
Abstract
SUMMARY: A 2-year-old girl who had a 3-day history of swelling in her right eye presented with a case of intraocular ectopic lacrimal tissue. MR imaging findings and possible causes of the ectopic lacrimal tissue in the globe, including embryology, are reviewed. The differential diagnoses of other intraocular masses and the imaging features that can be of help in making a diagnosis are also discussed.
Ectopic lacrimal tissue has been most frequently described in the orbit or on the ocular adnexa, such as the eyelid, conjunctiva, tarsal plate, cornea, and even under the nasal mucosa, whereas intraocular growth is an extremely rare phenomenon.1–18 Puech2 described the first report of ectopic lacrimal tissue within the globe as adenoma of the choroids in a female adult.
In this report, we present an unusual case of ectopic lacrimal tissue in localized to the globe. The CT and MR findings and possible embryologic causes for ectopic lacrimal tissue are reviewed. Imaging features that differentiate this entity from other intraocular masses are also discussed.
Case Report
A 2-year-old girl presented with a 3-day history of swelling in her right eyelid. Physical examination revealed redness and tenderness in her right eyelid. There was a choroidal mass in the supertemporal portion of right eye. The appearance of right optic fundus was normal, and the intraocular pressure was normal.
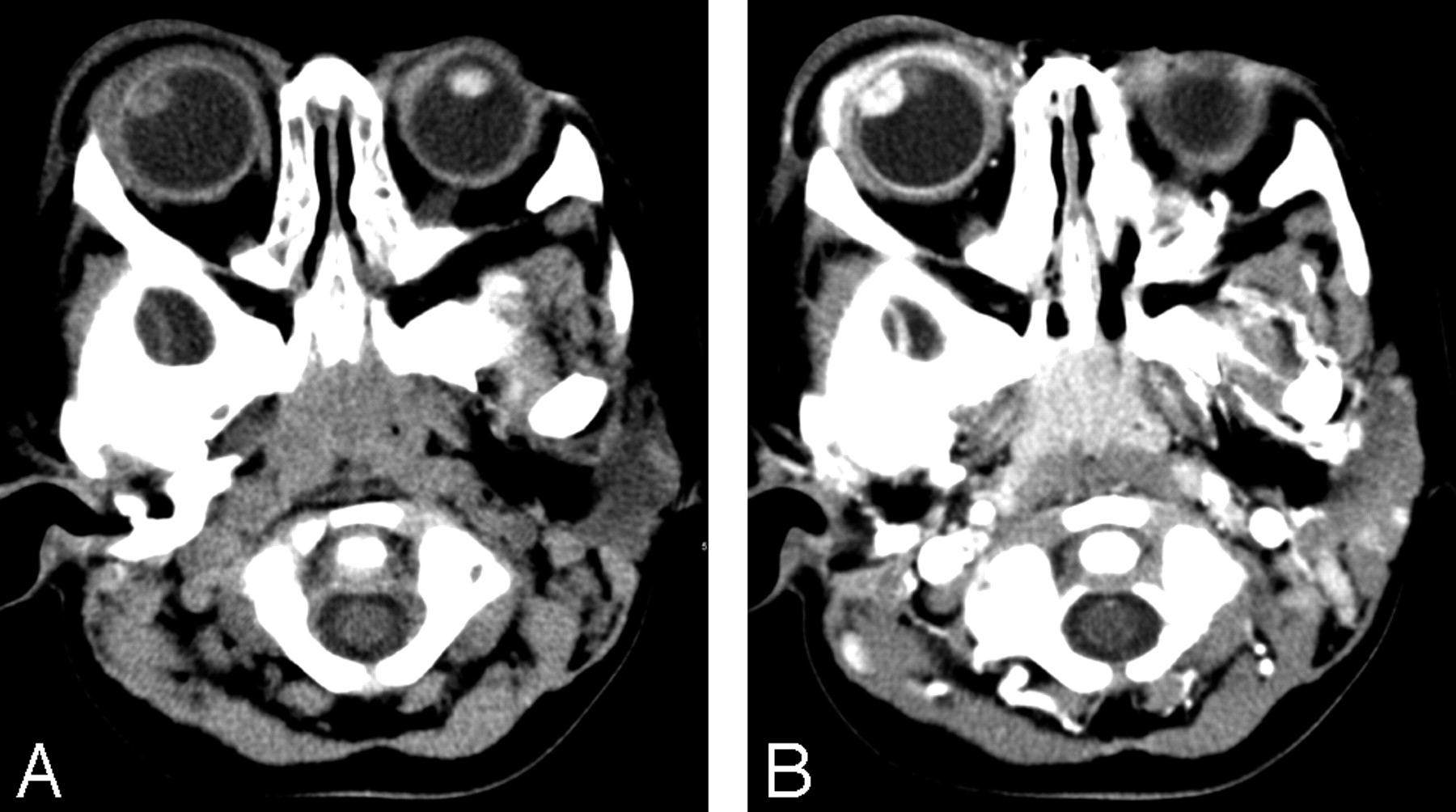
Axial precontrast and postcontrast enhanced CT scans revealed an 8-mm circumscribed ovoid enhancing mass in the superolateral portion of right eye (Fig 1). Swelling of soft tissue in right preseptal area, right eyelid, and ipsilateral lacrimal gland was consistent with orbital cellulitis and lacrimal adenitis. Postcontrast enhanced CT scans showed enhancement of right uvea, sclera suggesting scleritis, and uveitis.

A, Precontrast axial orbital CT revealed a soft tissue attenuation ovoid mass in the superolateral portion of right eye.
B, Postcontrast axial orbital CT scan showed intense enhancement of an ovoid mass. Swelling in soft tissue around right preseptal area and ipsilateral lacrimal gland suggested orbital cellulitis with lacrimal adenitis.
