and lower than the brain parenchyma. The mean ADC value in the anterior and medial aspect measured 573 × 10-6 mm2/s, and in the central portion 2808 × 10-6 mm2/s. The left globe is hyperintense, similar to the intracranial CSF, with mean ADC value of 2813 × 10-6 mm2/s.
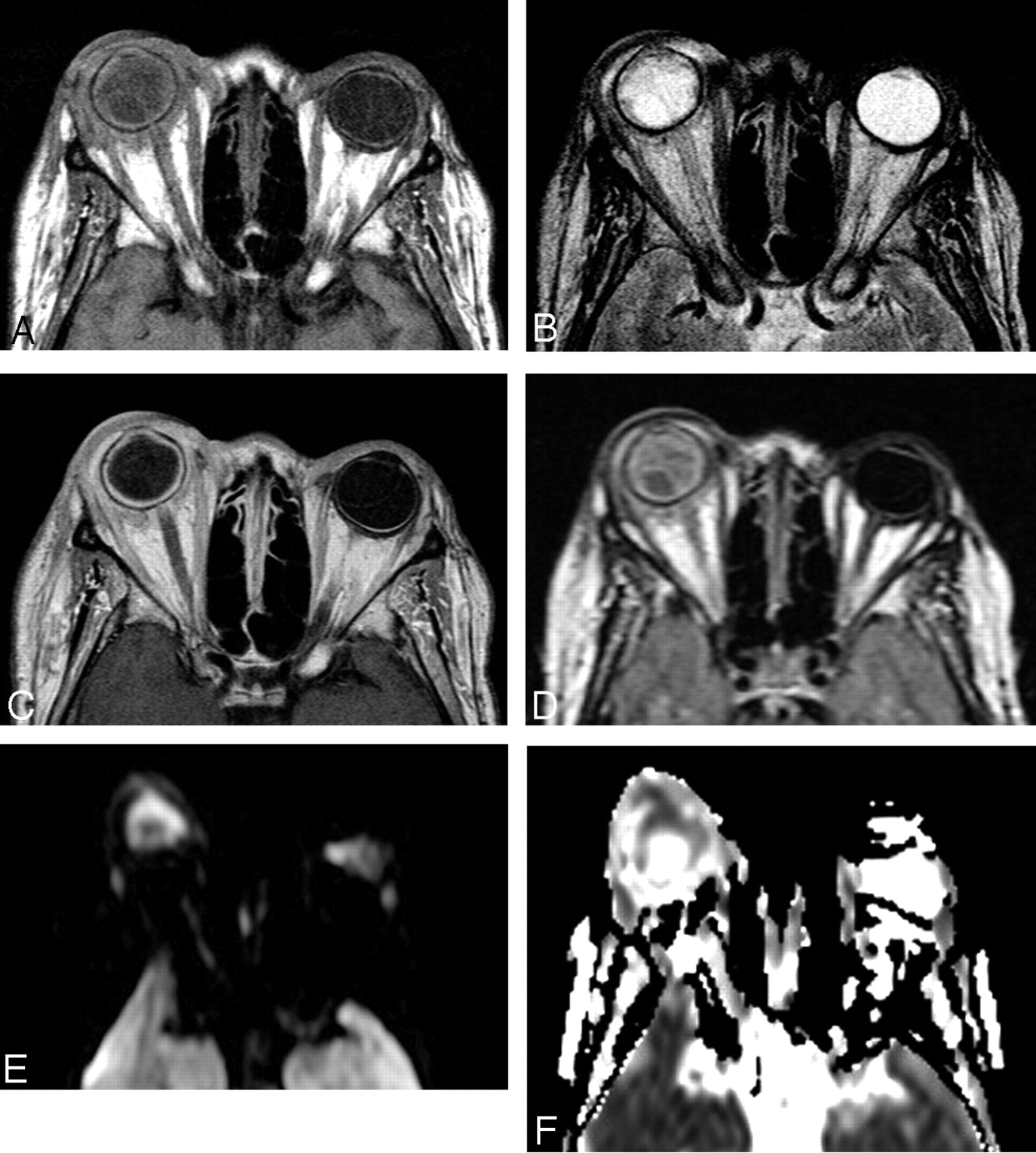
The intravitreal specimens were culture positive for methicillin-sensitive S aureus. The patient’s antibiotic regimen was adjusted and she continued on intravenous antibiotic therapy for 1 additional week. A dose of intravitreal antibiotics was also administered. A follow-up MR imaging study (Fig 2) was performed 5 days after the antibiotic treatment was started, in an attempt to assess treatment response. The study showed relative decrease in signal intensity on the DWI with corresponding increase on ADC maps. The mean ADC values showed increase by >60% compared with the prior study. This was interpreted as a good treatment response, but the patient remained in the hospital under close observation for several additional days. There was no recovery of vision in the affected eye, but enucleation was not deemed necessary, and the patient was eventually discharged 10 days after the initial admission with preserved globe.

