
Abstract
BACKGROUND AND PURPOSE: To describe the results of transvenous embolizations of cavernous dural arteriovenous fistua (cDAVF) with an emphasis on identifying the incidence, characteristics, and management strategies associated with the complications of transvenous embolization of cDAVFs.
METHODS: Fifty-six consecutive patients who were treated by transvenous embolization for cDAVFs were reviewed. The approach routes, angiographic results, complications, and clinical outcome were assessed.
RESULTS: Retrograde inferior petrosal sinus (n = 36), transfacial vein (n = 7), transcontralateral intercavernous sinus (n = 4), and direct superior ophthalmic vein (n = 3) approaches were used. Angiographic results showed complete occlusion (n = 29), nearly complete occlusion (n = 13), and incomplete occlusion (n = 14). Complications associated with the procedures were cranial nerve palsy (n = 6), venous perforation (n = 3), and brain stem congestion (n = 2). The cranial nerve signs resolved with conservative treatment. Venous perforations were managed by coil embolizations at the site of the tear with no significant neurologic sequelae. One case of brain stem congestion resulted in hemiplegia after conservative treatment. The other case showed venous congestion as a result of rerouting of the shunted flow after venous embolization that was successfully managed by covered stent deployment for occlusion of the residual feeders. Clinical follow-up data were available in 46 patients. Complete resolution or improvement of symptoms was seen in 42 patients (91%).
CONCLUSIONS: Cavernous DAVFs may be effectively treated by transvenous embolization. However, the procedure can be associated with various complications, some of which can potentially result in significant morbidity. Prompt diagnosis of the complications with appropriate management strategies is mandatory for a safe procedure.
Dural arteriovenous fistulas (DAVFs) are abnormal arteriovenous shunts developing on the dura mater, usually within or near the walls of a dural sinus.1 The transverse sigmoid sinus and the cavernous sinus are known to be the most frequent sites of occurrence; the cavernous sinus is the most frequent in the Asian literature.2–4 The symptoms of these lesions depend on the location of the shunt, the type of venous drainage, and the flow characteristics.1 Cavernous DAVFs (cDAVFs) may show signs of orbital hypertension—which include glaucoma, pulsatile exophthalmos, chemosis, conjunctival injection, and episcleral venous dilation—central nervous system symptoms, or bruit according to the venous drainage pattern.5,6
The decision to treat cDAVFs depends mostly on the drainage pattern and the symptoms of the lesion. Some of these lesions may even regress spontaneously.7–9 However, DAVFs that are associated with persistent cortical venous drainage are known to yield an annual mortality rate of 10.4%.10 Thus, higher risk lesions associated with cortical venous drainage, progressive visual loss, neurologic deficits, hemorrhage, and cases presenting with intolerable diplopia, severe headache, and severe cosmetic disfigurement justify endovascular intervention.11–13 The treatment options for cDAVFs include manual compression of the ipsilateral carotid artery, transarterial embolization of feeder vessels, and transvenous embolization. The manual carotid compression may be performed in patients with a benign type of cDAVF. This maneuver is simple and allows thrombus formation in the cavernous sinus by arterial and venous occlusion.14 Transarterial feeder vessel embolizations may be performed for the cDAVF lesion but are frequently inadequate for definitive treatment. Some lesions derive meningeal supply from branches of the intracranial circulation that cannot be accessed or embolized safely. In some cases, a plethora of external carotid artery meningeal supply may not be satisfactorily accessed.5
Transvenous embolization is generally considered to be an effective method of treatment for cDAVFs.5 Since the initial reports of transvenous embolization for carotid cavernous fistulas, improvement in endovascular techniques and materials has allowed alternative choice of routes in addition to the inferior petrosal sinus (IPS) for navigation of the microcatheter and microwire into the targeted cavernous sinus.15,16 However, there are potential complications associated with this procedure, and there is a lack of detailed information concerning the incidence, manifestations, and management of such complications in the literature.
