
Abstract
SUMMARY: Congenital absence of the major salivary glands is an infrequent disorder. Clinically, patients may be asymptomatic or may present with dryness of the mouth, difficulty in chewing and swallowing, and dental caries. The absence of the submandibular gland may be associated with hypertrophy of the contralateral submandibular gland. We report a case of ipsilateral sublingual hypertrophy associated with unilateral submandibular aplasia.
Congenital absence of the salivary glands is an infrequent disorder, which has been described to affect the parotid or submandibular glands. Congenital absence of a major salivary gland is associated with multiple other developmental anomalies, especially in the face.1,2 Clinically, patients may be asymptomatic or may present with dryness of the mouth, difficulty in chewing and swallowing, and dental caries.3,4 The most common pattern seen is absence of the submandibular gland, which may be associated with hypertrophy of the contralateral submandibular gland.1–4 We report a case of incidentally detected unilateral submandibular gland aplasia, with ipsilateral sublingual gland hypertrophy mimicking a mass, demonstrated on CT and MR imaging. To the best of our knowledge, this is the first report of ipsilateral sublingual hypertrophy associated with unilateral submandibular aplasia.
Case Report
A 35-year-old woman who had facial pressure and rhinorrhea was referred by her internist for a CT scan of the paranasal sinuses to evaluate possible recurrent sinusitis. Apart from extensive mucosal disease, the CT also demonstrated incidental absence of the right submandibular gland, with a “mass” in the right sublingual space in the expected location of the right sublingual gland (Fig 1A, -B). There were no calculi or other lesions, and the mass was above the mylohyoid muscle. The possibility of hypertrophy of the ipsilateral sublingual gland was considered. Other differential diagnoses included an inflamed sublingual gland, postinflammatory enlargement, or a benign minor salivary gland tumor such as a benign mixed tumor. Squamous cell carcinoma of the floor of the mouth was also considered but was thought unlikely because of the low attenuation of the lesion.

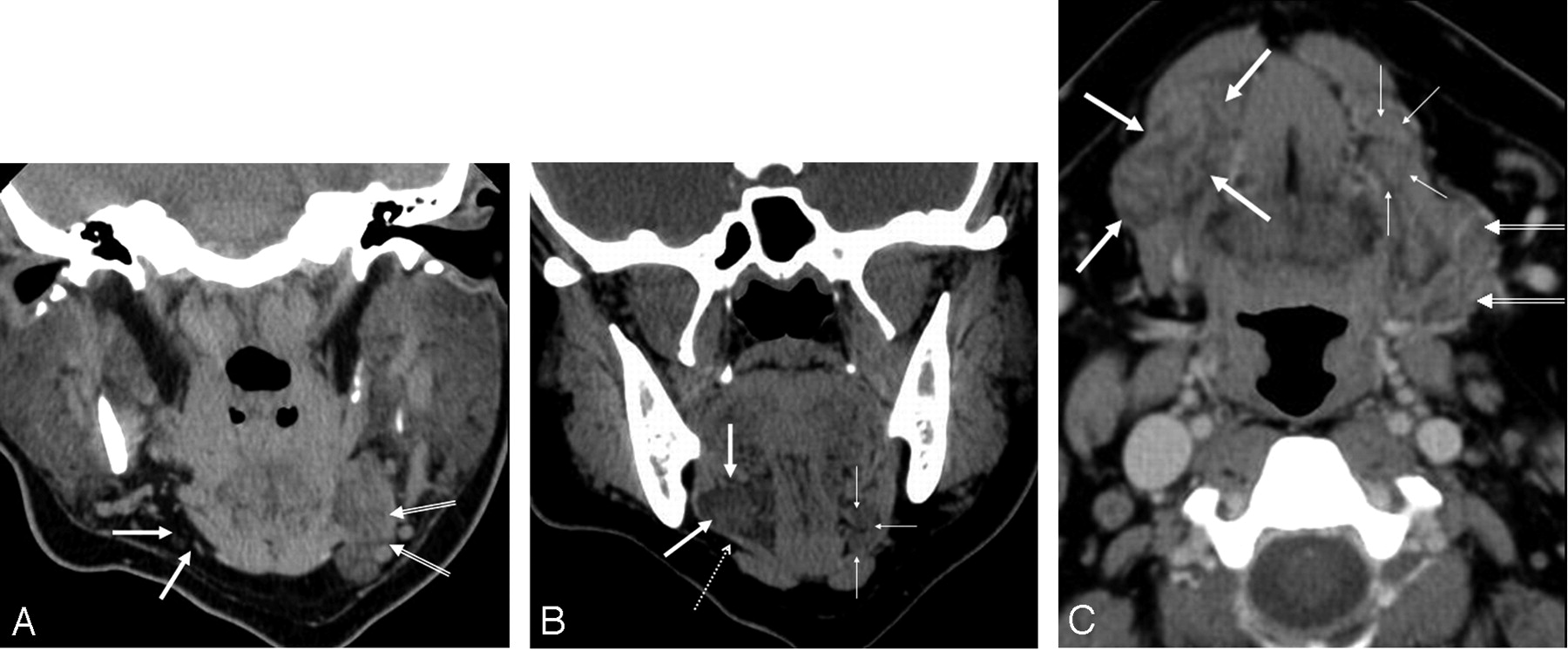
A, Coronal noncontrast maxillofacial CT image reveals absence of the right submandibular gland (broad arrows). The contralateral submandibular gland is visualized in the left submandibular space (double arrows).
