
Abstract
BACKGROUND AND PURPOSE: Z-axis automatic exposure control (AEC) technique automatically adjusts tube current based on size of body region scanned. The purpose of the current study was to compare diagnostic acceptability, noise, and radiation exposure of multidetector row CT (MDCT) of neck performed with z-axis AEC and with fixed current.
MATERIALS AND METHODS: Two study groups of 26 patients each underwent MDCT of neck using z-axis AEC with 8 noise index (NI), 150–440 mA, and 10 NI, 75–440 mA, respectively. A control group consisting of another 26 patients underwent MDCT of neck with fixed-current technique (300 mA). Objective noise and mean tube current-time products (mA · s) were recorded. Two radiologists evaluated images for diagnostic acceptability and subjective noise on a 5-point scale.
RESULTS: All CT examinations of study and control groups were diagnostically acceptable, though objective noise was significantly more with z-axis AEC (shoulder: NI 8, 20.6 ± 6.2 HU; NI 10, 22.2 ± 4.6 HU) than with fixed current (16.2 ± 6 HU) (P = .01). There was no significant difference between AEC and fixed current in diagnostic acceptability and subjective noise (P = .22–.42). AEC resulted in significant radiation dose reduction (NI 8, 186.3 ± 20.5 mA · s; NI 10, 158.1 ± 21.2 mA · s), compared with fixed current (235 ± 21.8 mA · s).
CONCLUSION: Z-axis AEC resulted in similar subjective noise and diagnostic acceptability, with radiation dose reduction of 21% for NI of 8 and 33% for NI of 10, respectively, for MDCT evaluation of neck, compared with those of fixed current technique.
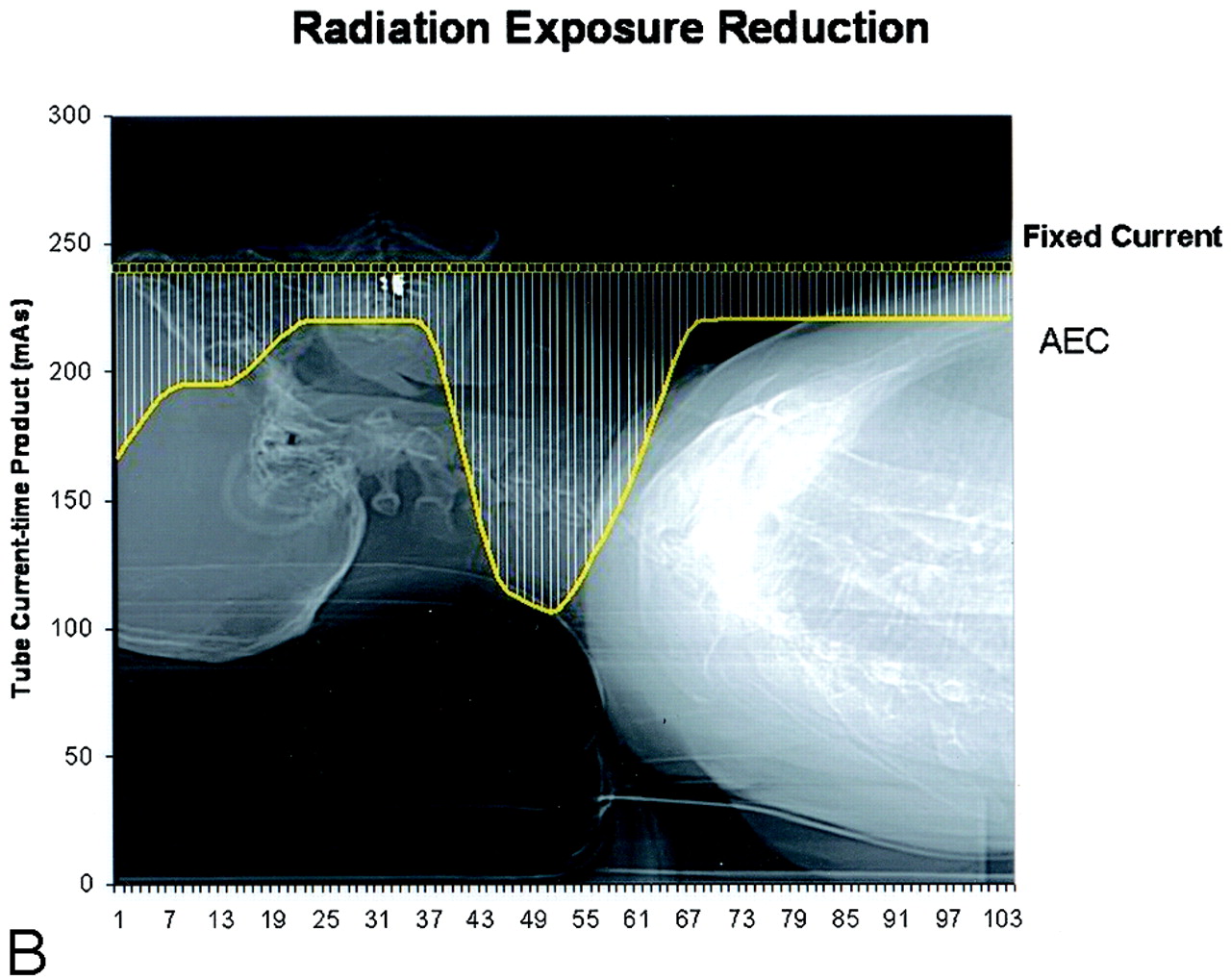
Increasing awareness of risks associated with radiation exposure mandates lowest possible radiation exposure to patients from CT studies while maintaining optimum image quality.1 However, choosing appropriate scanning parameters to maintain optimum diagnostic acceptability of images at low radiation exposure is technically challenging because of recent advances in the multidetector row CT (MDCT) technology.2,3 The most practical way to reduce CT radiation dose is to reduce tube current.2,4 A recent technologic innovation for automatic tube current adaptation to patient size in CT is the availability of automatic exposure control (AEC). AEC performs automatic adjustment of tube current in the x-y plane (angular modulation) or along the z-axis (z-axis modulation) depending on the width and attenuation characteristics of the body part scanned (Fig 1A, -B), to achieve optimum image quality throughout the scan volume with optimum radiation exposure.4