In this study, we reviewed a relatively large homogenous group of cDAVFs treated in a single institution. The purpose of this study was to describe the results of transvenous embolization of cDAVF with an emphasis on identifying the incidence, characteristics, and management strategies associated with the complications of transvenous embolizations of cDAVFs.
Materials and Methods
We conducted a retrospective analysis of patients who underwent transvenous embolizations for cDAVF between January 1997 and September 2005. The imaging findings and medical records of 56 consecutive patients were reviewed. The approach routes, angiographic results, complications, and clinical outcome were assessed. Institutional review board approval was obtained for this retrospective study with waiver of informed consent.
Bilateral selective internal carotid artery (ICA), external carotid artery, and common carotid artery angiography were performed in all patients for assessment of the feeding arteries, the fistula sites, and the venous drainage patterns. Patients with higher risk drainage patterns, such as cortical venous drainage, worsening of visual acuity, or intolerable symptoms, were selected for endovascular treatment. In general, the embolization procedures were performed under local anesthesia, and the transvenous approach was initially attempted through the ipsilateral IPS regardless of its angiographic patency. A 5F guiding catheter was navigated to the internal jugular vein, and a microcatheter with a microwire was navigated coaxially to the cavernous sinus via the IPS. In some cases, a diagnostic angiographic catheter was positioned in the external carotid artery to delineate the target site for occlusion with the road-mapping technique.
If the ipsilateral IPS approach was not successful, the contralateral intercavernous sinus, facial vein, or the direct superior ophthalmic vein (SOV) routes were also used. For the direct SOV approach, the vessel was exposed by the neurosurgeon and then punctured. The microguidewire was then carefully introduced and advanced to the cavernous portion, followed by the microcatheter.
All transvenous embolizations were performed with fibered and/or electrically detachable coils under real-time digital subtraction fluoroscopic mapping. Adjunctive transarterial embolizations were also performed with polyvinyl alcohol (PVA) particles or n-butyl-cyanoacrylate (n-BCA) in cases of remnant shunt or failed transvenous approach.
Angiographic complete occlusion was defined as complete occlusion of the shunt, nearly complete occlusion as small residual stagnant shunt that was considered likely to thrombose, and incomplete occlusion as the presence of residual shunt. Complete and nearly complete occlusions were considered successful angiographic results.
The patients were generally followed by clinical evaluations on a 2–3 month basis and in between upon changes or deterioration in symptoms. Additional imaging studies such as brain CT or MR were performed during the follow-up period in complicated cases. Angiographic reevaluation was performed if changes or deterioration of symptoms believed to be related to the DAVF had occurred.
Clinical improvement was defined as cure or improvement of the symptoms related to the lesion, no improvement as no changes or aggravation of symptoms, and recurrence as newly developed symptoms related to the lesion during follow-up.
Results
The characteristics of the patients are summarized in Table 1.
Characteristics of patients and results of transvenous embolizations
Overall, the transvenous approach to the cavernous lesion site was successful in 50 cases (89.3%). Ipsilateral IPS approach was successful in 36 cases (64%). Other accessible venous approaches were also used, including the transcontralateral intercavernous sinus (n = 4), and the facial vein (n = 7). Direct surgical SOV puncture approach was also performed in 3 cases. Adjunctive transarterial embolizations for residual shunts after transvenous embolizations were performed in 11 cases (19.6%). Target site access through any available venous route was unsuccessful in 6 cases (10.7%), and transarterial embolizations using PVA and n-BCA were performed for these cases. Angiographic complete (n = 29) and nearly complete (n = 13) occlusions were achieved in 29 and 13 cases, respectively, for an angiographic success rate of 75% (n = 42). Clinical follow-up data were available in 46 patients (mean 13 months; range, 1 week to 7 years). Complete resolution or improvement of symptoms were seen in 42 patients (91%), no improvement of symptoms in 2 patients, and recurrent symptoms in 2 patients.
