
Abstract
BACKGROUND AND PURPOSE: Iodine deficiency and hypothyroxinemia have a negative effect on the development of the central nervous system during fetal and early postnatal life. MR spectroscopy is a sensitive technique for detecting the changes of brain metabolites in various neurodevelopmental disorders. By using MR spectroscopy, we aimed to show the decrease in N-acetylaspartate (NAA) levels in neonates with hypothyroidism who were born in iodine-deficient areas and its normalization with early thyroxine therapy.
METHODS: Eight congenital hypothyroid and 8 healthy full-term neonates were chosen as study and control groups, respectively. Serum thyroid hormones and median urinary iodine concentration of the neonates and their mothers were measured. Measurements of NAA, choline (Cho), and creatine (Cr) were made in frontal white matter, parietal white matter (PWM), and the thalamus with MR spectroscopy, first at 5–7 days of life and after 8 weeks of thyroxine therapy in the study group and at the same time in the control group.
RESULTS: The patient group had significantly lower NAA/Cr ratios in PWM and the thalamus (P < .05, for each), whereas the difference between Cho/Cr ratios of the 2 groups before therapy was not significant. After 8 weeks of thyroxine therapy, measurements did not show significant difference between study and control groups.
CONCLUSION: MR spectroscopy performed in neonates with hypothyroidism reveals that intrauterine hypothyroxinemia due to iodine deficiency results in significant decrease in NAA levels in PWM and the thalamus and that the normalization of NAA levels is achieved with early thyroxine therapy.
Thyroid hormones are essential for normal brain development, proliferation of axons and dendrites, synapse formation, gliogenesis, myelination, and regulation of synthesis of specific neurotransmitters beginning from the intrauterine period and extending through 1–2 years of age.1 During pregnancy, both maternal and fetal thyroid hormones are required for normal fetal brain development. Maternal hormones are the main source in the first and second trimester, whereas fetal hormones contribute in the third trimester.2,3 There are many studies indicating that iodine deficiency and iodine-induced maternal and fetal hypothyroxinemia result in impairment of central nervous system (CNS) development during the fetal and early postnatal life. Iodine deficiency is one of the causes of preventable mental retardation, so that if it is severe enough to impair thyroid hormone synthesis during critical periods of brain development, it can induce irreversible brain damage with the clinical consequences of mental retardation and psychomotor disabilities.4,5
Proton MR spectroscopy is a noninvasive tool to investigate the biochemical alterations in neural structures. It is increasingly being used to aid in diagnosis and clinical management. Using MR spectroscopy, we gain quantitative information from various cerebral metabolites, such as amino acids like N-acetylaspartate (NAA), alanine, and glutamate (Glu); amines like glutamine (Gln), choline (Cho), creatine (Cr), myo-inositol, and glucose; and lipids and compounds involved in high-energy metabolism like lactate.6,7 NAA is seen only in neuronal tissue7 and is accepted as a marker for neuronal and axonal integrity, development of synaptic terminals, dendritic arborizations, and myelination.6,8 Cho concentration reflects increased or decreased membrane turnover, and Cr is a marker for brain energy metabolism and used to be an internal reference because of its relatively constant state in metabolic diseases.7 In general, relative concentrations of these metabolites are normally expressed by the peak areas of the corresponding resonances. Determination of the concentration and relative levels of proton-containing metabolites may help in assessing normal and abnormal tissues and their response to therapy.9
Our country has been known to be a mild-to-moderate iodine-deficient area, but still a nationwide screening program for congenital hypothyroidism (CH) has not been initiated. Some regional studies from our country have reported the ratio of CH as 1/2326,10 which is much higher than the ratio of 1/400011 obtained from the worldwide screening programs. That finding is the reason that we measured the NAA, Cho, and Cr levels of the brain metabolites in neonates with hypothyroidism, who were born in iodine-deficient areas, in parietal white matter (PWM), the thalamus, and frontal white matter (FWM) by using MR spectroscopy. We aimed to show the reducing effect of intrauterine hypothyroxinemia on NAA levels, which are neuronal maturation markers, and the normalization of NAA levels after early thyroxine therapy.