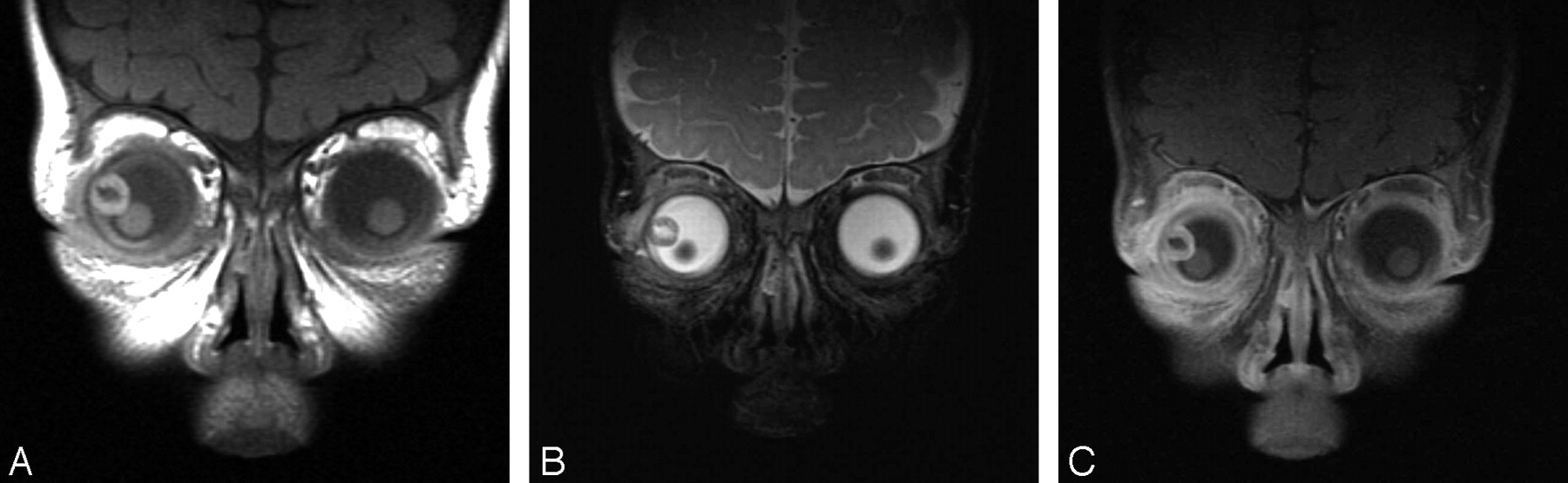
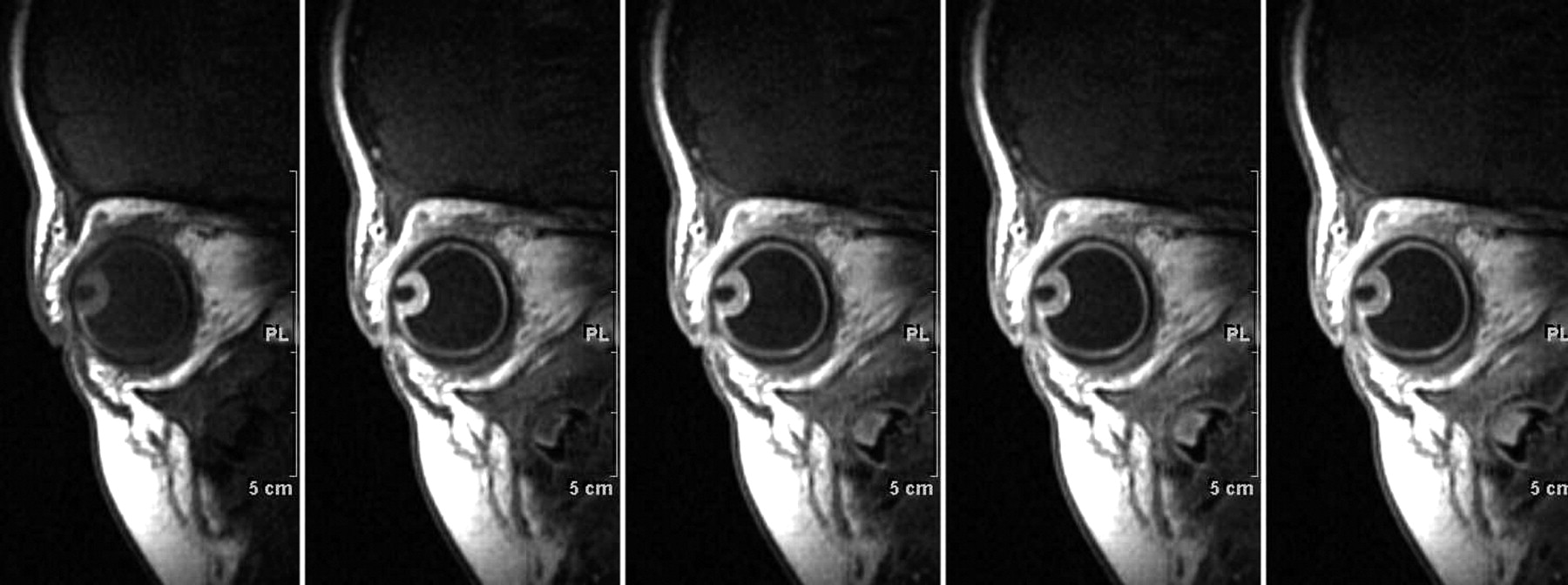
MR imaging showed a circumscribed ring-enhancing mass in the superolateral aspect of right lens (Fig 2). In comparison with the vitreous, the mass revealed slightly high signal intensity on T1-weighted imaging (T1WI) (TR, 420; TE, 12; section thickness, 3 mm; FOV, 12 cm) and low signal intensity on T2-weighted imaging (T2WI) (TR, 2900; TE, 90; section thickness, 3 mm; FOV, 12 cm). Gadolinium-enhanced T1-weighted MR images (TR, 630; TE, 12; section thickness, 3 mm; FOV, 12 cm; gadolinium-DTPA, 2 mL) showed homogenous strong enhancement in peripheral portion of mass. The central portion of mass had low signal intensity on T1WI and high signal intensity on T2WI. Dynamic enhanced T1-weighted MR images (TR, 300; TE, 20; pre-enhanced, immediately; and 1–2-3 minutes after enhancement) showed early and homogenous strong enhancement in the peripheral portion of mass (Fig 3). The diagnosis of intraocular mass, based on the CT and MR images, was uveal hemangioma.