Overall, complications associated with the procedure were observed in 11 cases (19.6%). The most common complication associated with the procedure was cranial nerve palsy (n = 6, 10.7%) (Table 2). Abducens nerve palsy (n = 5) was the most common pattern. In general, the symptoms relieved within a few days to weeks with conservative treatment. However, 1 patient complained of mild residual diplopia as a result of abducens nerve palsy after 42 months of follow-up.
Characteristics of cranial nerve palsy caused by transvenous embolizations of the cavernous sinus
A case of severe trigeminal neuralgia was also observed in which the patient complained of severe ipsilateral upper toothache during the venous coil embolization procedure. The patient recovered from the pain after 3 days of conservative analgesic treatment.
The second most common complication associated with the transvenous embolization procedure was venous perforation (n = 3, 5.4%). The perforations occurred during careful navigation with the microwire and microcatheter in the occluded dural sinuses or multicompartmented cavernous sinus. The sites of perforations were the IPS (n = 1) and the cavernous sinus (n = 2). The perforations were identified by opacification of the brain parenchymal outlines on slow careful contrast injection through the microcatheters after suspected venous tear. In all cases, the microcatheter was not completely withdrawn from the suspected perforation site. These perforated sites were embolized with coils. The patients complained of headache and nausea but soon resolved during follow-up without neurologic sequelae in all cases.
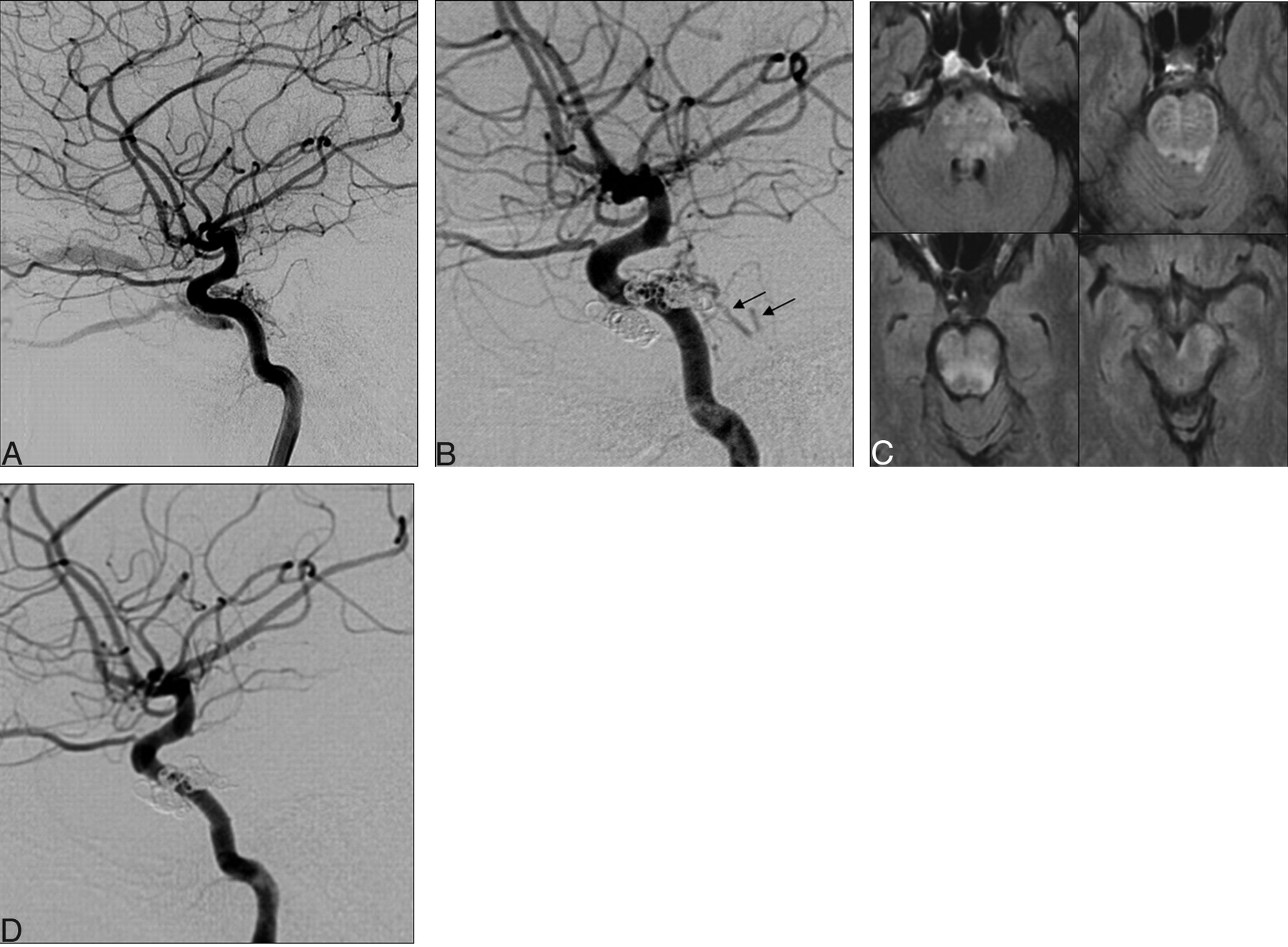
Venous congestion after transvenous coil embolizations occurred in 2 cases (3.6%). In 1 case, the patient developed dysarthria, decreased gag reflex, and hemiparesis on the evening of the treatment. Follow-up CT and repeat angiogram revealed venous congestion of the posterior fossa. These symptoms were managed conservatively, but the patient did