Methods
Subjects
Eight full-term neonates with hypothyroidism, 5–7 days of age, born to mothers living in iodine-deficient regions with no iodine supplementation either in the pregestational or gestational period, were included in the study. After diagnosis, these neonates were given thyroxine at a dosage of 10 μg/kg per day. On the other hand, 8 full-term healthy neonates of the same age as the study group were chosen as the control group; their mothers had been using iodine-supplied salt since the pregestational period. All infants included in the study were free of congenital malformations, detectable metabolic or chromosomal disorders, cerebral pathologies, and risk factors for brain injury such as perinatal hypoxia/acidosis or respiratory distress syndrome requiring mechanical ventilation.
Laboratory Examinations
Serum total T4 (TT4), free T4 (FT4), and thyroid-stimulating hormone (TSH) levels of the neonates and serum total T3 (TT3), TT4, and TSH levels of their mothers were measured with chemiluminescent immunometric assay. Normal limits for these values were accepted as follows: TT3, 84–172 ng/dL; TT4, 4.5–12.5 μg/dL; FT4, 0.8–1.9 ng/dL; TSH, 0.4–4 μIU/mL. The estimation of median urinary iodine (MUI) concentration was performed in spot urine samples obtained from all mothers and their neonates 5 days after delivery. Urine specimens were stored at −70°C until required for analysis, and measurements were performed by using the Sandell-Kolthoff reaction.12 Classification of the severity of iodine deficiency in mothers was according to the cutoff points of MUI excretion values; thus, MUI values less than 20 μg/L were considered severe; between 20–49 μg/L, as moderate; between 50 and 99 μg/L, as mild; and greater than 100 μg/L, as adequate, according to World Health Organization (WHO) criteria.13
Sonographic Determination of Thyroid Volumes
Thyroid volume (Tvol) was measured in all neonates and their mothers with sonography by the same radiologist with the same sonographic scanner (7.5-MHz linear transducer, ATL-HDI-5000, Philips Medical Systems, Bothell, Wash), and Tvol (mL) was calculated according to the formula of the ellipsoid model: width × length × thickness × 0.52 for each lobe.14 The total Tvol (TTvol) was the sum of both lobes, and the isthmus volume was not included. In the mothers, goiter was defined when the Tvol was greater than 18.0 mL according to WHO criteria.15,16
MR Spectroscopy
Cranial MR spectroscopy was performed on a 1.5T whole-body imager (Gyroscan Intra Master, Philips, Best, the Netherlands). T1-weighted images (TR, 560 ms; TE, 15 ms) were obtained in the axial and sagittal planes (with 5-mm-thick sections). T2-weighted images (TR, 4530 ms; TE, 100 ms) were obtained in the axial and coronal planes. The routine images were used to identify anatomic structures and to confirm the absence of any structural or signal intensity abnormalities.
Single-voxel spectroscopy was performed in all patients and controls by using a point-resolved spectroscopy sequence (TR, 2000 ms; TE, 136 ms) with 128 averages. Voxel sizes of 15 × 15 × 15 mm were used, and voxels were placed at locations in FWM, PWM, and the thalamus. In the placement of voxels, contamination by gray matter and CSF was avoided. Before MR spectroscopy, shimming was performed to optimize field homogeneity, and water suppression was optimized by using automated routines provided by the manufacturer. The water signal intensity was suppressed by a chemical shift selective saturation pulse. A spectral sweep width of 1000 Hz was used with data size of 1024 points. All data postprocessing was performed with software provided by the manufacturer (Gyroscan ACS-NT; Phillips Medical Systems, release MMR 5461; 1H spectroscopy 1.5 packages). The magnitude spectra were processed automatically by using baseline correction and curve-fitting procedures to determine the resonance areas of NAA, Cr, and Cho. Resonances were assigned as follows: NAA, 2.0 ppm; Cr, 3.02 ppm; Cho, 3.2 ppm. Peak area metabolite ratios (NAA/Cr, Cho/Cr) were calculated.
All of the patients, just before thyroxine therapy, and the control subjects underwent cranial MR spectroscopy study between days 5–7 of life. Cranial MR spectroscopy studies and thyroid hormone measurements were repeated after 8 weeks of thyroxine therapy in the patients and 8 weeks after the first scanning in the control subjects. Cranial MR spectroscopy studies were performed during the normal sleep period of the babies without any application of sedatives, and cotton was placed into external ear orifices for sound isolation during the process. All neonates were protected from the cold MR spectroscopy room and attended by their mothers during the whole MR spectroscopy study. Detailed consent forms of the study were signed by the families of the neonates in both groups, and local ethics committee approval was obtained.