Graphs illustrate schematic representations of the modulation of tube current (A) and, hence, tube current-time product (mA · s) (B) with body region along z-axis in automatic exposure control (AEC) technique (continuous lines in A and B). Tube current and tube current-time products in fixed current technique is shown for comparison as dotted lines in A and B, respectively. Radiation dose (mA · s) with AEC is less than that with fixed current in all section positions along z-axis.
The z-axis AEC (AutomA; General Electric Healthcare Technologies, Waukesha, Wis) used in our study determines the width of the body part and its attenuation on the localizer radiograph. The user specifies the minimum and maximum current thresholds (milliampere range), and the desired noise index (NI). NI represents the quantum noise (image noise level) specified by the user based on which AEC will adjust the tube current settings within the specified milliampere range. Choosing a high NI results in more image noise and less radiation dose and vice versa.5 Several other vendors have also introduced z-axis AEC for CT scanners (Real E.C., Toshiba Medical Systems, Tokyo, Japan; z-axis exposure control [ZEC], Siemens Medical Solutions, Forchheim, Germany). The purpose of this study was to compare the diagnostic acceptability, noise, and radiation exposure associated with 16-section MDCT examination of extracranial head and neck performed with z-axis modulation technique AEC and with fixed current.
Materials and Methods
Study Subjects and Scanning Parameters
Our institutional review board approved the study protocol. The need for consent was waived. Our study was in compliance with the Health Insurance Portability and Accountability Act (HIPAA).
A study group composed of 52 consecutive subjects referred for contrast material–enhanced MDCT examination of neck. All subjects were scanned with a 16-section MDCT (LightSpeed 16; General Electric Healthcare Technologies) using 120 kV peak (kVp) tube voltage, 0.938:1 beam pitch, 16 × 1.25-mm detector configuration, 18.75-mm table feed per gantry rotation, and 0.5-second gantry rotation time. Images were reconstructed with 2.5-mm section thickness and 2.5-mm reconstruction interval using a standard reconstruction algorithm.