not recover from the hemiparesis, resulting in permanent morbidity (follow-up, 7 years). The other patient (Fig 1) underwent aggressive eradication of the small residual meningohypophyseal feeders with covered stent grafts (Jomed International, Helsingborg, Sweden; 3.5/12 mm [right ICA] and 4/16 mm [left ICA]) after 3 days of antiplatelet premedication. The patient was placed on aspirin (Astrix; 100 mg/day for 3 months) and clopidogrel (Plavix; 75 mg/day indefinitely) after the treatment. The patient’s symptoms showed resolution, and a conventional angiogram at 2-month follow-up revealed persistent occlusion of the meningohypophyseal feeders with patent bilateral stent grafts. Small reopening of the left middle meningeal and artery of foramen rotundum feeders were successfully embolized with liquid coil, n-BCA, and PVA. The patient remained symptom-free after 8 months of follow-up.

A 60-year-old man presented with symptoms of decreased visual acuity, exophthalmos, and chemosis of the left eye of 1 month’s duration.
A, Initial left ICA angiogram revealed an arteriovenous shunt at the left cavernous sinus with drainage into the superior ophthalmic and inferior ophthalmic veins.
B, Transvenous coil embolization of the left cavernous sinus was performed via a left SOV approach, resulting in nearly complete occlusion of the target sinus with slow but stagnant flow in the anterior pontomesencephalic veins (arrows).
C, Fluid-attenuated inversion recovery images of the patient after he developed mild dysarthria shows congestion of the brain stem. Bilateral graft stents were deployed for occlusion of the residual meningohypophyseal feeders.
D, Poststent left ICA angiogram shows complete occlusion of the residual shunt.
Discussion
The results of this study show the efficacy of transvenous embolizations for cDAVF in a large single series consisting of 56 cases. In addition, the incidence, characteristics, and management strategies for complications associated with the procedure have been presented.
