
Abstract
SUMMARY: We present a patient with double spinal dural arteriovenous fistulas revealed by progressive myelopathy. Numerous dilated veins extending along the entire length of the spinal cord were found on MR imaging. Angiography showed a first spinal dural fistula at the level of T7 with descending venous drainage and a second spinal dural fistula at the level of T5 with ascending venous drainage. Both fistulas were cured by therapeutic embolization.
Spinal dural arteriovenous fistulas (SdAVFs) are vascular malformations comprising an arteriovenous shunt located within the spinal dura.1,2 They are encountered predominantly in middle-aged and elderly men and are often revealed by a slowly progressive and ascending myelopathy.3,4 SdAVFs are acquired lesions of unknown etiology.5 We present a patient with 2 separate SdAVFs at the time of presentation who underwent endovascular treatment (EVT).
Case History
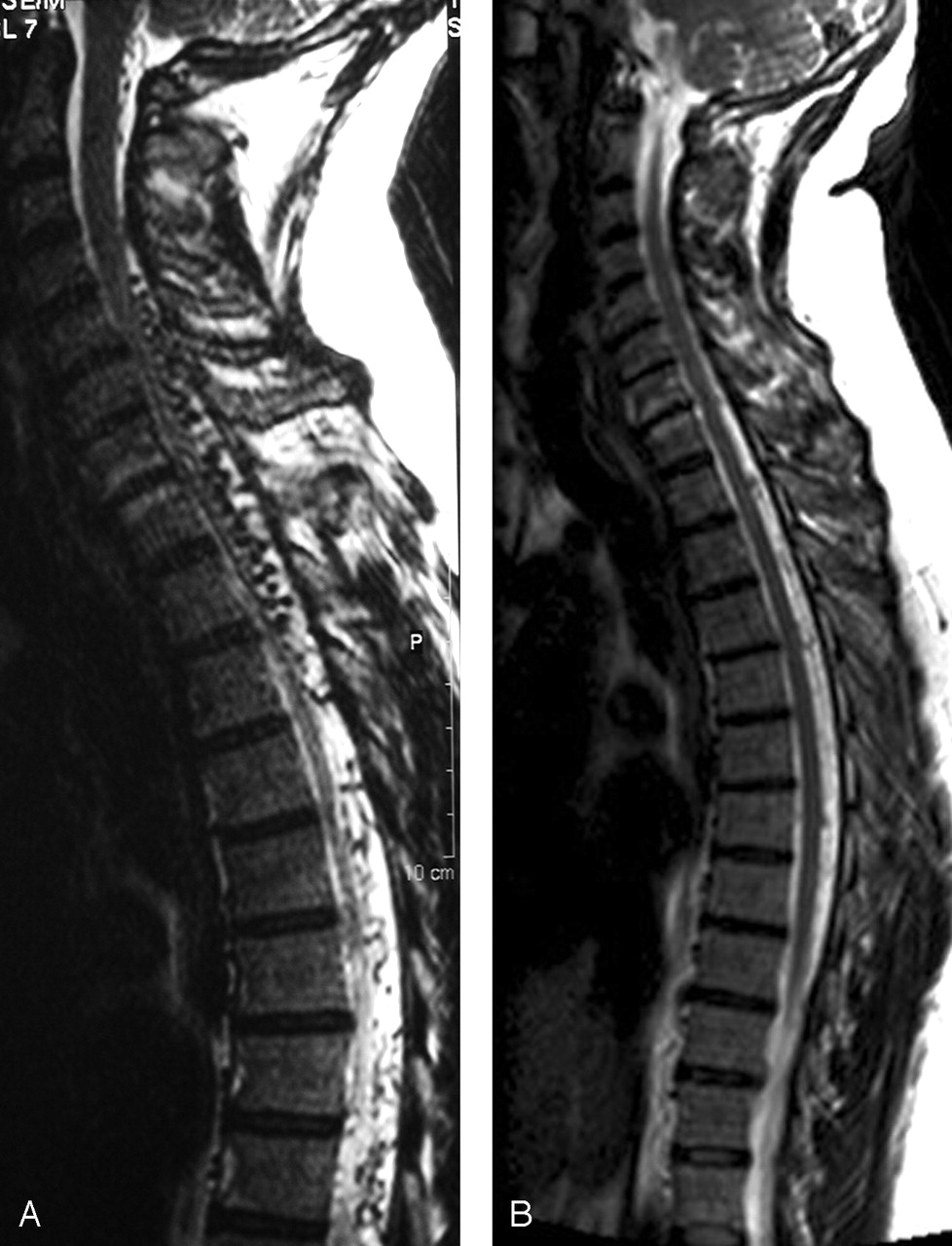
A 47-year-old man presented with progressive weakness of both lower limbs for the past 9 months and recent sphincter dysfunction. MR showed abnormal vessels appearing as flow voids on the posterior aspect of the whole spinal cord, from the level of T12 up to C4 (Fig 1A).