CT was performed using z-axis AEC (AutomA, GE Healthcare Technologies) with a range of 150–440 mA, and 8 NI in the first subgroup of 26 consecutive subjects (mean age, 49 years; age range, 19–81 years; 9 men, 17 women). In the next subgroup of 26 consecutive subjects (mean age, 53 years; age range, 21–78 years; 19 men, 7 women), a range of 75–440 mA for AEC, and 10 NI were used. A control group composed of 26 consecutive subjects (mean age, 56 years; age range, 24–68 years; 17 men, 9 women) who underwent contrast-enhanced MDCT of the neck using a fixed tube current of 300 mA with a 0.8-second (n = 23) gantry rotation time or 330 mA with 0.6-second (n = 3) gantry rotation time. The remaining scanning parameters were held constant as in the study group.
Image Analysis
All image datasets were transferred to a standalone postprocessing workstation (Advantage 4.2, GE Healthcare Technologies). Two radiologists, each with more than 4 years of experience, independently graded the studies for subjective image noise (graininess or mottle in images) and diagnostic acceptability using a 5-point scale (1, unacceptable; 2, below average; 3, average; 4, above average; 5, excellent) to score images at 2 anatomic levels, including upper neck (level of angle of the mandible), and shoulder (level of sternal notch). Subjective image noise was considered average when there was moderate amount of graininess, and satisfactory visualization of small anatomic structures, such as blood vessels, and the interface between structures of variable attenuation. Unacceptable image noise was defined as image graininess that interfered with visualization of these structures. Excellent image noise was defined on the basis of minimal or no appreciable graininess in the image. Diagnostic acceptability was graded depending on the confidence in detecting lesions, which is usually determined by soft tissue contrast, sharpness of tissue interfaces, lesion conspicuity, and degree of image degradation by streak or beam-hardening artifacts. A score of greater than or equal to 3 was considered acceptable noise or adequate diagnostic acceptability.
Objective image noise was measured by placing a circular region of interest cursor (100 mm2) over arbitrarily selected anatomic landmarks including sternocleidomastoid, and pectoralis major muscle at upper neck, and shoulder level, respectively. Objective image noise represents the standard deviation of CT attenuation in Hounsfield units (HU) recorded by drawing a region of interest cursor over a body part in the image. To compare patient size in study and control groups, 2 measurements were used. Scan coverage (a reflection of patient size) and transverse neck diameters of all subjects at the level of upper neck (across anterior surface of cervical vertebral body) were recorded.
Radiation Dose
To compare radiation exposure with AEC and fixed tube current techniques we used tube current-time product. As z-axis AEC changes tube current for different section locations, we recorded tube current (milliamperes) for each image of all patients in the study group. The mean tube current in each subject in the study group was calculated by averaging the tube current on each image. The mean tube current-time product (mA · s) was calculated for each examination in the study group by multiplying the mean tube current by the gantry rotation time. For control subjects, the fixed tube current was multiplied by gantry rotation time to calculate the tube-current time product.
Statistical Analysis
Image quality scores for subjective noise and diagnostic acceptability in the 2 AEC subgroups versus fixed current group were compared using the Kruskal-Wallis test (SPSS version 13.0; SPSS, Chicago, Ill). Objective noise of 2 subgroups of AEC and fixed current group were compared by analysis of variance. In case of a significant difference between means, Tukey pair-wise multiple comparison was performed to determine which means differ. Mean tube current-time products for examinations performed with either NI, AEC were compared with those performed using fixed current with the use of the unpaired t test. The degree of interobserver concordance was determined by calculation of κ statistic. A P value of less than 0.05 was considered to indicate a statistically significant difference.
Results
The age and sex distribution of the subjects in the 3 groups was comparable (P = .49, P = .85). The scan coverage (264.8 ± 29.8, 270.4 ± 27, and 259 ± 23.8 mm), and transverse neck diameters (137.4 ± 12.7, 132.9 ± 16.3, and 135.4 ± 17.3 mm) of the 2 study groups and the control group were not significantly different (P = .23–.73). None of the studies required a repeat CT study as a result of unacceptable image quality.