Statistical Analyses
All statistical analyses were performed by using a commercially available SPSS Release 10.0 software package (SPSS, Chicago, Ill). The results are presented as mean ± SD and are shown in Tables 1–3. Comparisons within and between groups were assessed by the Mann-Whitney U test or the Wilcoxon rank sum test. Linear correlations between variables were tested by calculating the Spearman correlation coefficient.
Thyroid hormone levels of the neonates (mean ± SD)
Results
All of the neonates included in the study had normal birth weights. Serum thyroid hormone levels of patients and controls are listed in Table 1. Serum TT4 and FT4 levels of the study group were significantly lower (P < .01 and P < .01, respectively), whereas TSH levels were significantly higher (P < .001) than those of the control group (Table 1). There were also significant differences between the TT3, TT4, and TSH levels of mothers in both groups (P < .05, P < .05, and P < .05, respectively) (Table 2). Patients, after 8 weeks of therapy, and the control group, after 8 weeks of follow-up, had normal levels of thyroid hormones. The borderline elevation of TSH levels, besides increased TT3, near-normal TT4 levels, and increased TTvol, indicated that subclinical hypothyroidism was present in the mothers of the patient group.
Maternal thyroid hormone levels and maternal and neonatal MUI excretions and total thyroid volumes (means ± SD)
MUI excretion of both the neonates with hypothyroidism and their mothers was significantly lower than that of the control groups (P < .01) (Table 2). These decreased levels were accepted as mild-to-moderate iodine deficiency according to WHO criteria. The mean TTvol of the neonates with hypothyroidism was found to be increased (> 2 SD) on thyroid sonography compared with that of the controls (P < .05) (Table 2), whereas no palpable thyroid tissue was detected on physical examination.
The NAA/Cr ratios measured from the PWM and thalamus of the neonates with hypothyroidism were lower than those of the control group before the treatment (P < .05 and P < .05, respectively), but no significant change was obtained in FWM (Table 3).
Spectroscopy findings obtained from PWM, FWM, and thalamus in patients and control subjects (mean ± SD)
The Cho/Cr ratios of the patient group in PWM, the thalamus, and FWM were higher than the corresponding ratios of the control group before the treatment but were also not statistically significant (Table 3). There were significant differences in the NAA/Cr ratios of PWM and thalamic regions of the neonates with hypothyroidism before and after 8 weeks of thyroxine therapy (P < .05) (Table 3). Levels of MUI in both the patients and their mothers were positively correlated with NAA/Cr ratios of PWM and the thalamus before the treatment (r = 0.78, P < .05 and r = 0.85, P < .05, respectively).