The results of our study show that the transvenous access of the target sinus was successful in 89% (n = 50) of the cases. The ipsilateral IPS selection was successful in 64% (n = 36) of cases. Other routes of navigation included the contralateral cavernous sinus (7%, n = 4), facial vein (13%, n = 7), and the SOV after surgical exposure (5%, n = 3). The major routes available for access to the cavernous sinus include: anteriorly, the SOV and facial vein; superiorly, superficial middle cerebral vein and sphenoparietal sinus; posteriorly, the petrosal sinuses; and inferiorly, the pterygoid plexus.17–21 Detailed knowledge of the anatomy in addition to new endovascular equipment suitable for navigation into small connecting channels is essential for a successful treatment. Using this multichannel approach, we were able to achieve complete or nearly complete occlusion of the fistula in 75% (n = 29 and 13, respectively) with cure or improvement of symptoms in 91% (n = 42) on clinical follow-up. These results seem compatible with other smaller series that had reported similar anatomic and clinical cure rates of 71%–89% and 77%–96% and show the efficacy of transvenous embolizations for cDAVFs.13,22–24
A few articles are available on the complications of transvenous embolization of cDAVF. Most are case reports or small, heterogenous case series with a limited number of complications.12,13,22,23,25–28 From a single center experience of 56 cases of transvenous cDAVF, we were able to identify the incidence of various complications, characteristics, and the management strategy.
The total incidence of complications associated with the procedure was high (19.6%, n = 11); however, most were transient morbidities. Only a single case (1.8%) showed serious permanent deficit. The low incidence of permanent morbidity despite the high incidence of total number of complications may be attributed to the vigilant detection and management of the complications.
Six cases (10.7%) showed newly developed cranial nerve signs after transvenous coil embolizations. The reason for cranial nerve signs after transvenous embolization may be due to progressive thrombosis of the cavernous sinus, mass effect by the coil, and direct injury of the nerve by the coil or microwire/microcatheter.23,29 In our series, the mean number of coils used for embolization was 16.7 (range; 4–37 coils). Overpacking of the cavernous sinus may have been a cause of the transient cranial nerve symptoms in most cases; however, paradoxical worsening as a result of thrombosis of the cavernous sinus may be have been the cause in the 2 cases embolized with only 4 coils. The reason for abducens nerve predilection is unclear but may be because the occulomotor, trochlear, ophthalmic, and maxillary nerves are usually located in the lateral wall of the cavernous sinus, whereas the abducens nerve is located just lateral to the internal carotid artery. This anatomic disposition may allow further vulnerability of the abducens nerve to the stretching and mass effects of the coil or thrombus within the sinus.30 Even though permanent deficits have been reported, the management of these complications by conservative analgesics and steroid therapy resulted in good outcome.23
The rate of venous perforations (5.4%, n = 3) in our series seems to be higher than any in other case series.12,13,22,23 In the other case series, newly developed subarachnoid hemorrhage after transvenous embolization may have been due to unrecognized venous perforation during the procedure.13,23,28 All cases of venous perforations occurred during careful blind navigation in the occluded sinuses. The results of our study show that perforations can occur despite use of supple microwires and microcatheters. The hemodynamic stresses of the shunted arterial flow leaking into the subdural/subarachnoid spaces may become a potential source of significant morbidity if undetected or untreated. Direct surgical exposure and obliteration of the perforation with n-BCA has been reported for management of such complications.28 However, according to our series, immediate recognition and coil embolization at the site of perforation, followed by occlusion of the arteriovenous shunt to reduce the hemodynamic stress, seem to be sufficient for management of such complications.