B, Coronal noncontrast maxillofacial CT image shows a well-defined low-attenuation mass (broad arrows) in the right sublingual space located lateral to the genioglossus-geniohyoid complex and bowing the mylohyoid inferiorly (dotted arrow). The normal left sublingual gland is visualized in its expected location (thin arrows).
C, Axial contrast-enhanced CT image demonstrates a low-attenuation mildly enhancing mass in the right sublingual region (broad arrows). The contralateral submandibular gland (double arrows) shows attenuation characteristics similar to those of the mass. The normal left sublingual space is also demonstrated (thin arrows).
The patient was referred to an otorhinolaryngologist for further assessment. Her history was unremarkable except for very occasional dysphagia. Clinical examination of the oral cavity and oropharynx did not reveal any palpable masses. There was no palpable neck adenopathy, and indirect laryngoscopy showed a normal larynx with mobile cords and a clear base of the tongue.
She underwent a contrast-enhanced neck CT, which revealed that the mass enhanced, with the degree of enhancement similar to that of the contralateral submandibular gland (Fig 1C). The margins of the mass were well defined, and there was no evidence of invasion of the adjacent soft tissue or inner cortex of the mandible.
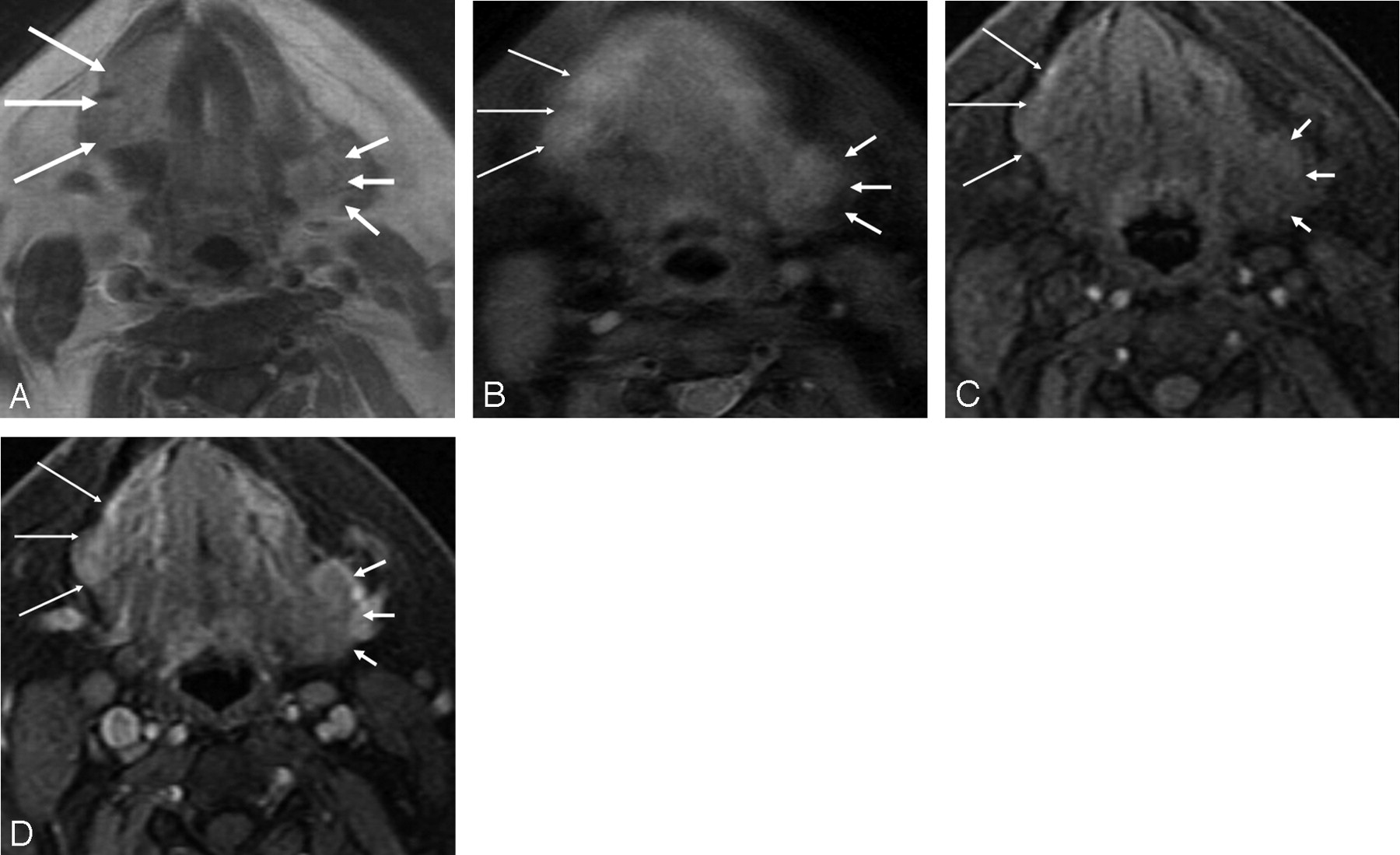
Contrast-enhanced MR imaging was performed for further characterization. The study demonstrated that the sublingual mass had T1-weighted (Fig 2A) and T2-weighted (Fig 2B) signal intensity characteristics similar to those of the contralateral submandibular gland. The dynamic contrast-enhanced MR images showed that the enhancement of the mass was similar to that of the contralateral sublingual and submandibular glands (Fig 2C, -D). On the basis of these findings, the imaging results were thought to be indicative of asymmetric sublingual gland hypertrophy.