T1- and T2-weighted MR images revealed a circumscribed ringlike mass in superolateral aspect of right eye. The central portion of the mass was low signal intensity relative to vitreous on coronal T1WI (A) and high signal intensity on T2WI (B). The peripheral portion of mass revealed slightly high signal intensity on T1WI and low signal intensity on T2WI. Coronal gadolinium-enhanced T1WI (C) showed strong and homogenous enhancement in peripheral portion of mass in continuity with the enhancing uveal tract.

Dynamic enhanced T1-weighted MR sagittal scans showed early and homogenous strong enhancement in the mass.
The patient underwent incisional biopsy of the mass. The pathology was ectopic lacrimal tissue without any malignant feature. Special stain revealed the presence of myoepithelial cells with smooth muscle actin expression along the outside of glands. This feature is consistent with non-neoplastic glands.
Discussion
There have been 91 reported cases of ectopic lacrimal tissue (Table 1).1–18 Intraocular ectopic lacrimal tissue of the globe is rare, with only 14 cases reported.1,2,4–15 In our case, the ectopic lacrimal tissue arose in the ciliary body.
The locations of the reported lacrimal gland tissue
The globe is formed from neuroectoderm of the forebrain, surface ectoderm from the head, mesoderm lying between these layers, and neuronal crest cells.19 The surface ectoderm forms the corneal and conjunctival epithelium, lens, and lacrimal glands.19,20 In human lacrimal gland morphogenesis, the formation of epithelial bud at the level of the superior conjunctival fornix constitutes the onset of glandular development in embryos between 22 and 25 mm.21 In the 5-mm embryo, the choroidal fissure exists in the inferior edge of the optic cup19–20; later, the choroidal fissure closes at the 15-mm stage. Thereafter, the iris and ciliary body complete their development within the globe after the closure of the choroidal fissures.22 Therefore, it is not well understood how lacrimal tissue reaches in the intraocular structures, because the choroidal fissure closes at the 15-mm stage, and the lacrimal gland does not appear until the 25-mm stage.
Some theories have been proposed concerning the origin of the ectopic lacrimal tissue.4–7,12 These include: 1) early aberrant implantation of embryonic cells destined to become lacrimal gland tissue, 2) implantation with surface epithelium during the formation of the lens, 3) pinching off of lacrimal gland buds by closure of the choroidal fissure at the time when they are in proximity, particularly if there is a delay in the closing of the fissure, and 4) intraocular extension of lacrimal tissue along pre-existing scleral defects, which may later close.
Another possible developmental mechanism for the appearance of intraocular ectopic lacrimal tissue is an epithelial-mesenchymal interaction whereby the FGF-10, an inductive signal intensity for the lacrimal gland, acts directly on the conjunctival epithelium to stimulate proliferation.23 In a study by Govindarajan et al, transgenic mice studies show that misexpression of FGF-10 in the lens fiber cells can alter the fate of the nearby corneal epithelial cells and can lead to the formation of ectopic lacrimal tissues within the cornea.24 The iris and ciliary body are derived from mesenchyme, which extends forward into the space between the lens and the surface ectoderm, giving rise to the cornea, sclera, choroids,25 and the adjacent neuroderm. Therefore, we presumed that if misexpression of FGF-10 in mesenchyme (which extends forward into the surface ectoderm during embryogenesis) occurs, ectopic lacrimal tissue could possibly develop in the ciliary body derived from this mesenchyme.