A, MR showing flow voids in abnormal dilated vessels extending from T12 to C4 along the spinal cord.
B, Control MR 8 months after therapeutic embolization showing marked regression of the dilated vessels.
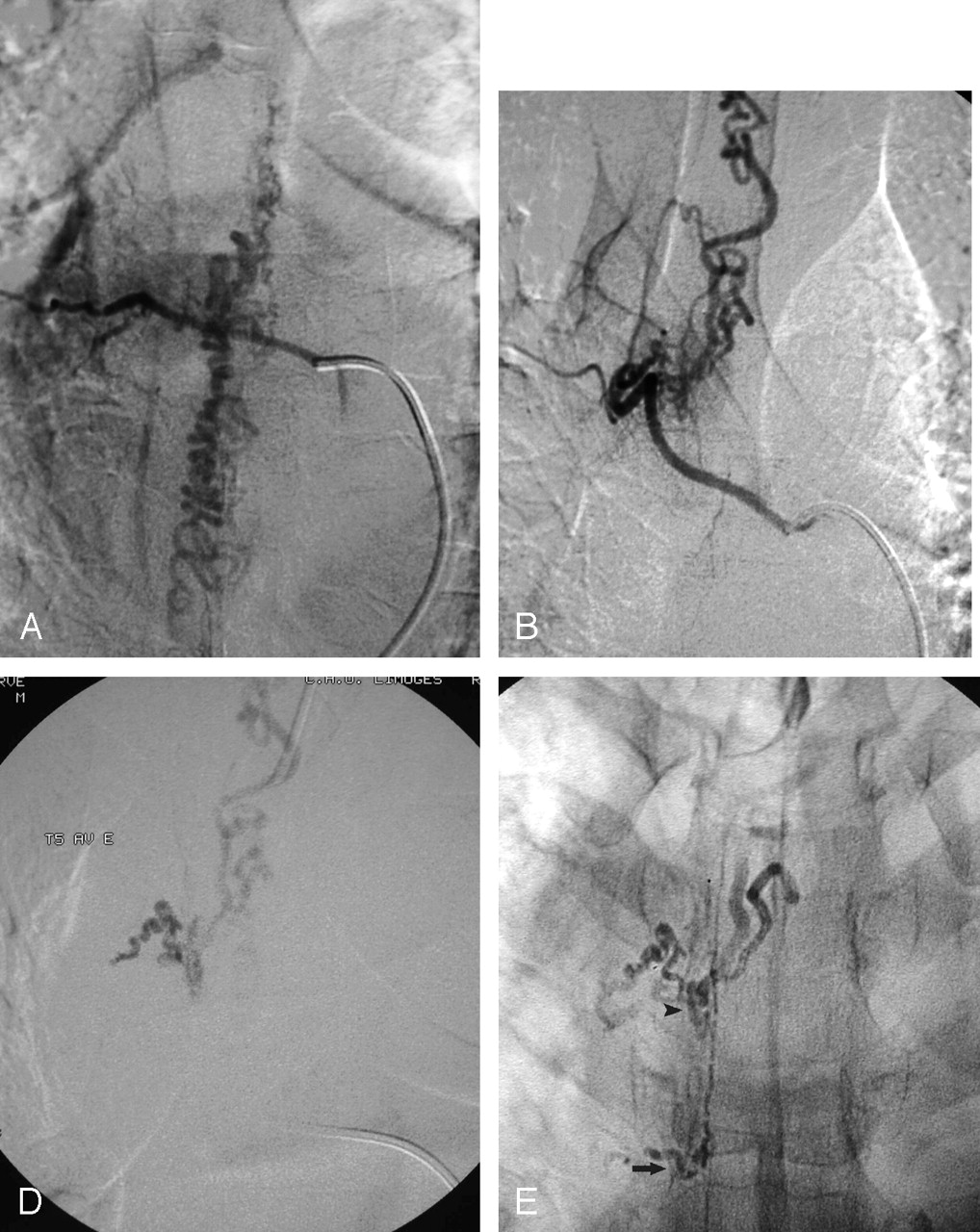
Spinal angiography confirmed a SdAVF at T7 level fed by right T7 intercostal artery and indirectly from an anastomosis with the right T8 intercostal artery. Lateral projection showed that the point of shunt was located anterior to the spinal cord. The venous drainage was found to be descending (Fig 2A). Because MR imaging showed flow voids at the cervical level and no ascending veins were found, angiography was continued. A second SdAVF was found at the level of T5, on the dura mater located anterior to the spinal cord, fed mainly by the right T5 intercostal artery and indirectly by the right T4 intercostal artery. This second fistula showed ascending venous drainage with a medullary outflow by a radicular vein at the level of C6 (Fig 2B).


A, Selective angiogram of the right seventh intercostal artery showing the inferior SdAVF with a descending venous drainage.
B, Selective angiogram of the right fifth intercostal artery showing the superior SdAVF with an ascending venous drainage.
C, Selective angiogram of the right fourth intercostal artery after treatment of the inferior SdAVF. The venous drainage changed from exclusively ascending to both ascending and descending. The upper thoracic anterior spinal artery is visualized (arrow).
D, Superselective catheterization of the meningeal feeders from the fifth intercostal artery before injection of acrylic glue.
E, Casts of n-BCA at the level of T7 (arrow) and T5 (arrowhead), involving the origin of the draining veins, which enabled definite cure.