The right sublingual mass (long arrows) reveals similar signal intensity similar to that of the contralateral submandibular gland (short arrows) on axial spin-echo nonenhanced T1-weighted (A) and fat-saturated T2-weighted (B) images. Dynamic contrast-enhanced fat-saturated gradient-echo images (C and D) reveal the enhancement pattern of the mass (long arrows) to be similar to that of the left submandibular gland (short arrows).
Discussion
The salivary glands arise as buds from the epithelial lining of the oral cavity. These primordial buds grow and extend into the underlying mesenchymal tissue as a solid core of cells. The developing tissue then undergoes extensive branching and eventually develops lumina. The glands are divided into lobules by the surrounding mesenchyme, which also envelopes them to form a capsule. The parotid glands appear during the fourth week of gestation in the angle between the maxillary process and the mandibular arch. The submandibular glands appear in the sixth week, and the sublingual glands arise during the ninth week between the tongue and the mandibular arch.5–7
Congenital absence of the salivary glands is infrequent and more often involves multiple major salivary glands.1,2 Isolated unilateral major salivary gland aplasia is a rare entity with only a few cases reported in the literature to date.4,8–10 The aplasia is likely due to arrest in organogenesis, but the exact etiology is unknown.9 The unique feature of our patient is the demonstrable ipsilateral sublingual gland hypertrophy associated with the submandibular gland aplasia, which, to the best of our knowledge, has not been reported previously.4 The enlargement of the sublingual gland is likely due to compensatory hypertrophy.
Salivary gland aplasia may be associated with first branchial arch defects in the Treacher-Collins syndrome (mandibulofacial dysostosis) or orbital abnormalities like lacrimal hypoplasia, canalicular atresia, and absence of the lacrimal puncta.1,2,11,12 Absence of salivary glands may also be seen as part of the lacrimoauriculodentodigital syndrome, characterized by hypoplasia, aplasia or atresia of the lacrimal system, deafness and ear malformations, and dental and digital anomalies.13 In our patient, there were no such associated anomalies.
The clinical picture of patients with salivary gland aplasia is variable. They may be asymptomatic or may complain of dry mouth, have difficulty in chewing and swallowing, and have an increased incidence of dental caries, which is thought to be due to reduction of the protective effect of saliva within the oral cavity.1,6,14 Our patient presented with symptoms of recurrent sinusitis, and a detailed history revealed only occasional dysphagia, with no other symptoms related to the gland aplasia. Her relative lack of salivary gland–related symptoms was presumably due to the unilateral nature of the aplasia, with the other major salivary glands being present, and compensatory hypertrophy of the ipsilateral sublingual gland.
Salivary gland aplasia can be diagnosed with a variety of imaging techniques, which include CT, MR imaging, sonography, sialography, or nuclear medicine (technetium T99m-pertechnetate) studies.1,2,4,6,10,15–18 In our patient, we were able to confirm the diagnosis of compensatory sublingual gland hypertrophy by using a combination of CT and MR imaging, including dynamic contrast-enhanced sequences. The imaging findings confirmed the presence of a hypertrophied sublingual gland in association with the absence of the ipsilateral submandibular gland and excluded a floor of the mouth tumor. Radiologists should be familiar with this entity and its imaging findings to prevent unnecessary biopsy of this benign condition.
References
- Received October 12, 2005.
- Accepted after revision November 9, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Unilateral submandibular gland aplasia with contralateral hypertrophy: an unusual neck mass
- CT and MR findings of bilateral submandibular gland aplasia associated with hypertrophied symmetrical sublingual glands herniated through mylohyoid defects
- Bilateral submandibular gland aplasia with clinico-radiological mass due to prolapsing sublingual salivary tissue through mylohyoid boutonniere: a case report and review