Image Quality
Table 1 illustrates the subjective noise and diagnostic acceptability scores of the study and control groups. All subjects (100%, 52/52) had acceptable noise at upper neck level in both AEC subgroups according to both readers (Fig 2). Both readers reported below average noise (score 2) at upper neck level in a subject in the fixed current group. Reader 1 reported below average noise at shoulder level for the NI 8 and NI 10 subgroups, and fixed current groups in 3 (12%, 3/26), 2 (8%, 2/26), and 3 (12%, 3/26) subjects, respectively (Figs 3 and 4). Likewise, reader 2 reported the same in 2 (8%, 2/26), 3 (12%, 3/26), and 2 (8%, 2/26) patients, respectively. The subjective noise scores at upper neck and shoulder levels were not significantly different across the 3 groups (P = .22–.31). All studies in both study and control groups were diagnostically acceptable, except for suboptimal study for diagnostic acceptability in 1 subject in the fixed current group. The overall diagnostic acceptability was comparable across the 3 groups (P > .05) for both readers.

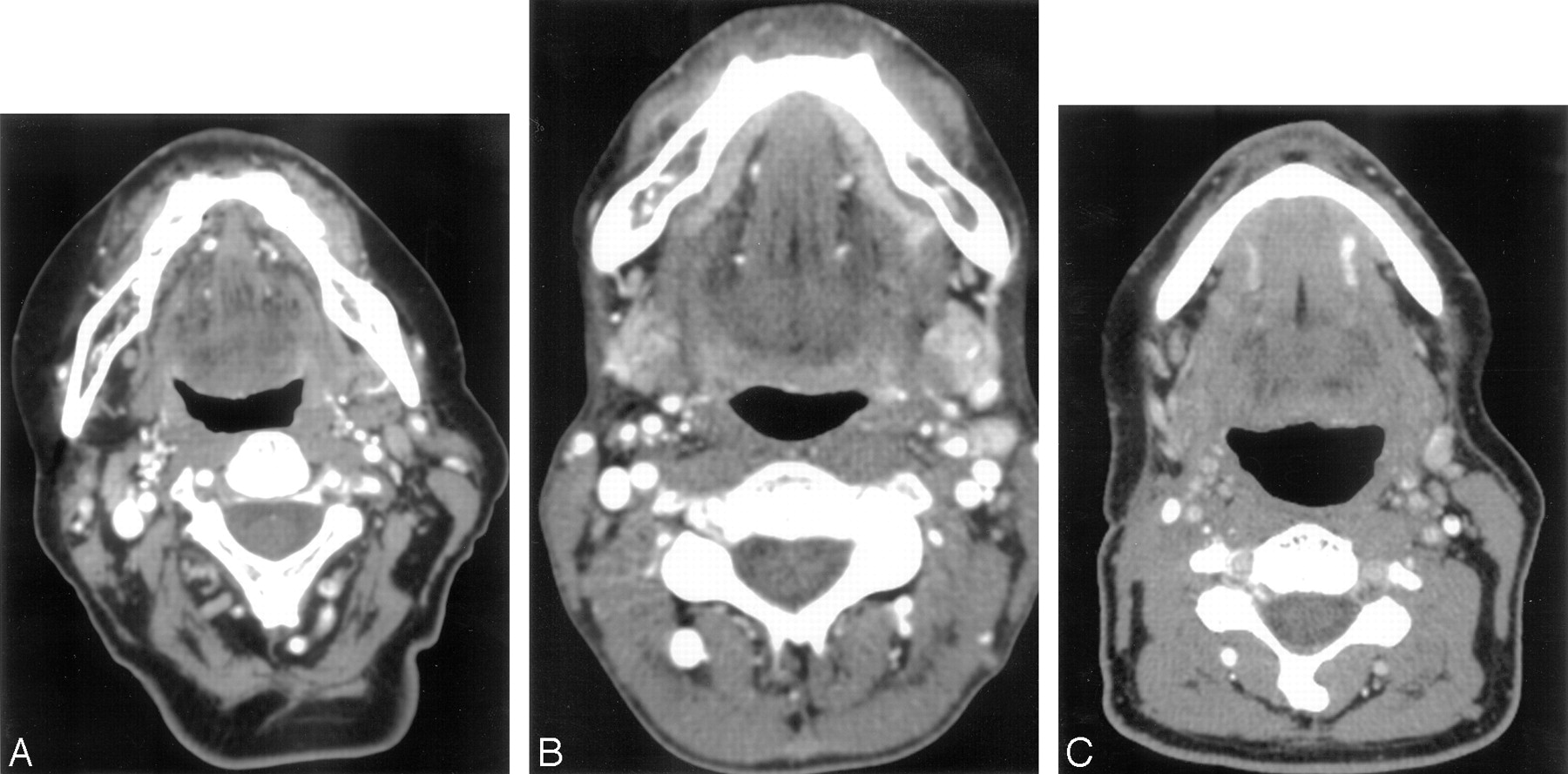
Multidetector row CT evaluation of extracranial head and neck. Transverse image through upper neck using fixed current (A), z-axis automatic exposure control (AEC) with noise index 8 (B), and noise index 10 (C). The subjective noise and diagnostic acceptability of the 3 techniques are comparable.

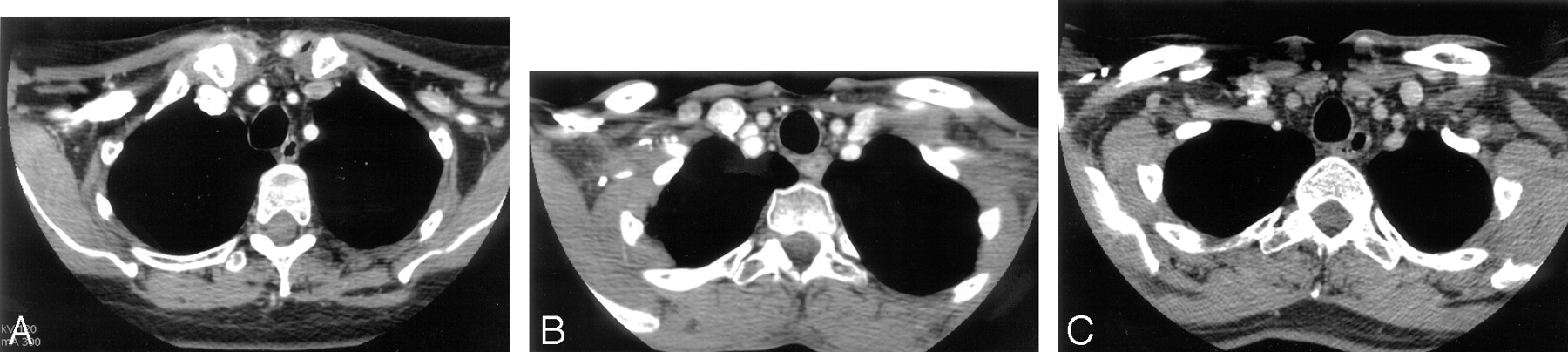
Multidetector row CT evaluation of extracranial head and neck. Transverse image at the level of shoulders using fixed current (A), z-axis automatic exposure control (AEC) with noise index 8 (B), and noise index 10 (C). The subjective noise and diagnostic acceptability of the 3 techniques are comparable.

Multidetector row CT evaluation of extracranial head and neck. Transverse CT images of fixed current (A) and z-axis automatic exposure control (AEC) with noise index 8 (B) and noise index 10 (C) at the level of the shoulders, illustrating suboptimal subjective noise and diagnostic acceptability.