Indirect feeders to both fistulas also gave rise to anterior spinal arteries that were found at the level of T8 on the right side for the inferior spinal artery injecting the conus medullaris and at the level of T4 on the right side for an upper thoracic anterior spinal artery.
Embolization was decided as primary treatment technique due to anterior location of the point of shunt and despite the close location of the spinal arteries. The initial goal of treatment was the inferior SdAVF at the level of T7, because the descending venous drainage was considered responsible for the clinical symptoms.
Selective catheterization of the T7 fistula feeding artery was achieved by using a Spinacker-Elite 1.5F microcatheter (Target; Boston Scientific, Fremont, Calif) to obtain a wedged flow condition. A mixture of n-butyl cyanoacrylate (n-BCA) (Glubran2; GEM, Viareggio, Italy)-Lipiodol Ultra Fluide (Guerbet, Roissy, France) at a 1:4 ratio enabled occlusion of the fistula with extension of glue in the first centimeters of the draining vein. Control injections of the neighboring intercostal arteries confirmed complete disappearance of this fistula.
Clinically, the patient noted no significant change in the weakness of the legs after this first session of embolization. A second session was therefore scheduled for embolization of the second fistula. Angiography showed a change in the venous drainage that became both ascending and descending after being exclusively ascending (Fig 2C,-D). Selective catheterization of the feeder arising from T5 (Fig 2D) was achieved with a Vasco 10 microcatheter (Balt Extrusion, Montmorency, France). A mixture of glue with Lipiodol at the same ratio as before was injected and reached the initial portion of the draining vein (Fig 2E), totally occluding the fistula.
Clinical symptoms completely resolved within 3 months. Control MR and spinal angiography at 8 months confirmed stable occlusion of both SdAVFs.