At the end of 8 weeks, no significant differences were present between the 2 groups with respect to MR spectroscopy parameters (NAA/ Cr, Cho/Cr) (Table 3). Additionally, all hormonal measurements of the patient group after the treatment and of controls were within the normal limits (Table 1).
Discussion
Iodine is an essential trace element for the synthesis of thyroid hormones, which have been shown to be absolutely necessary for the development of the fetal CNS during intrauterine life, starting from the second half of gestation. Their roles in the first trimester, when fetal cerebral neurogenesis and neural migration mostly take place, have not been defined yet. The importance of maternal thyroid hormones for normal fetal brain development is provided by well-established data showing that developmental brain deficiencies in children with endemic iodine deficiency, in which both the mother and the fetus have a thyroid hormone deficiency, are greater than those in children with only a fetal thyroid hormone deficiency.17 Most studies show that iodine deficiency and maternal-fetal hypothyroxinemia have negative effects on the fetal neural maturation, dendritic arborization, and synaptic formation, and they delay the neuronal myelinization and gliogenesis, which start in the third trimester and speed up in postnatal life. The defects in brain development and neuron maturation are well correlated with the level of iodine deficiency.18 In severe iodine deficiency and resulting maternal and fetal hypothyroxinemia, various degrees of irreversible neuromental developmental defects are present. However, recent studies show that even if clinical maternal hypothyroidism is not found, inadequate thyroxine levels may lead to fetal brain damage.4,5
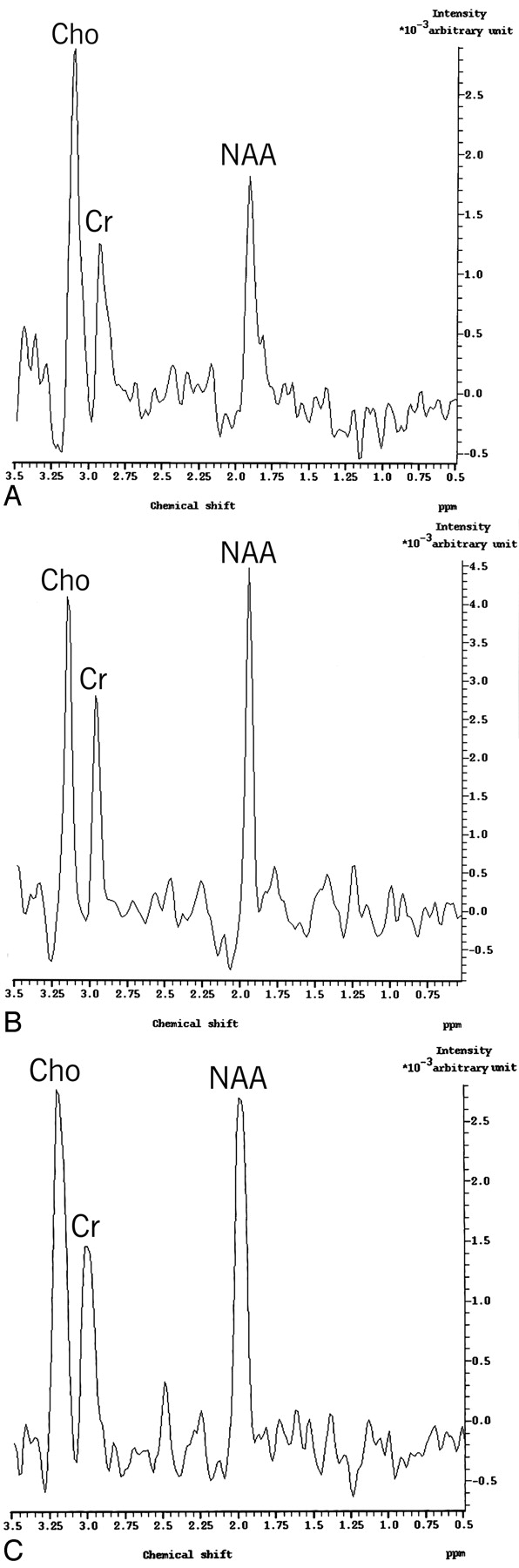
MR spectroscopy provides a noninvasive diagnostic tool for the biochemical characterization of pathophysiologic processes in the brain. Therefore, we used MR spectroscopy to detect the changes in brain metabolites of the neonates with hypothyroidism before and after thyroxine replacement therapy and compared them with those of normal neonates. In this study, NAA, Cho, and Cr levels were measured in the first week of life in the neonates with hypothyroidism born in iodine-deficient regions. The changes in these parameters after 8 weeks of thyroxine treatment were detected again (Fig 1).

A, MR spectrum (TR, 2000 ms; TE, 136 ms) obtained from PWM before treatment in the patient with hypothyroidism. B, Eight weeks after thyroxine therapy in the same patient. C, Five days of age in the control subject.