Images in a 52-year-old woman with endophthalmitis, 5 days after intravitreal and systemic antibiotic therapy was initiated.
A, Axial precontrast T1-weighted image shows relative hyperintensity of the right vitreous body and periscleral tissue that is isointense with the brain. The findings are comparable to Fig 1A.
B, Axial T2-weighted image at the same level again shows periscleral hyperintensity surrounding the right globe. The right vitreous body and the uveal tract are now of subtle heterogenous appearance with a relative decrease in signal intensity.
C, Corresponding axial contrast-enhanced T1-weighted image again shows uveal tract and perisclearal enhancement on the right.
D, Corresponding axial FLAIR image reveals diffuse heterogenous appearance and relative hyperintensity of the right vitreous body. Periscleral tissue of similar signal intensity is also seen.
E, Axial DWI at a similar level demonstrates some relative hyperintensity of the right globe, far less prominent compared with the pretreatment image, Fig 1E.
F, Corresponding axial ADC map shows hypointensity consistent with decreased diffusion in the periphery of the right globe, which is now slightly higher than in the brain parenchyma. This area is of increased signal intensity in comparison with the pretreatment image, whereas the central portion is of slightly lower signal intensity, which is not conspicuous. The mean ADC value in the anterior and medial aspect measured 927 × 10-6 mm2/s, and in the central portion 2336 × 10-6 mm2/s. The mean ADC value in the left globe was 2813 × 10-6 mm2/s.
Discussion
Acute endophthalmitis is an ophthalmologic emergency, and a high clinical suspicion is necessary for prompt diagnosis. Although some of the classic clinical features may help identify patients with endophthalmitis, most are nonspecific and diagnosis remains difficult, especially in light of its low incidence (1). This is especially true for endogenous endophthalmitis, which usually occurs in chronically ill patients. Because of the rapid advance of medical technology, a longer life span of chronically debilitated patients, and a rising prevalence of long-term intravenous access, the disease may become more common in clinical practice (1, 3). Early diagnosis and prompt aggressive treatment are imperative if vision loss is to be avoided.
The poor visual prognosis, however, has not improved in more than half a century, at least in part because most patients are initially misdiagnosed (1). The most common misdiagnosis in adults is acute, noninfectious, anterior uveitis; in children, it is retinoblastoma. Effective treatment is generally delayed by 2 days or more, and it appears to be >9 days on average (1). In approximately two-thirds of affected patients, vision is eventually worse than counting fingers and about one-quarter of eyes require evisceration or enucleation (1). The mortality rate associated with endogenous endophthalmitis is significant, at least 5%, and it was found to be 32% in a prospective study (1).
Currently, the diagnosis of endophthalmitis is based almost exclusively on history and physical examination, but it mimics several common ophthalmic conditions and may be clinically indistinguishable from anterior uveitis. Also success of treatment may not be clinically evaluated, and the patients remain hospitalized for a week or longer to ensure early recognition of potential intracranial extension of the infectious process. Any imaging technique that may expedite or assist in the diagnosis would be useful, because adequate and effective treatment is based on prompt administration of intravenous and intravitreal antibiotics.
MR imaging with DWI and ADC mapping sequences has become an important imaging tool for the evaluation and diagnosis of acute stroke (6), as well as to distinguish between brain abscess and cystic neoplasm (7, 8). The use of DWI has been extended to the evaluation of spinal infection as well (9, 10). To the best of our knowledge, there have been only 2 reports of MR imaging findings in endogenous endophthalmitis but none discussing the use of DWI, ADC maps, or FLAIR sequences (4, 5). This case report demonstrates the utility of MR imaging with DWI, ADC, and FLAIR sequences in cases of endophthalmitis. We have shown that this is not only useful in diagnosis, but can also demonstrate treatment response, which is almost impossible to assess clinically. We propose that the imaging findings reflect positive treatment response by revealing a decrease in the inflammatory process as evidenced by decreasing DWI signal intensity with corresponding increase in mean ADC values. This pattern has been described recently for treatment response of cerebral abscesses (11). If MR imagings with DWI, ADC, and FLAIR sequences are performed to confirm or establish the diagnosis, or at the initiation of therapy, repeat imaging can be employed to assess treatment response. This may lead to earlier patient discharge and consequently reduced cost.
FLAIR has been only rarely used for evaluation of ocular pathology (12), but we believe it could be very advantageous because of its combination of T2 weighting and nulling of water signal intensity, which leads to radically improved conspicuity of intraocular lesions. DWI and ADC appear to be very sensitive for intraocular infectious processes, similar to the brain, and, as more recently shown, the spine. These imaging techniques may also prove useful for detection of infections in other parts of the body.
References
- Received August 9, 2004.
- Accepted after revision October 7, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}