Discussion
SdAVFs are the most common spinal vascular malformations.6 The precise etiology for SdAVFs is unknown; they may occur after thrombosis or because of a hypercoagulable state.7 They have been described by Kendall and Logue8 and Merland et al1 as arteriovenous malformations located at the dura mater and draining into medullary veins. The meningeal feeders may arise from various arteries, including intercostal, lumbar, and hypogastric, depending on the level of the SdAVF, which is more frequent at the thoracic and lumbar levels1,2,4 than at the sacral9,10 or cervical level.7 The drainage in the medullary veins leads to venous hypertension with swelling and edema of the spinal cord, inducing progressive neurologic deterioration.11 A similar clinical picture may be seen in intracranial dural fistulas draining exclusively into spinal veins, because of similar medullary venous congestion.12 SdAVF is rarely associated with another vascular malformation. The pathology of SdAVFs may be associated with a medullary arteriovenous malformation in Cobb syndrome, which is a metameric angiomatosis with involvement of the spinal cord, dura mater, vertebrae, muscles, and skin.
MR may suggest the diagnosis of SdAVF by showing spinal cord edema with enlargement of medullary veins. The gold standard is spinal angiography, which confirms the diagnosis and gives the characteristics of the SdAVF before treatment: level of the fistula, anterior or posterior location to the spinal cord, venous drainage, and identification of normal spinal vasculature. When a suspected SdAVF is not found on spinal angiography, an indirect argument for its presence is the absence or delayed appearance of the medullary veins after injection of the anterior spinal artery.13 In cases of normal spinal angiography in a patient with typical clinical and imaging features of SdAVF, cerebral angiogram must also be performed to look for an intracranial dural fistula draining into the medullary veins.12,14
Treatment of the fistula is mandatory because the natural history leads to progressive clinical deterioration. This may be due to progressive occlusion of the normal radicular veins draining the medullary veins.15 Delayed treatment reduces the chances for clinical recovery.13
The goal of treatment is to occlude the primary draining vein, which may be achieved by surgery or embolization.16,17 EVT may be attempted as a primary treatment technique because of its low invasiveness. EVT seems preferable to surgery in cases of difficult surgical location such as the upper thoracic level or an anterior location to the spinal cord. Surgery may be preferred to EVT in cases of neighboring normal spinal arteries that may be occluded during injection of glue. There is a 15%–20% risk of recurrence after EVT18 or surgery, which is mostly due to incomplete treatment. Recurrence is avoided in EVT if the glue reaches the proximal portion of the vein of drainage.18
Multiple SdAVFs have rarely been described: Merland et al19 reported 4 cases with double SdAVFs in a series of 56 patients with a single SdAVF, Pierot et al20 reported 2 patients of 50, van Dijk et al21 reported one patient of 49, and Krings et al22 reported one patient of 129. The estimated frequency of double SdAVF seems therefore to be rare, about 1% or 2%. It has been argued that one SdAVF could cause development of another SdAVF because of elevated pressure, venous stagnation, and subsequent thrombosis.20 MR imaging seems unable to determine whether there is single or double SdAVF, because the fistula itself is not seen; only the abnormal veins of drainage are. The location of these veins may show the level of the SdAVF, but these veins often extend along the entire length of the spinal cord. The diagnosis of all reported double SdAVFs was established on angiography, with a 6-year delay in one patient to diagnose the second fistula.22 In our patient, the diagnosis was established on the initial angiography because of a discrepancy in the venous drainage between MR and angiography. The abnormal veins were seen throughout the entire spinal cord on MR, but the drainage of the inferior fistula involved only the veins at the lower thoracic level. Therefore, angiography was continued, which enabled diagnosis of the superior SdAVF.
EVT was chosen in our patient because of the anterior location of the SdAVF and despite the close location of the spinal arteries. The SdAVF with a descending venous drainage was chosen as the first to be treated because it was the most likely to induce medullary venous congestion; however, the pattern of the venous drainage coming from the second SdAVF changed after treatment of the first SdAVF. It became both ascending and descending, which explains the absence of clinical improvement. Occlusion of the initial portion of the draining veins of both SdAVFs enabled a definite cure, which was confirmed on the follow-up MR and angiography.
Conclusion
Double SdAVF is a rare clinical condition. It may be suspected on the initial angiography when a discrepancy in the venous drainage between MR and angiography is found.
References
- Received October 22, 2004.
- Accepted after revision November 17, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}