Distribution of suboptimal and acceptable image quality scores in the study and control groups
Table 2 shows the objective noise at upper neck and shoulder in the study and control groups. Objective noise at upper neck is comparable in both subgroups of AEC (NI 8, 7 ± 1.2 HU; NI 10, 6.9 ± 1.2 HU, P = .99). However, the mean noise measurements at upper neck with AEC groups are slightly more compared with the fixed current group (5.9 ± 2.1 HU), which was statistically significant (NI 8, P = .034; NI 10, P = .04). Likewise, noise measurements at shoulder level were significantly greater with AEC subgroups (NI 8, 20.6 ± 6.2 HU, P = .01; NI 10, 22.2 ± 4.6 HU, P = .01), compared with the fixed current group (16.2 ± 6 HU). However, the noise measurements in the 2 AEC subgroups were comparable (P = .6).
Objective noise at upper neck and shoulder levels, and mean tube current-time product (mAs) in the study and control groups
Radiation Dose
The mean tube current-time product for the 3 scanning techniques is listed in Table 2. When AEC technique was used, overall mean tube current–time product (mA · s) reduction was 21% (range, 7%–51%) and 33% (range, 11%–51%) with NI of 8 and 10, respectively, compared with those scanned with fixed current technique. The use of z-axis AEC resulted in a reduction in tube current–time product in all subjects (100%, 52/52) compared with those scanned with fixed current technique. Compared with the fixed tube current group, mean tube current time-product in both AEC groups was significantly low (P < .001). Furthermore, use of NI 10 resulted in additional radiation dose reduction by 12% compared with NI 8 (P < .001).
Interobserver Agreement
The 2 readers had substantial interobserver agreement for both image noise and diagnostic acceptability (κ coefficient, 0.68; P < .05).
Discussion
Recent advances in MDCT technology increased the number of CT examinations by approximately 100% during the last decade of the 20th century.6 However, risks of radiation exposure raise concern. A recent study has reported increased relative risk of cancer mortality among atom bomb explosion survivors, who were exposed to 50–150 mSv radiation dose.7 Furthermore, the National Institute of Environmental Health Sciences (NIEHS) has recently declared low energy x-ray and gamma radiation to be known human carcinogens in the 11th edition of its Report on Carcinogens.8 In large hospitals, CT scanning now accounts for approximately 15% of procedures and 75% of the diagnostic radiation dose received by patients.9
Many technologic innovations have been introduced in the modern state-of-the-art CT scanners for radiation dose reduction. AEC represents the most critical development in CT technology for optimizing radiation exposure. Published reports on clinical application of AEC are encouraging. A prior study reported 33% mean tube current-time product reduction with similar noise and diagnostic acceptability for abdominal and pelvic CT using z-axis AEC compared with fixed current technique.10 Radiation dose reduction of 56%–77% has been reported for urinary tract stone CT studies with the use of z-axis AEC without compromising stone depiction.11 Another study reported 18%–26% radiation dose reduction for chest CT study using z-axis AEC.12 Mulkens et al13 compared the radiation dose reduction and image quality of combined angular (x-y axis) and z-axis tube current modulation with angular tube current modulation alone.13 They reported a radiation dose reduction of 68% and 16% with combined modulation and angular modulation alone, respectively. Mastora et al14 evaluated the on-line tube current modulation technique (Siemens Medical Systems) for CT study of the thoracic outlet. They reported a 35% reduction in mean tube current-time product without loss of image quality when a preset minimum dose saving of 20% was used. To the best of our knowledge, in no previous peer-reviewed scientific study has there been a comparison of z-axis modulation AEC with different noise indices for MDCT evaluation of extracranial head and neck with fixed tube current scanning in adults.
Compared with chest and abdomen, neck CT spans over a body region with wide variations in body size and attenuation pattern. With fixed tube current technique, a low dose CT may have resulted in suboptimal quality images at the shoulders. Conversely, to obtain better image quality at the shoulders, a higher tube current would have resulted in greater exposure of neck region. Because AEC automatically adapts tube current based on size and attenuation of the body region(s), we hypothesized that it will automatically lower the tube current for the neck and increase it for the shoulder region for CT of the neck. Our study confirms this hypothesis (Fig 1A, -B).