The most common presenting clinical finding of intraocular ectopic lacrimal tissue is an abnormal-looking eye noted by parents. Most reported cases have been diagnosed in infants.1,2,4–15 In 4 previous reports, intraocular pressure was raised.7,9,10,14 In our case, the intraocular pressure was within normal range. Some have recommended observation with local resection only if complications such as secondary glaucoma develop,8 others have recommended early surgical removal (iridocyclectomy)10 to prevent glaucoma and visual impairment. In the literature, the treatment was primary enucleation in 6 cases, local surgical removal of the mass in 6 cases, local resection with subsequent enucleation in 1 case, and follow-up after histologic confirmation in 2 cases, including ours.1,2,4–15
Identification of the cause of the ocular mass in childhood is critical, because retinoblastoma, the highly malignant primary retinal cancer, is the most common intraocular tumor. Other causes for an intraocular mass include ocular lymphoma, medulloepithelioma, uveal nevus, and choroidal hemangioma, melanocytoma, choroidal osteoma, and uveal leiomyoma.25
There are several characteristics in differential diagnosis for intraocular mass on CT or MR images. In our case, the peripheral portion of the mass revealed slightly high and low signal intensity on T1- and T2-weighted MR images relative to vitreous and homogenous strong enhancement on gadolinium-enhanced, T1-weighted MR images. Signal intensity of the central portion was suggestive of a cystic component. There was no calcification in the mass on precontrast CT scan. The location of mass was in the superolateral aspect of lens and at the ciliochoroidal region, adjacent to the anterior half of the choroid. These MR and CT findings, and the characteristic location of intraocular ectopic lacrimal tissue, may be useful to differentiate this entity from other ocular masses, in that 1) retinoblastoma is often seen with calcification and a typical retina location, and the cystic aspect of the intraocular lacrimal tissue is not characteristic for retinoblastoma26; 2) primary ocular lymphoma is typically bilateral26; 3) uveal nevus is the most frequently seen in the posterior choroid, is flat in shape, and is for the most part <5 mm in basal diameter25; 4) the features of MR images of uveal melanoma can be similar to our case, but uveal melanomas are seen mostly in adults27; 5) uveal leiomyoma is isointense to brain on both T1- and T2-weighted sequences28; 6) choroidal hemangioma is mainly located in the posterior choroid,27 is characterized by isointensity relative to the vitreous on T2-weighted sequences and shows a centrifugal pattern of enhancement on dynamic enhanced T1-weighted sequences,29 and is typically seen in middle-aged to elderly persons25; 7) medulloepitheliomas can contain cystic changes and calcification30; 8) melanocytoma usually occurs at the optic disk25; and 9) choroidal osteoma appears as a platelike calcified thickening of the posterior choroids, typically in the juxtapapillary region.31
CT and MR imaging provide better resolution compared with ultrasonography, and the extent of the tumor can be further evaluated. MR imaging gives better soft tissue resolution and provides more precise information in determining specific tissue characteristics.
Even though the CT and MR imaging findings are useful in differential diagnosis of ectopic lacrimal tissue from other intraocular tumors, the rarity of ectopic lacrimal tissue is responsible for the fact that it is often incorrectly diagnosed as neoplasm. The differential diagnosis for intraocular ectopic lacrimal tissue is very important because this benign lesion may be incorrectly diagnosed clinically as a malignant tumor and may cause unnecessary treatment. In addition, ectopic lacrimal gland may result in benign cystic lesion of the orbit3 or neoplastic transformation of ectopic lacrimal tissue to pleomorphic adenoma and adenocarcinoma.1,32 Therefore, surgical biopsy and histologic confirmation of the orbital lesion may be necessary even though MR imaging could play a role in differential diagnosis.
References
- Received September 15, 2005.
- Accepted after revision November 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.