NAA is the most sensitive CNS metabolite because it is almost exclusively present in the CNS, specifically in pyramidal neurons, dendrites, and axons and so is called a neuronal marker.6,8 Because it is a neuroaxonal marker, abnormalities of neuronal structures, like reduced neuronal attenuation or viability, lead to reductions in NAA. Therefore, it is an important predictor of neuronal dysfunction.19 Because of the importance of mitochondrial energy state in the synthesis of NAA, cellular dysfunction due to impairment of mitochondrial energy metabolism can cause more marked reductions in NAA levels than neuronal loss.20,21 An age-dependent increase of the NAA levels in cerebral gray and white matter with normal brain development has been found especially during the first 3 years of life.22,23 This increase does not reflect a parallel increase in the number of neurons because neuronal proliferation ends before birth. Therefore, the observed changes in the concentration of NAA during normal brain maturation, mediated by many factors including thyroxine, might signify the development of synaptic terminals, dendritic arborizations, the increase in axonal diameter, and the progress of myelination.6 Although the exact mechanism by which NAA is related to neuronal functioning is unknown, it has been demonstrated that NAA is an important cellular osmolyte, a storage vehicle for aspartate and glutamate, and a metabolic precursor of the excitatory dipeptide N-acetylaspartyl-glutamate; it may be involved in neuronal-glial signaling, is likely to participate in myelin formation, and serves as a molecular pump.24
Although mothers of the neonates with hypothyroidism in our study had no clinical hypothyroidism, the borderline elevated TSH, near-normal TT4, elevated TT3, increased TTvol, and decreased MUI levels suggested that they had subclinical hypothyroidism. NAA/Cr ratios of PWM and thalamic regions were found to be lower in the neonates with hypothyroidism before the thyroxine treatment, which can be explained by inadequate exposure of the neonates to thyroid hormones during the intrauterine period due to subclinical hypothyroidism of their mothers. Another acceptable explanation would be that in the untreated state, there is cerebral hypometabolism leading to a diminished synthesis of NAA by viable neurons. With adequate thyroxine therapy, eumetabolic state, which is able to increase in the synthesis of NAA by the same neurons, is achieved.25 Neuronal maturation and myelinization process are rapidly progressive in neonates. Early thyroxine treatment results in better development of neurons and cognitive functions in the neonates with congenital hypothyroidism. We found no difference between the NAA/Cr ratios of the patients after 8 weeks of thyroxine treatment and those of controls; therefore, this finding shows that the changes in NAA levels are reversible with early and adequate thyroxine treatment (Fig 1A, -B).
In our study, the MUI excretion was low in both the neonates with hypothyroidism and their mothers; and in addition to this finding, decreased thyroid hormones and enlarged TTvol observed in this group reflect iodine deficiency. The positive correlation of NAA/Cr in the PWM and thalamus regions with the MUI excretion of neonates with hypothyroidism and their mothers reveals the possibility of detecting the negative effects of iodine deficiency and maternal or fetal hypothyroxinemia on brain development with MR spectroscopy.
In proton MR spectroscopy, Cho is a composite peak, which has contributions from free Cho, phosphocholine, and glycerophosphocholine. The major part of Cho is present as a polar head group of the lipids in membranes and myelin, so it is accepted as a marker of membrane turnover.26 Myelin in the neonatal brain is rich in Cho-containing compounds. However, with maturation, the concentration of Cho declines, and myelin is largely composed of galactolipid and sphingomyelin. Therefore, the increase in the Cho/Cr ratio might point to an inability to properly incorporate Cho-containing molecules into myelin. Also, loss or disruption of normal myelin increases the level of Cho-containing compounds. The increase in Cho/Cr ratios of lately diagnosed hypothyroidism and normalization of this ratio with thyroxine treatment reveal the importance of thyroid hormones on myelin maturation.25,27 In our study, the Cho/Cr ratios of the neonates with hypothyroidism were higher than those in the control group but with no statistical significance. This finding can be explained by the early stages of the myelinization process in our patients, which starts in the last trimester and continues in the postnatal first year. On the other hand, we can consider that nonsevere iodine deficiency and intrauterine hypothyroxinemia do not significantly affect the myelinization process in the fetal period and first week of life. The Cho/Cr ratios of our patients could probably be significantly higher than those of the control group if they were not diagnosed this early. After the treatment, there was no difference between 2 groups, whether statistically significant or not.
There are a few studies in the literature that were performed on children not diagnosed earlier with hypothyroidism.28 In 1 of them, the NAA/Cr ratio was found to be lower and the Cho/Cr ratio, to be higher than that in the control group in 3 children not diagnosed earlier with congenital hypothyroidism at the thalamic and cerebellar regions before the treatment.25 In the same study, the normalization of these values was achieved after 6 weeks of thyroxine treatment. In an another study, 5 untreated patients with congenital hypothyroidism, between 6 and 15 years of age, had increased Cho/Cr ratios before treatment, and there were no significant differences between the study and the control groups after 6 weeks of thyroxine treatment.26
Conclusion
In this study, NAA, Cho, and Cr levels were measured by using MR spectroscopy in neonates with congenital hypothyroidism born in iodine-deficient areas. MR spectroscopy study shows that maternal and fetal hypothyroxinemia due to iodine deficiency results in significant decrease in NAA levels, without any changes in Cho, and that the normalization of NAA levels is achieved with early thyroxine therapy. In this way, it has been shown that the decrease in NAA levels, which can be determined by MR spectroscopy, is an essential parameter indicating intrauterine hypothyroxinemia–related neuronal damage.
References
- Received December 16, 2005.
- Accepted after revision February 3, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.