We found that the z-axis AEC provides images with acceptable subjective image noise and adequate diagnostic acceptability for MDCT examination of the neck compared with those achieved by the fixed tube current technique. Findings of our study for neck CT are in agreement with the results of AEC reported for CT evaluation of abdomen, pelvis, or chest.10,12 Objective noise at shoulder level is greater than in the upper neck for both AEC and fixed current groups (P < .001). This is explained by the wide and higher beam attenuating shoulders in the scan field. AEC resulted in greater objective noise compared with fixed tube current in both upper neck and shoulder levels (P = .01). However, all studies performed with AEC resulted in acceptable image quality. If the shoulders are the primary area of interest, better image quality with AEC at the shoulders can be obtained by choosing a higher tube current (mA) range, longer gantry rotation time, or a smaller noise index. Although we did not increase tube current to more than 440 mA or gantry rotation time beyond 0.5 seconds, to limit the radiation exposure to thyroid gland, we found that all studies were diagnostically acceptable.
From a radiation dose reduction perspective, in comparison with the fixed tube current technique, z-axis AEC resulted in reduction of 21% (range, 7%–51%) and 33% (range, 11%–51%) mean-tube current time product with NI 8 and 10, respectively. Our study protocol was associated with greater radiation dose reduction for adults than reported by Greess et al15 (12%) for neck CT of children. As expected, in the current study, with increase in NI from 8 to 10, there was further reduction in radiation exposure by another 12%. Our observation is consistent with a prior report of increase in radiation dose reduction from 16%–55% with increase in NI from 10.5 to 15 for abdominal and pelvic CT.5
It is important to note that we lowered minimum tube current limit to 75 mA for NI 10 (as reported in AutomA studies for abdominal CT),5 as image quality at NI 8 with 150 mA was acceptable. Because tube current lower than 150 mA was recorded with NI 10, we believe that reduction of minimum tube current to 75 mA was appropriate for neck CT to achieve further radiation dose reduction.
An important consideration in our study is that we used mA · s to compare radiation dose associated with the use of 3 different CT techniques. However, there is a strong linear relationship of mA · s with radiation dose, when the other scanning parameters, including kilovolt peak, tube rotation time, pitch, and section thickness are kept constant.2,16 Indeed, several studies on AEC have used mA · s to compare radiation dose associated with use of AEC and fixed tube current technique.5,10,12
There are some limitations in the present study. Although our study demonstrated a reduction in mean tube current–time product in neck CT examinations performed with z-axis AEC, a similar study with a larger study cohort and greater range of noise index values may be required to suggest a patient-based NI value for further radiation dose reduction. Our study did not include comparison of standard radiation dose indices like CT dose index, dose length product, or estimated effective dose with AEC and fixed tube current techniques. However, when other scanning parameters are kept constant, the mean tube current-time product can serve as a valid radiation dose indicator for comparison between techniques.10,12 We evaluated the z-axis AEC technique of a single vendor only. However, tube current modulation programs of the other vendors function based on similar principles. Another limitation of our study was that we did not correlate the noise, image quality, and radiation exposure with patient weight and transverse neck diameter. However, we believe that such correlation must be assessed in a larger study population.
Conclusions
In summary, z-axis AEC results in similar diagnostic acceptability and subjective image noise for MDCT evaluation of extracranial head and neck compared with those scanned with fixed current technique. Objective noise is slightly more with z-axis AEC at shoulder level. Radiation exposure reduction was 21% for NI of 8 and 33% for NI of 10 for z-axis AEC, whereas subjective image noise and diagnostic acceptability are similar, compared with those scanned with fixed tube current technique. Based on the present study results, we recommend using NI 10 with tube current thresholds of 75–440 mA for MDCT evaluation of extracranial head and neck.
References
- Received November 23, 2005.
- Accepted after revision January 29, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Low Kilovoltage CT of the Neck with 70 kVp: Comparison with a Standard Protocol
- Image Quality and Radiation Dose of Dual-Energy CT of the Head and Neck Compared with a Standard 120-kVp Acquisition
- Radiation dose evaluation in multidetector-row CT imaging for acute stroke with an anthropomorphic phantom
- Optimal Use of AEC in CT: A Literature Review
- Comparison of Image Quality and Radiation Dose between Fixed Tube Current and Combined Automatic Tube Current Modulation in Craniocervical CT Angiography