Two cases (3.6%) of venous congestion developed after transvenous embolization of the cavernous sinus. Other reports have shown rare cases of brain stem congestion in cDAVF caused by shunted flow into the posterior fossa.25,31 Venous congestion by rerouting to the pontomesencephalic veins occurred after coil embolization in our cases, despite nearly complete occlusions of the shunts after embolization. Such venous rerouting is a known complication in cases of transvenous embolization in other dural sinuses. It is important to avoid simple trapping or partial embolization of the involved dural sinus, because this can lead to diversion of shunt flow into the normal cerebral venous pathways and ultimately result in conversion of the DAVF into a more dangerous and aggressive disease.5 However, transvenous coil embolization of the complex and septated cavernous sinus may sometimes be difficult and could result in unintended dangerous rerouting of the shunt. Because of the small caliber and the unusual anatomy of the brain stem venous drainage in our 2 cases, recognition of such potential complication was difficult. Both patients developed neurologic symptoms after the completion of the procedure. In the first case, these symptoms were treated by conservative management resulting in permanent morbidity. In the second case, however, the newly developed neurologic symptom was recognized early as a possible sign of venous congestion. A repeat angiogram revealed flow in the small feeders from bilateral meningohypophyseal trunks that were diverted to the pontomesencephalic veins. These feeders were considered to cause venous hypertension and were aggressively occluded by deploying covered stents in the ICA. Experience from the cardiology literature has shown the efficacy of polytetrafluoroethylene (PTFE)-covered stents in occlusion of coronary perforations and aneurysms.32–34 In our cases, these stents were effective in occluding the arterial feeders arising from the ICA by providing a mechanical barrier and also in ameliorating the harmful consequences of brain stem congestion. Stent thrombosis and restenosis after covered stent deployment are a major concern. Previous studies have reported subacute thrombosis and restenosis rates of 5.7% and 24%–31.6%, respectively, after covered stent implantation for coronary aneurysm, perforation, saphenous vein graft, and in-stent restenosis.32,35,36 The restenosis rate after covered stent deployment in nonatherosclerotic parent vessels are unknown; however, the rates seem lower in cases of native, noncomplicated coronary vessels.32,34 Therefore, the future risk for stenosis or occlusion in our case of stent graft in the nonatherosclerotic ICA may be more favorable. Although antiplatelet medications contradict the objective of occluding the shunt, we believe that prolonged medication is necessary for prevention of thrombosis and stenosis of the stent site. In addition, mid- and long-term angiographic evaluations are necessary for detection of not only stent stenosis but also reopening of the feeder vessels.
Conclusion
Cavernous DAVFs presenting with higher risk pattern such as cortical venous drainage and intolerable symptoms may be effectively treated by transvenous embolization. However, transvenous embolization of the cavernous sinus can be associated with various complications, some of which can potentially result in significant morbidity. Prompt diagnosis of the complications with appropriate management strategies is mandatory for a safe procedure.
References
- Received January 23, 2006.
- Accepted after revision February 21, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Additional outlet occlusion as an important factor in avoiding retreatment after transvenous embolization for cavernous sinus dural arteriovenous fistulas
- Endovascular Management of Intracranial Dural AVFs: Transvenous Approach
- Newly occurring cranial nerve palsy after endovascular treatment of cavernous sinus dural arteriovenous fistulas
- Cannulation of Occluded Inferior Petrosal Sinuses for the Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistulas: Usefulness of a Frontier-Wire Probing Technique
- Augmented 3D venous navigation for neuroendovascular procedures
- Transvenous embolization of dural carotid cavernous fistulas: the role of liquid embolic agents in association with coils on patient outcomes
- Dural carotid cavernous fistulas: endovascular treatment and assessment of the correlation between clinical symptoms and the Cognard classification system
- Transorbital superior ophthalmic vein sacrifice to preserve vision in ocular hypertension from aseptic cavernous sinus thrombosis
- Mid- and long-term outcomes of carotid-cavernous fistula endovascular management with Onyx and n-BCA: experience of a single tertiary center
- Transorbital superior ophthalmic vein sacrifice to preserve vision in ocular hypertension from aseptic cavernous sinus thrombosis
- Onyx 18 embolisation of dural arteriovenous fistula via arterial and venous pathways: preliminary experience and evaluation of the short-term outcomes
- Turn-Back Embolization Technique for Effective Transvenous Embolization of Dural Arteriovenous Fistulas
- Long-Term Outcome after Coil Embolization of Cavernous Sinus Arteriovenous Fistulas
- Transvenous Embolization of Dural Carotid Cavernous Fistulas: A Series of 44 Consecutive Patients